
Abstract
Background
We designed a phase II trial to examine the benefit of preoperative hyperfractionated radiation therapy (XRT) and concurrent chemotherapy for patients with locally advanced esophageal cancer (LAEC).
Aim of Study
The pathologic complete response (pCR) was the primary endpoint to estimate efficacy.
Methods
Twenty-three patients with LAEC received twice-daily XRT during wk 1 and 5 once-daily XRT during wk 2–4 (59 Gy). Cisplatin (100 mg/m2) was given on d 1, while 5-fluorouracil (1000 mg/m2) was given by continuus infusion the first and fifth weeks of the XRT.
Results
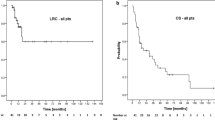
The pCR for the 19 patients undergoing esophagectomy was 16%. The study was closed at the interim analysis having not met the required minimum pCR rate of 20%. Hematologic toxicities consisted of grades III and IV neutropenia observed in 33% and 14% of patients, respectively. Grade III nausea and vomiting was seen in 38% of patients. One grade V pulmonary toxicity occurred. The median survival was 44.6 mo with 65% of patients alive at 2 yr.
Conclusions
The pCR rate in this trial did not meet the predetermined statistical minimum. With the encouraging 2-yr survival, it is not clear that pCR is a reliable surrogate endpoint to discern treatment efficacy.
Similar content being viewed by others


References
Jemal A, Murray T, Ward E, et al. Cancer statistics, 2005. CA Cancer J Clin, 2005;55:10–30.
Herskovic A, Martz K, al-Sarraf M, et al. Combined chemotherapy and radiotherapy compared with radiotherapy alone in patients with cancer of the esophagus. N Engl J Med 1992;326:1593–1598.
al-Sarraf M, Martz K, Herskovic A, et al. Progress report of combined chemoradiotherapy versus radiotherapy alone in patients with esophageal cancer: an intergroup study. J Clin Oncol, 1997;15:277–284.
Choi N, Park SD, Lynch T, et al. Twice-daily radiotherapy as concurrent boost technique during two chemotherapy cycles of adjuvant chemoradiotherapy for resectable esophageal carcinoma: mature results of a phase II study. Int J Radiat Oncol Biol Phys, 2004;60:111–122
Leichman L, Steiger Z, Seydel HG, et al. Preoperative chemotherapy and radiation therapy for patients with cancer of the esophagus: a potentially curative approach. J Clin Oncol, 1984;2:75–79.
Thames HD, Peters LJ, Withers HR, Fletcher GH. Accelerated fractionation vs hyperfractionation: rationale for several treatments per day. Int J Radiat Oncol Biol Phys 1983;9:127–138.
Jeremic B, Shibamoto Y, Acimovic L, et al. Accelerated hyperfractionated radiation therapy and concurrent 5-fluorouracil/cisplatin chemotherapy for locoregional squamous cell carcinoma of the thoracic esophagus: a phase II study. Int J Radial Oncol Biol Phys, 1998;40:1061–1066.
Swisher SG, Ajani JA, Komaki R, et al. Long-term outcome of phase II trial evaluating chemotherapy, chemoradiotherapy, and surgery for locoregionally advanced esophageal cancer. Int J Radiat Oncol Biol Phys, 2003;57: 120–127.
NCI/CTC. Website: http://ctep.info.nih.gov.
Kaplan E, Meier P. Nonparametric estimation from in complete observations. J Am Stat Assoc, 1958;53:457–481.
Urba SG, Orringer MB, Ianettonni M, Hayman JA, Satoru H. Concurrent cisplatin, paclitaxel, and radiothrrapy as preoperative treatment for patients with locoregional esophageal carcinoma. Cancer, 2003;98:2177–2183.
Urba SG, Orringer MB, Turrisi A, Lannettoni M, Forastiere A, Strawderman M. Randomized trial of preoperative chemoradiation versus surgery alone in patients with locoregional esophageal carcinoma. J Clin Oncol, 2001;19:305–313.
Bosset JF, Gignoux M, Triboulet JP, et al. Chemoradiotherapy followed by surgery compared with surgery alone in squamous cell cancer of the esophagus. N Engl J Med 1997;337:161–167.
Blackstock AW, Farmer MR, Lovato J, et al. A prospective evaluation of the impact of 18-F-fluoro-deoxy-D-glucose positron emission tomography staging on survival for patients with locally advanced esophageal cancer. Int J Radiat Oncol Biol Phys, 2006;64:455–460.
Donington JS, Miller DL, Allen MS, Deschamps C, Nichols FC, 3rd, Pairolero PC. Tumor response to induction chemoradiation: influence on survival after esophagectomy. Eur J Cardiothorac Surg, 2003;24:631–636; discussion 636–637.
Poplin E, Fleming T, Leichman L, et al. Combined therapies for squamous-cell carcinoma of the esophagus, a Southwest Oncology Group Study (SWOG-8037). J Clin Oncol 1987;5:622–628.
Berger AC, Farma J, Scott WJ, et al. Complete response to neoadjuvant chemoradiotherapy in esophageal carcinoma is associated with significantly improved survival. J Clin Oncol, 2005;23:4330–4337.
Jones DR, Detterbeck FC, Egan TM, Parker LA, Jr., Bernard SA, Tepper JE, Induction chemoradiotherapy followed by esophagectomy in patients with carcinoma of the esophagus. Ann Thorac Surg, 1997;64:185–191; discussion 191–182.
Kleinberg L, Knisely JP, Heitmiller RF, et al. Mature survival results of preoperative cisplatin, protracted infusion 5-fluorouracil, and 44-Gy radiotherapy for esophageal cancer. Int J Radiat Oncol Biol Phys 2003;56:328–334.
Rohtagi PR, Swisher SG, Correa AM, et al. Failure patterns correlate with the proportion of residual carcinoma after preoperative chemoradiotherapy for carcinoma of the esophagus. Cancer, 2005;104:1349–1355.
Lee J-L, Park SI, Kim S-B, et al. A single institutional phase III trial of preoperative chemotherapy and hyperfractionated radiotherapy plus surgery versus surgery alone for resectable esophageal squamous carcinoma. Ann Oncol 2004;15:947–954.
Zhao KL, Shi XH, Jiang GL, et al. Late course accelerated hyperfractionated radiotherapy plus concurrent chemotherapy for squamous cell carcinoma of the esophagus: a phase III randomized study. Int J Radiat Oncol Biol Phys 2005;62:1014–1020.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Blackstock, A.W., Aklilu, M., Lovato, J. et al. Pathologic complete response may not represent the optimal surrogate for survival after preoperative therapy for esophageal cancer. Int J Gastrointest Canc 37, 7–14 (2006). https://doi.org/10.1385/IJGC:37:1:7
Issue Date:
DOI: https://doi.org/10.1385/IJGC:37:1:7