
Abstract
Background
Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) used to treat peritoneal surface disease (PSD) from appendiceal cancer have shown variability in survival outcomes. The primary goal of this study was to determine predictors of surgical morbidity and overall survival. The secondary goal was to describe the impact of nodal status on survival after CRS/HIPEC for PSD from low-grade appendiceal (LGA) and high-grade appendiceal (HGA) primary lesions.
Methods
A retrospective analysis of 1,069 procedures from a prospective database was performed. Patient characteristics, tumor grade, nodal status, performance status, resection status, morbidity, mortality, and survival were reviewed.
Results
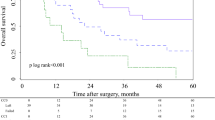
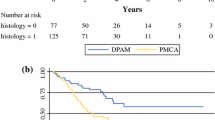
The study identified 481 CRS/HIPEC procedures: 317 (77.3 %) for LGA and 93 (22.7 %) for HGA lesions. The median follow-up period was 44.4 months, and the 30-day major morbidity and mortality rates were respectively 27.8 and 2.7 %. Major morbidity was jointly predicted by incomplete cytoreduction (p = 0.0037), involved nodes (p < 0.0001), and comorbidities (p = 0.003). Multivariate negative predictors of survival included positive nodal status (p = 0.003), incomplete cytoreduction (p < 0.0001), and preoperative chemotherapy (p = 0.04) in LGA patients and incomplete cytoreduction (p = 0.0003) and preoperative chemotherapy (p = 0.0064) in HGA patients. After complete cytoreduction, median survival was worse for patients with positive nodes than for those with negative nodes in LGA (85 months vs not reached [82 % alive at 90 months]; p = 0.002) and HGA (30 vs 153 months; p < 0.0001).
Conclusions
Positive nodes are associated with decreased survival not only for HGA patients but also for LGA patients even after complete cytoreduction. Nodal status further stratifies histologic grade as a prognostic indicator of survival. Patients with node-negative HGA primary lesions who receive a complete cytoreduction may experience survival comparable with that for LGA patients.


Similar content being viewed by others

References
Chua TC, Moran BJ, Sugarbaker PH, et al. Early- and long-term outcome data of patients with pseudomyxoma peritonei from appendiceal origin treated by a strategy of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. J Clin Oncol. 2012;30:2449–56.
Elias D, Gilly F, Quenet F, et al. Pseudomyxoma peritonei: a French multicentric study of 301 patients treated with cytoreductive surgery and intraperitoneal chemotherapy. Eur J Surg Oncol. 2010;36:456–62.
Baratti D, Kusamura S, Nonaka D, et al. Pseudomyxoma peritonei: clinical pathological and biological prognostic factors in patients treated with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC). Ann Surg Oncol. 2008;15:526–34.
Stewart JHt, Shen P, Russell GB, et al. Appendiceal neoplasms with peritoneal dissemination: outcomes after cytoreductive surgery and intraperitoneal hyperthermic chemotherapy. Ann Surg Oncol. 2006;13:624–34.
Bradley RF, Stewart JHt, Russell GB, et al. Pseudomyxoma peritonei of appendiceal origin: a clinicopathologic analysis of 101 patients uniformly treated at a single institution, with literature review. Am J Surg Pathol. 2006;30:551–9.
Levine EA, Stewart JHt, Russell GB, et al. Cytoreductive surgery and intraperitoneal hyperthermic chemotherapy for peritoneal surface malignancy: experience with 501 procedures. J Am Coll Surg. 2007;204:943–53; discussion 953–5.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6,336 patients and results of a survey. Ann Surg. 2004;240:205–13.
Levine EA, Stewart JHt, Shen P, et al. Intraperitoneal chemotherapy for peritoneal surface malignancy: experience with 1,000 patients. J Am Coll Surg. 2014;218:573–85.
Glehen O, Mohamed F, Sugarbaker PH. Incomplete cytoreduction in 174 patients with peritoneal carcinomatosis from appendiceal malignancy. Ann Surg. 2004;240:278–85.
El Halabi H, Gushchin V, Francis J, et al. The role of cytoreductive surgery and heated intraperitoneal chemotherapy (CRS/HIPEC) in patients with high-grade appendiceal carcinoma and extensive peritoneal carcinomatosis. Ann Surg Oncol. 2012;19:110–4.
Halabi HE, Gushchin V, Francis J, et al. Prognostic significance of lymph node metastases in patients with high-grade appendiceal cancer. Ann Surg Oncol. 2012;19:122–5.
Lieu CH, Lambert LA, Wolff RA, et al. Systemic chemotherapy and surgical cytoreduction for poorly differentiated and signet ring cell adenocarcinomas of the appendix. Ann Oncol. 2012;23:652–8.
Sugarbaker PH, Bijelic L, Chang D, et al. Neoadjuvant FOLFOX chemotherapy in 34 consecutive patients with mucinous peritoneal carcinomatosis of appendiceal origin. J Surg Oncol. 2010;102:576–81.
Acknowledgment
This study was supported by Wake Forest University Biostatistics shared resource NCI CCSG P30CA012197.
Disclosure
Nothing to disclose
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Votanopoulos, K.I., Russell, G., Randle, R.W. et al. Peritoneal Surface Disease (PSD) from Appendiceal Cancer Treated with Cytoreductive Surgery (CRS) and Hyperthermic Intraperitoneal Chemotherapy (HIPEC): Overview of 481 Cases. Ann Surg Oncol 22, 1274–1279 (2015). https://doi.org/10.1245/s10434-014-4147-y
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-014-4147-y