
Abstract
Purpose: To compare the timing of administration of morphine in patients undergoing painful ambulatory surgical procedures to determine whether there was a difference in postoperative nausea or vomiting (PONV), quality of analgesia, and recovery profile.
Methods: In a double-blinded, placebo-controlled, prospective study, 70 ASA 1–11 patients were randomized to receive 0.1 mg·kg−1 morphine intraoperatively (lop) (n=35), or postoperatively (Pop) (n=35). The severity of nausea and pain were measured using visual analog scales (VAS).
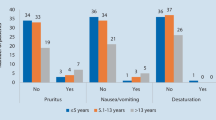
Results: There was no difference between the groups in postoperative nausea scores or the incidence of PONV. Upon awakening, patients who received Pop morphine had higher pain VAS scores with movement (7.6±2 vs 5.4±3,P<0.003) and at rest (6.9±3 vs 5.1±3,P<0.013) than the lop morphine group. The total number of PCA attempts and analgesic requirements were similar. Patients who received Pop morphine were able to drink sooner than the lop group (90±34 vs 111±38 min,P<0.05). All other recovery milestones were similar. Times to discharge from hospital were similar.
Conclusions: Administration of 0.1 mg·kg−1 morphineiv intraoperatively improves postoperative analgesia upon emergence from painful ambulatory surgical procedures without increasing the incidence of PONV. There was no increase in PONV when morphine was administered intraoperatively rather than postoperatively.
Résumé
Objectif: Vérifier si l’incidence de nausées et de vomissements postopératoires (NVPO), la qualité d’analgésie et le profil de récupération est différente selon le moment choisi pour l’administration de morphine lors d’une intervention chirurgicale ambulatoire algique.
Méthode: Une étude prospective et à double insu contre placebo a été menée auprès de 70 patients d’état physique ASA 1–11. On a procédé à l’administration peropératoire (PER) ou postopératoire (POST) de 0,1 mg·kg−1 (n=35 dans chaque groupe). La sévérité des nausées et des douleurs a été mesurée par l’échelle visuelle analogique (EVA).
Résultats: On n’a pas noté de différence intergroupe du score de nausées postopératoires ou d’incidence de NVPO. Au réveil, les patients du groupe POST, comparés à ceux du groupe PER, ont présenté des scores de douleurs plus élevés à l’EVA lors de mouvement (7,6±2 vs 5,4±3,P<0,003) et au repos (6.9±3 vs 5,1±3,P<0,013). Le nombre total de recours à l’ACP et de demandes d’analgésiques a été similaire. Les patients du groupe POST ont pu boire plus tôt que ceux du groupe PER (90±34 vs 111±38 min,P<0,05). Les autres étapes de la récupération étaient semblables et le congé a été accordé après un temps de récupération similaire pour tous.
Conclusion: L’administration peropératoire, comparée à l’administration postopératoire, de 0,1 mg·kg−1 de morphineiv améliore l’analgésie postopératoire au réveil d’une intervention chirurgicale ambulatoire algique sans augmenter l’incidence de NVPO.
Article PDF
Similar content being viewed by others


References
Ritchie ED, Chung F, Su J, Claxton A, Thanamayooran S. Indicators of excessive pain in ambulatory surgery. Anesthesiology 1995; 83: A46.
Chung F, Ritchie E, Su J. Postoperative pain in ambulatory surgery. Anesth Analg 1997; 85: 808–16.
Denton JE, Beecher HK. A comparison of the side effects of morphine, methadone and methadone’s isomers in man. JAMA 1949; 141: 1148–53.
Whitehead EM, O’Sullivan GM, Lloyd J, Bullingham RES. A new method for rate of analgesia onset: two doses of intravenous morphine compared with placebo. Clin Pharmacol Ther 1992; 69: 2S-19.
Clarke RSJ, Dundee JW, Love WJ. Studies of drugs given before anaesthesia. VIII: Morphine 10 mg alone and with atropine or hyoscine. Br J Anaesth 1965; 37: 772–7.
Watcha MF, Jones MB, Lagueruela RG, Schweiger C, White PF. Comparison of ketoralac and morphine as adjuvants during pediatric surgery. Anesthesiology 1992; 76: 368–72.
Aldrete JA, Kroulik D. A postanesthetic recovery score. Anesth Analg 1970; 49: 924–34.
Chung F. Are discharge criteria changing? J Clin Anesth 1993; 5(Suppl1): 64S-8.
Stoelting R Opioid agonists and antagonists.In: Stoelting R (Ed.). Pharmacology and Physiology in Anesthetic Practice. Philadelphia: Lippincott, 1987: 69–101.
Claxton A, McGuire G, Chung F, Cruise C. Evaluation of morphine versus fentanyl for postoperative analgesia after ambulatory surgical procedures. Anesth Analg 1997; 84: 509–14.
Kamath B, Curran J, Hawkey C, et al. Anaesthesia, movement and emesis. Br J Anaesth 1990; 64: 728–30.
Lasagna L, Beecher HK. The optimal dose of morphine. JAMA 1954; 156: 230–4.
Mansfield MD, James KS, Kinsella J. Influence of dose and timing of administration of morphine on postoperative pain and analgesic requirements. Br J Anaesth 1996; 76: 358–61.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wong, J., Ritchie, E., Chung, F. et al. Intraoperativevs post-operative morphine improves analgesia without increasing PONV on emergence from ambulatory surgery. Can J Anaesth 47, 1090–1093 (2000). https://doi.org/10.1007/BF03027960
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03027960