
Abstract
According to population-based epidemiological studies using International Headache Society diagnostic criteria, the prevalence of migraine in developed countries ranges from 8 to 14%. These prevalence figures confirm the widespread nature of the disorder. Moreover, as migraine is a chronic episodic disorder that predominantly affects people during their working lives (between the ages of 25 and 55 years), indirect costs associated with reduced productivity represent a substantial proportion of the total cost of migraine.
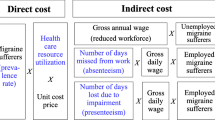
The results of health-related quality-of-Life studies demonstrate that migraine has a considerable impact on functional capacity, resulting in disrupted work and social activities. Many migraineurs, however, do not seek medical attention, have not been accurately diagnosed by a physician or do not use prescription medication. Therefore, the direct costs of treatment for migraine are relatively small compared with the indirect costs.
Migraine is an important chronic illness that has a major impact on the working sector of a population. The overall cost attributable to migraine is unknown, but it is now established that the indirect costs of migraine outweigh the direct costs and therefore represent an obvious target for healthcare intervention aimed at reducing the impact of this chronic condition.
Similar content being viewed by others


References
Stewart WF, Lipton RB, Celentano DO, et al. Prevalence ofmigraine headache in the United States. JAMA 1992; 267:64–9
Pryse-Phillips W, Findlay H, Tugwell P, et al. A Canadian population survey on the clinical, epidemiologic and societal impactof migraine and tension-type headache. Can J Neurol Sci1992; 19: 333–9
International Headache Society (IHS). Headache Classification Committee of the IHS. Classification and diagnostic criteriafor headache disorders, cranial neuralgias, and facial pain.Cephalalgia 1988; 8 Suppl. 7: 1–96
Breslau N, Merikangas K, Bowden CL. Comorbidity of migraine and major affective disorders. Neurology 1994; 44Suppl. 7: 17–22
Blau IN.Migraine: theories of pathogenesis. Lancet 1992; 339: 1202–7
Merikangas KR. Genetic epidemiology of migraine. In: Sandler M, Collins GM, editors. Migraine: a spectrum of ideas. Oxford University Press, 1990: 40–50
Bartelink ML, van Weel C. Migraine in female patients in family practice. Headache Quarterly 1995; 6: 203–7
Lipton RB, Silberstein SO, Stewart WF. An update on the epidemiology of migraine. Headache 1994; 34: 319–28
Stewart WF, Simon O, Shecter A, et al. Population variation in migraine prevalence: a meta-analysis. J Clin Epidemiol 1995;48: 269–80
Lipton RB, Stewart WF. The epidemiology of migraine. Eur Neurol 1994; 34 Suppl. 2: 6–11
Edmeads J, Findlay H, Tugwell P, et al. Impact of migraine and tension-type headache on life-style, consulting behaviour and medication use: a Canadian population survey. Can J Neurol Sci 1993; 20: 131–7
Stang PE, Osterhaus JT, Celetano DO. Migraine: patterns of healthcare use. Neurology 1994; 44 Suppl. 4: S47–55
Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and healthcare use. Neurology 1993; 43Suppl. 3: 6–10
Breslau N, Davis GC, Andreski P. Migraine, psychiatric disorders, and suicide attempts: an epidemiologic study of youngadults. Psychiatry Res 1991; 37: 11–23
Cull RA, Wells NEJ, Miocevich ML. The economic cost of migraine. Br J Med Econ 1992; 2: 103–15
Henry P, Michel P, Brochet B, et al. A nationwide survey of migraine in France: prevalence and clinical features in adults.Cephalalgia 1992; 12: 229–37
Michel P, Pariente P, Duru G, et al. MIG ACCESS: a population- based, nationwide, comparative survey of access to carein migraine in France. Cephalalgia 1995; 16: 50–5
Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population: a prevalence study. J ClinEpidemiol 1991; 44: 1147–57
van Roijen L, Essink-Bot ML, Koopmanschap MA, et al. Societal perspective on the burden of migraine in The Netherlands.Pharmaco Economics 1995; 7: 170–9
