
Abstract
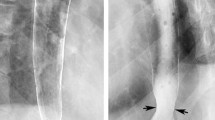
The roentgenographic, echocardiographic, endoscopic, and manometric findings were studied in five consecutive patients with cardiovascular dysphagia, including four with a dilated left atrium and one with an anomalous left subclavian artery. Common and different manometric findings were found in the two types of cardiovascular dysphagia. The major manometric abnormality in all cases was an elevated baseline pressure, with superimposed large rhythmic pressure waves occurring at the same frequency as the electrocardiogram in the mid-esophagus. This manometric abnormality, produced by pulsatile cardiovascular compression, provides direct evidence that cardiovascular dysphagia is caused by esophageal luminal obstruction from cardiovascular compression. Indirect evidence supporting this mechanism includes smooth extrinsic compression and hang-up of ingested barium in the mid-esophagus on esophagogram and transmitted mural pulsations and a compressed lumen in the mid-esophagus at panendoscopy. Two of the five patients had deranged esophageal peristalsis within the high-pressure zone, which also contributed to the dysphagia. Autopsy in one patient with deranged peristalsis revealed a band of ischemic esophageal mucosa in the zone compressed by the dilated left atrium. A novel manometric maneuver might distinguish dysphagia due to an anomalous left subclavian artery from dysphagia due to a dilated left atrium. Left arm elevation during manometry in the single patient with the anomalous artery significantly increased the mean mid-esophageal baseline pressure by 92% (N=10 trials), and mean pressure wave amplitude by 93% (N=10 trials,P<0.002 for each, nonparametric signed rank test). Left arm elevation in this patient also increased the observed luminal obstruction during endoscopy. These manometric and endoscopic findings may be explained by increased arterial compression of the esophagus produced by arterial stretch and anterior displacement with arm elevation.
Similar content being viewed by others


References
Behl PR, Holden MP: Mitral valve disease and dysphagia. Eur Heart J 5:919–923, 1984
Channer KS, Bell J, Virjee JP: Effect of left atrial size on the oesophageal transit of capsules. Br Heart J 52:223–227, 1984
Jorgensen F, Hesse B, Gronbaek P, Fogh J, Hanuso S: Abnormal oesophageal function in patients with non-toxic goiter or enlarged left atrium, demonstrated by radionuclide transit measurements. Scand J Gastroenterol 24:1186–1192, 1989
Cappell MS: Manometric findings in dysphagia secondary to left atrial dilatation: Giant, cyclic midesophageal pressure waves occurring with every heart beat. Dig Dis Sci 36:693–698, 1991
Bohane TD, Perrault J, Fowler RS: Oesophagitis and oesophageal obstruction from quinidine tablets in association with left atrial enlargement: A case report. Aust Paediatr J 14:191–192, 1978
Lincoln JCR, Deverall PB, Stark J, Aberdeen E, Waterston DJ: Vascular anomalies compressing the esophagus and trachea. Thorax 24:295–306, 1969
Lubbe WF, Cadogan ES, Kannemey AHR: Oesophageal ulceration due to slow release potassium in the presence of left atrial enlargement. NZ Med J 90:377–379, 1979
McCall AJ: Slow-K ulceration of esophagus with aneurysmal left atrium. Br Med J 3:230–231, 1975 (letter)
Sumithran E, Lim KH, Chiam HL: Atrio-esophageal fistula complicating mitral valve disease. Br Med J 2:1552–1553, 1979
Conte BA: Dysphagia caused by an aneurysm of the descending thoracic aorta: Relief by surgical creation of a hiatal hernia. N Engl J Med 274:956–957, 1966
Birnholz JC, Ferrucci JT, Wyman SM: Roentgen features of dysphagia aortica. Radiology 111:93–96, 1974
McMillan IKR, Hyde I: Compression of the oesophagus by aorta. Thorax 24:32–38, 1969
Mittal RK, Siskind BN, Hongo M, Flye W, McCallum RW: Dysphagia aortica: Clinical, radiological and manometric findings. Dig Dis Sci 31:379–384, 1986
Berenzweig H, Baue AE, McCallum RW: Dysphagia lusoria: Report of a case and review of the diagnostic and surgical approach. Dig Dis Sci 25:630–636, 1980
McNally PR, Rak KM: Dysphagia lusoria caused by persistent right aortic arch with aberrant left subclavian artery and diverticulum of Kommerell. Dig Dis Sci 37:144–149, 1992
Gabert E: Die lagebeziehung des osophagus zur dorsalen. Fortschr Geb Rontgenstr 32:410–415, 1924
Steel D: Extreme dilatation of the left auricle. Am J Roentgenol 26:66–73, 1931
Ashworth H, Jones AM: Aneurysmal dilatation of left auricle with erosion of spine. Br Heart J 8:207–211, 1946
Daley R, Franks R: Massive dilatation of the left auricle. Q J Med 18:81–91, 1949
Bishop LJ Jr, Babey A: Massive left auricle. JAMA 106:462–464, 1936
Nichols CF, Ostrum HW: Unusual dilation of the left auricle. Am Heart J 8:205–216, 1932
Patterson R: The value of roentgenologic study of the esophagus and bronchi in cases of heart disease, especially mitral disease. Am J Roentgenol 23:396–408, 1930
Dines DE, Anderson MV: Giant left atrium as a cause of dysphagia. Ann Intern Med 65:758–760, 1966
Morgan AA, Mourant AJ: Left vocal cord paralysis and dysphagia in mitral valve disease. Br Heart J 43:470–473, 1980
Dolowitz DA, Lewis CS: Left vocal cord paralysis associated with heart disease. Am J Med 4:856–862, 1948
Fetterolf G, Norris GW: The anatomical explanation of the paralysis of the left recurrent laryngeal nerve found in certain cases of mitral stenosis. Am J Med Sci 141:625–638, 1911
Hurst JW, Crawley IS, Morris DC, Dorney ER: The history: Symptoms and past events related to cardiovascular disease.In The Heart: Arteries and Veins, 7th ed. WJ Hurst, RG Schlant, CE Rackley, EH Sonnenblick, NK Wenger (eds). New York, McGraw-Hill, 1990, p 133
Schulze K, Dodds WJ, Christensen J, Wood JD: Esophageal manometry in the opossum. Am J Physiol 233:E152-E159, 1977
Stagias JG, Ciarolla D, Campo S, Seeman H, Burrell MI, Traube M. Vascular compression of the esophagus: A manometric and radiographic study (abstract). Gastroenterology 104(4 part 2):A197, 1993
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Cappell, M.S. Endoscopic, radiographic, and manometric findings associated with cardiovascular dysphagia. Digest Dis Sci 40, 166–176 (1995). https://doi.org/10.1007/BF02063961
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02063961