
Abstract
Background
The effect of routine drainage after abdominal surgery with enteric anastomoses is controversial. In particular, the role of peritoneal drain (PD) placement after total gastrectomy for adenocarcinoma is not well established.
Methods
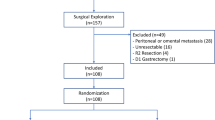
Patients who underwent total gastrectomy for gastric adenocarcinoma (GAC) at seven institutions from the US Gastric Cancer Collaborative, from 2000 to 2012, were identified. The association of PD placement with postoperative outcomes was analyzed.
Results
Overall, 344 patients were identified and 253 (74 %) patients received a PD. The anastomotic leak rate was 9 %. Those with PD placement had similar American Society of Anesthesiologists score, tumor size, TNM stage, and the need for additional organ resection when compared with their counterparts. No difference was observed in the rate of any complication (54 vs. 48 %; p = 0.45), major complication (25 vs. 24 %; p = 0.90), or 30-day mortality (7 vs. 4 %; p = 0.51) between the two groups. In addition, no difference in anastomotic leak (9 vs. 10 %; p = 0.90), the need for secondary drainage (10 vs. 9 %; p = 0.92), or reoperation (13 vs. 8 %; p = 0.28) was identified. On multivariate analysis, PD placement was not associated with decreased postoperative complications. Subset analysis, stratified by patients who did not undergo concomitant pancreatectomy (n = 319) or those who experienced anastomotic leak (n = 31), similarly demonstrated no association of PD placement with reduced complications or mortality.
Conclusions
PD placement after total gastrectomy for GAC is associated with neither a decrease in the frequency and severity of adverse postoperative outcomes, including anastomotic leak and mortality, nor a decrease in the need for secondary drainage procedures or reoperation. Routine use of PDs is not warranted.
Similar content being viewed by others

References
Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29.
Brown LM, Devesa SS. Epidemiologic trends in esophageal and gastric cancer in the United States. Surg Oncol Clin N Am. 2002;11:235–56.
Hansson LE, Sparen P, Nyren O. Increasing incidence of carcinoma of the gastric cardia in Sweden from 1970 to 1985. Br J Surg. 1993;80:374–7.
Steevens J, Botterweck AA, Dirx MJ, et al. Trends in incidence of oesophageal and stomach cancer subtypes in Europe. Eur J Gastroenterol Hepatol. 2010;22:669–78.
Vial M, Grande L, Pera M. Epidemiology of adenocarcinoma of the esophagus, gastric cardia, and upper gastric third. Recent Results Cancer Res. 2010;182:1–17.
Dassen AE, Lemmens VE, van de Poll-Franse LV, et al. Trends in incidence, treatment and survival of gastric adenocarcinoma between 1990 and 2007: a population-based study in the Netherlands. Eur J Cancer. 2010;46:1101–10.
Piazuelo MB, Correa P. Gastric cancer: overview. Colomb Med (Cali). 2013;44:192–201.
Smyth EC, Capanu M, Janjigian YY, et al. Tobacco use is associated with increased recurrence and death from gastric cancer. Ann Surg Oncol. 2012;19:2088–94.
Song Q, Wang J, Jia Y, et al. Shorter dinner-to-bed time is associated with gastric cardia adenocarcinoma risk partly in a reflux-dependent manner. Ann Surg Oncol. 2014;21:2615–9.
Ajani JA, Bentrem DJ, Besh S, et al. National Comprehensive Cancer Network. Gastric cancer, version 2.2013: featured updates to the NCCN Guidelines. J Natl Compr Canc Netw. 2013;11(5):531–46.
Wang Z, Chen J, Su K, Dong Z. Abdominal drainage versus no drainage post gastrectomy for gastric cancer. Cochrane Database Syst Rev. 2011;(8):CD008788. doi:10.1002/14651858.CD008788.pub2.
Petrowsky H, Demartines N, Rousson V, Clavien PA. Evidence-based value of prophylactic drainage in gastrointestinal surgery: a systematic review and meta-analyses. Ann Surg. 2004;240(6):1074–84; discussion 1084–5.
Conlon KC, Labow D, Leung D, et al. Prospective randomized clinical trial of the value of intraperitoneal drainage after pancreatic resection. Ann Surg. 2001;234(4):487–93; discussion 493–4.
Correa-Gallego C, Brennan MF, Dʼangelica M, et al. Operative drainage following pancreatic resection: analysis of 1122 patients resected over 5 years at a single institution. Ann Surg. 2013;258(6):1051–8.
Mehta VV, Fisher SB, Maithel SK, Sarmiento JM, Staley CA, Kooby DA. Is it time to abandon routine operative drain use? A single institution assessment of 709 consecutive pancreaticoduodenectomies. J Am Coll Surg. 2013;216(4):635–42; discussion 642–4.
Van Buren G 2nd, Bloomston M, Hughes SJ, et al. A randomized prospective multicenter trial of pancreaticoduodenectomy with and without routine intraperitoneal drainage. Ann Surg. 2014;259(4):605–12.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–13.
Dougherty HH, Simmons RL. The biology and practice of surgical drains. Part 1 Curr Probl Surg. 1992;29:559–730.
Kim J, Lee J, Hyung WJ, Cheong JH, Chen J, Choi SH, et al. Gastric cancer surgery without drains: a prospective randomized trial. J Gastrointest Surg. 2004;8 (6):727–32.
Kumar M, Yang SB, Jaiswal VK, Shah JN, Shreshtha M, Gongal R. Is prophylactic placement of drains necessary after subtotal gastrectomy? World J Gastroenterol. 2007;13(27):3738–41.
Jiang ZW, Li JS, Wang ZM, Li N, Diao YQ, Huang XJ. Prospective randomized study of abdominal drains in gastric cancer surgery. Chin J Pract Surg. 2008;28(9):761–2.
Álvarez Uslar R, Molina H, Torres O, Cancino A. Total gastrectomy with or without abdominal drains: a prospective randomized trial. Revista Espanola de Enfermedades Digestivas 2005;97(8):562–9.
Acknowledgment
This study is supported in part by the Katz Foundation.
Disclosure
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dann, G.C., Squires, M.H., Postlewait, L.M. et al. Value of Peritoneal Drain Placement After Total Gastrectomy for Gastric Adenocarcinoma: A Multi-institutional Analysis from the US Gastric Cancer Collaborative. Ann Surg Oncol 22 (Suppl 3), 888–897 (2015). https://doi.org/10.1245/s10434-015-4636-7
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-4636-7