Action Asthma. The occurrence and cost of asthma. Worthing: Cambridge Medical Publications, 1990 (ISBN: 0904052028)
British Diabetic Association (BOA). Diabetes in the United Kingdom. London: BOA, 1988
Office of Health Economics (OHE). Epilepsy. London: OHE,1991
Cull RE, Wells NEJ, Miocevich ML. The economic cost of migraine. Br J Med Econ 1992; 2: 103–15
Stewart WF, Linet MA, Celentano DO, et al. Age and sex-specific incidence rates of migraine with and without visual aura.Am J Epidemiol 1991; 34: 1111–20
MacGregor EA. Menstrual migraine: towards a definition. Cephalalgia 1996; 16: 11–21
Silberstein SO. The role of sex hormones in headache. Neurology 1992; 42 Suppl. 2: 37–42
Abu-Arefeh I, Russell G. Prevalence of headache and migraine in schoolchildren. BMJ 1994; 309: 765–9
Raieli V, Raimondo O, Cammalleri R, et al. Migraine headaches in adolescents: a student population-based study in Monreale.Cephalalgia 1995; 15: 5–12
Lipton RB, Stewart WF, Von Korff M. Migraine impact and functional disability. Cephalalgia 1995; Suppl. 15: 4–9
Von Korff M, Ormel J, Keefe F, et al. Grading the severity of chronic pain. Pain 1992; 50: 133–49
Patrick DL, Erickson P. Health status and health policy: quality of life in healthcare evaluation and resource allocation. NewYork: Oxford University Press, 1992
Hartmaier SL, Santanello N, Epstein RS, et al. Development of a brief 24-hour migraine-specific quality of life questionnaire.Headache 1995; 35: 320–9
Miller DW, Kirchdoerfer LJ, Sheperd MO, et al. Adisease-spe-cific instrument to measure quality of life effects attributableto migraine. Health Service Research Association 10th Annual Meeting: 1993 June 27-29, Washington DC
Richard A, Henry P, Chazot G, et al. Qualite de vie et migraine. Validation du questionnaire QVM en consultationhospitaliere et en medecine generale. Therapie 1993; 48:89–96
Santanello NC, Hartmaier SL, Epstein SL, et al. Validation of a new quality of life questionnaire for acute migraine headache.Headache 1995; 35: 330–7
Osterhaus JT, Townsend RJ, Gandek B, et al. Measuring the functional stalUs and well-being of patients with migraineheadache. Headache 1994; 34: 337–43
Essink-Bot ML, van Royen L, Krabbe P, et al. The impact of migraine on health status. Headache 1995; 35: 200–6
Tarlov AR, Ware JE, Greenfield S, et al. The medical outcomes study. An application of methods for monitoring the results of medical care. JAMA 1989; 262: 925–30
Stewart AL, Greenfield S, Hays RD, et al. Functional status and well-being of patients with chronic medical conditions. Results from the medical outcomes study. JAMA 1989; 262:907–13
Solomon GD, Skobieranda FG, Gragg LA. Does quality of life differ among beadacbe diagnoses? Analysis using tbe MedicalOutcomes Study Instrument. Headache 1994; 34: 143–7
Dahlöf CGH, Dimeneäs E. Migraine patients experience poorer subjective well-being/quality of life even between attacks.Cephalalgia 1995; 15: 31–6
Drummond M. Cost-of-illness studies. A major headache? Pharmaco Economics 1992; 2; 1–4
Davey PJ, Leeder SR. The cost of migraine. More than just a headache? Pharmaco Economics 1992; 2: 5–7
de Lissovoy G, Lazarus SS. The economic cost of migraine. Present state of knowledge. Neurology 1994; 44 Suppl. 4:56–62
Blau IN, Drummond MF. Migraine. Office of Health Economics OHE London: OHE, 1991
Ramussen BK. Epidemiology of headache. Cephalalgia 1995: 15: 45–68
Lipton RB, Stewan WF, Von Korff M. Individual and societal impact of migraine. In: Olesen J, editor. Headache classification and epidemiology. New York: Raven Press, 1994: 327–33
Osterhaus JT. Gutterman DL. Plachetka JR. Healthcare resource and lost labour costs of migraine headache in the US.Pharmaco Economics 1992; 2: 67–76
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Solomon, G.D., Price, K.L. Burden of Migraine. Pharmaco economics 11 (Suppl 1), 1–10 (1997). https://doi.org/10.2165/00019053-199700111-00003
Published:
Issue Date:
DOI: https://doi.org/10.2165/00019053-199700111-00003