
Abstract
Purpose
We compared the efficacy of patient-controlled analgesia (PCA), with or without a background infusion of morphine, on postoperative pain relief in patients extubated in the operating room after coronary artery bypass grafting (CABG) surgery.
Methods
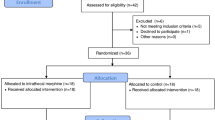
With Faculty Ethics approval, 60 consenting adults undergoing elective coronary artery surgery were randomly assigned to receive either morphine PCA alone (group PCA-A,n = 30) or morphine PCA plus a background infusion (group PCA-B,n = 30) for 24 hr postoperatively Pain scores with verbal rating scale (VRS1 from 0 to 10) at rest, sedation scores, morphine consumption and delivery/demand ratios were assessed at zero, one, two, four, six, 12 and 24 hr after surgery. Hemodynamic variables and arterial blood gases were also recorded in the same periods.
Results
Sedation scores in the two groups were similar. At all study periods after the first postoperative hour, VRS remained below 5 in both groups. Pain scores were significantly lower in the background infusion group, which also had greater cumulative morphine consumption (61.7 ± 10.9 mg vs 38.5 ± 16.2 mg). There were no episodes of hypoxemia or hypertension.
Conclusion
Morphine PCA effectively controlled postoperative pain after cardiac surgery. The addition of a background infusion of morphine enhanced analgesia and increased morphine consumption.
Résumé
Objectif
Nous avons comparé les effets de l’analgésie autocontrôlée (AAC), avec ou sans une perfusion de morphine de base, sur l’analgésie postopératoire des patients extubés au bloc opératoire à la suite d’un pontage aortocoronalre.
Méthode
Soixante adultes consentants devant subir une opération de pontage aortocoronalre réglée ont été recrutés dans notre étude après l’accord du Comité d’Éthique de la Faculté. Les patients ont reçu soit de la morphine en AAC seule (Groupe AAC-A, n = 30), soit de la morphine en AAC plus une perfusion de base continue (Groupe AAC-B, n =30) pendant 24 h après l’opération. La douleur au repos selon une échelle verbale analogique (score de 0 à 10), les scores de sédation, la consommation de morphine, ainsi que les niveaux sérlques de morphine à zéro, une, deux, quatre, six, 12 et 24 h après l’opération ont été évalués. Le bilan hémodynamique et les gaz du sang ont aussi été enregistrés durant la même période.
Résultats
Il n’y avait pas de différence dans les scores de sédation entre les deux groupes. Après la première heure postopératoire l’échelle verbale analogique était en dessous de 5 dans les deux groupes. Les scores de douleurs étalent slgnlfcatlvement moins élevés dans le groupe perfusion de base; ce dernier groupe avait aussi une plus grande consommation cumulative de morphine (61,7 ± 10,9 mgvs38,5 ± 16,2 mg). Il n’y a pas eu d’épisode d’hypoxle ni d’hypertension.
Conclusion
LAAC avec la morphine réduit efficacement la douleur postopératoire en cardiochirurgie. L’ajout d’une perfusion de base de morphine améliore l’analgésie et augmente la consommation de morphine.
Article PDF
Similar content being viewed by others


References
Lee TW, Jacobsohn E. Pro: Tracheal extubation should occur routinely in the operating room after cardiac surgery. J Cardiothorac Vasc Anesth 2000; 14: 603–10.
Gust R, Pecher S, Gust A, Hoffmann V, Bohrer H, Martin E. Effect of patient-controlled analgesia on pulmonary complications after coronary artery bypass grafting. Crit Care Med 1999; 27: 2218–23.
O’Connor CJ. Pain relief and pulmonary morbidity after cardiac surgery. Crit Care Med 1999; 27: 2314–6.
Checketts MR, Gilhooly CJ, Kenny GN. Patient-maintained analgesia with target-controlled alfentanil infusion after cardiac surgery: a comparison with morphine PCA. Br J Anaesth 1998; 80: 748–51.
Macintyre PE. Safety and efficacy of patient-controlled analgesia. Br J Anaesth 2001; 87: 36–46.
Walder B, Schäfer M, Henzi I, Tramer MR. Efficacy and safety of patient-controlled opioid analgesia for acute postoperative pain. A quantitative systematic review. Acta Anaesthesiol Scand 2001; 45: 795–804.
Lam KK, Chan MT, Chen PP, Kee WD. Structured preoperative patient education for patient-controlled analgesia. J Clin Anesth 2001; 13: 465–9.
Myles PS, Buckland MR, Cannon GB, et al. Comparison of patient-controlled analgesia and nursecontrolled infusion analgesia after cardiac surgery. Anaesth Intensive Care 1994; 22: 672–8.
Pettersson PH, Lindskog EA, Öwall A. Patient-controlled versus nurse-controlled pain treatment after coronary artery bypass surgery. Acta Anaesthesiol Scand 2000; 44: 43–7.
Boldt J, Thaler E, Lehmann A, Papsdorf M, Lsgro F. Pain management in cardiac surgery patients: comparison between standard therapy and patient-controlled analgesia regimen. J Cardiothorac Vasc Anesth 1998; 12: 654–8.
Tsang J, Brush B. Patient-controlled analgesia in postoperative cardiac surgery. Anaesth Intensive Care 1999; 27: 464–70.
Rapanos T, Murphy P, Szalai JP, Burlacoff L, Lam-McCulloch J, Kay J. Rectal indomethacin reduces postoperative pain and morphine use after cardiac surgery. Can J Anesth 1999; 46: 725–30.
Searle NR, Roy M, Bergeron G, et al. Hydromorphone patient-controlled analgesia (PCA) after coronary artery bypass surgery. Can J Anaesth 1994; 41: 198–205.
Ramsay MA, Savege TM, Simpson BR, Goodwin R. Controlled sedation with alphaxolone-alphadolone. Br J Med 1974; 2: 656–9.
Dal D, Kanbak M, Caglar M, Aypar U. A background infusion of morphine does not enhance postoperative analgesia after cardiac surgery. Can J Anesth 2003; 50: 476–9.
Dawson PJ, Libreri EC, Jones DJ, Libreri G, Bjorkstein AR, Royse CF. The efficacy of adding a continuous intravenous morphine infusion to patient-controlled analgesia (PCA) in abdominal surgery. Anaesth Intensive Care 1995; 23: 453–8.
Doyle E, Harper L, Morton NS. Patient-controlled analgesia with low dose background infusions after lower abdominal surgery in children. Br J Anaesth 1993; 71: 818–22.
Munro AJ, Long GT, Sleigh JW. Nurse-administered subcutaneous morphine is a satisfactory alternative to intravenous patient-controlled analgesia morphine after cardiac surgery. Anesth Analg 1998; 87: 11–5.
Zimmermann AR, Kibblewhite D, Sleigh J. Comparison of morphine/droperidol and tramadol/droperidol mixture for patient controlled analgesia (PCA) after cardiac surgery: a prospective, randomised, double-blind study. Acute Pain 2002; 4: 65–9.
Schug SA, Torrie JJ. Safety assessment of postoperative pain management by an acute pain service. Pain 1993; 55: 387–91.
Smythe MA, Zak MB, O’Donnell MP, Schad RF, Dmuchowski CF. Patient-controlled analgesia versus patient-controlled analgesia plus continuous infusion after hip replacement surgery. Ann Pharmacother 1996; 30: 224–7.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Guler, T., Unlugenc, H., Gundogan, Z. et al. A background infusion of morphine enhances patient-controlled analgesia after cardiac surgery. Can J Anesth 51, 718–722 (2004). https://doi.org/10.1007/BF03018432
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03018432