
Abstract
Background
This study aimed to apply the backpropagation neural network (BPNN) to develop a model for predicting multidrug-resistant organism (MDRO) infection in critically ill patients.
Methods
This study collected patient information admitted to the intensive care unit (ICU) of the Affiliated Hospital of Qingdao University from August 2021 to January 2022. All patients enrolled were divided randomly into a training set (80%) and a test set (20%). The least absolute shrinkage and selection operator and stepwise regression analysis were used to determine the independent risk factors for MDRO infection. A BPNN model was constructed based on these factors. Then, we externally validated this model in patients from May 2022 to July 2022 over the same center. The model performance was evaluated by the calibration curve, the area under the curve (AUC), sensitivity, specificity, and accuracy.
Results
In the primary cohort, 688 patients were enrolled, including 109 (15.84%) MDRO infection patients. Risk factors for MDRO infection, as determined by the primary cohort, included length of hospitalization, length of ICU stay, long-term bed rest, antibiotics use before ICU, acute physiology and chronic health evaluation II, invasive operation before ICU, quantity of antibiotics, chronic lung disease, and hypoproteinemia. There were 238 patients in the validation set, including 31 (13.03%) MDRO infection patients. This BPNN model yielded good calibration. The AUC of the training set, the test set and the validation set were 0.889 (95% CI 0.852–0.925), 0.919 (95% CI 0.856–0.983), and 0.811 (95% CI 0.731–0.891), respectively.
Conclusions
This study confirmed nine independent risk factors for MDRO infection. The BPNN model performed well and was potentially used to predict MDRO infection in ICU patients.
Similar content being viewed by others


Introduction
Multidrug-resistant organism (MDRO) are bacteria simultaneously resistant to three or more different antibiotics. The infection caused by such bacteria is called MDRO infection [1]. Intensive care unit (ICU) patients are in critical condition and require various invasive procedures [2]. Thus, ICU is deemed the hardest-hit area for MDRO infection in hospitals [3]. Approximately 50% of ICU patients in developing countries suffer from at least one hospital-acquired infection; the corresponding rate for developed countries is 25% [4]. Antibiotic abuse and bacterial mutation have increased the number of MDRO and drug resistance [5]. The World Health Organization stated that bacterial resistance can cause a massive burden of disease, including social expenditure and medical expenditure, and will lead to a decline in global gross domestic product of 1.40–1.60% [6]. The result of a multicenter prospective cohort study showed that the 30-day mortality of patients infected with Carbapenem-resistant Klebsiella pneumoniae in China, the United States, and South America were 12.00%, 23.00%, and 28.00%, respectively [7]. However, there is no specific therapy for MDRO infection.
The risk of MDRO infection is early predicted for patients, and appropriate interventions are taken in time, the MDRO colonization rate of ICU patients can be effectively reduced, and reduce the chance of self-infection and cross-infection between patients and healthcare workers [8]. However, the drug sensitivity test and microbial culture results need 24 to 72 h to obtain, resulting in a "lag" in determining the infection status of patients. Given the potential benefits of predictive models in MDRO, many researchers have developed various models based on logistic regression (LR) to predict the risk of MDRO infection [9,10,11]. Fortunately, LR has the following shortcomings: LR requires a specific linear relationship between the independent and transformed dependent variables. Moreover, the LR model lacked the ability for self-learning and iteration. Once the time and population characteristics changed, the model tended to underperform [12].
The backpropagation neural network (BPNN), one of the most widely used deep learning methods, is a multilayer forward neural network trained according to the error backpropagation algorithm [13]. Compared with traditional LR, the advantage of BPNN is no need for prior knowledge of the mapping relationship between independent and dependent variables. As long as sufficient samples are provided for training, it can complete the nonlinear mapping from input to output variables. BPNN can accept all kinds of independent variables simultaneously without any form of variable transformation, which preserves data information to the greatest extent [14]. In addition, BPNN has strong self-learning and adaptive ability and constantly updates and improves its performance in the use process [12]. The BPNN model has been used to construct disease diagnosis and prognosis prediction models and achieved sound prediction effects [15, 16]. Nevertheless, as far as we know, no study has used it to predict the risk of MDRO infection in ICU patients. Therefore, this study aims to establish the MDRO infection model through BPNN, which identifies high-risk factors and high-risk groups of MDRO infection early and guides the implementation of interventions to reduce the incidence of MDRO infection in ICU patients.
Methods
Study population
We retrospectively collected data from patients who received treatment in the ICU of the Affiliated Hospital of Qingdao University from July 2021 to January 2022. The primary cohort enrolled 688 critically ill patients. For external validation, patients in the same study center from May 2022 to July 2022 were selected in the validation set.
All adults (aged ≥ 18 years and ≥ one-time microbial culture performed during ICU hospitalization) in ICU were enrolled in this study. Patients who died or left the ICU within 48 h, had incomplete case data or were diagnosed with MDRO infection prior to ICU admission were excluded. Only the first admission was included for analysis for patients with multiple ICU admissions during hospitalization.
This study has obtained the approval of the Ethics Committee of Qingdao University Medicine (QDU-HEC-2021173). As this study was retrospective and data were anonymized, informed consent was waived.
Data collection
We obtained patient information through hospital infection surveillance and electronic medical records systems. Initial candidate factors may be associated with MDRO infections, including general data, invasive procedures, medication, laboratory indicators, and the scores. General data included gender, age, body mass index, length of hospitalization, length of ICU stay, and comorbid diseases (including diabetes, hypertension, chronic lung disease, liver disease, chronic renal disease, congestive heart failure, and cerebrovascular disease). Invasive procedures included surgical situations, mechanical ventilation, central venous catheters, gastrointestinal decompression, peripherally inserted central venous catheters, extracorporeal membrane oxygenation, urinary tube, and other drainage tubes in ICU. Medication included antibiotic use, hormone, and nutritional support therapy during ICU. Laboratory indicators included albumin, prealbumin, C-reactive protein, procalcitonin, white blood cells, blood–urea–nitrogen, and creatinine within the first 24 h of their ICU stay. The scores included the APACHE II score, Glasgow coma scale, and nutrition risk screening (NRS)-2002 score within 24 h of admission in the ICU. The diagnosis of the combined disease was as per the International Classification of disease-10 code [17].
This study obtained specimens for microbiologic cultures from blood, urine, sputum, pus, drainage fluid, and secretions. VITEK2 Compact System automatic microbial identification and drug sensitivity analysis system were used for culture identification of strains, and the Kirby Bauer paper diffusion method was applied to the drug sensitivity test of strains. The definition of MDRO was based on the provisional standard definition of MDRO published by Magiorakos and other experts [18]. Long-term bed rest refers to being bedridden for 15 days at least, and more than 90% of the time in bed within 1 day. The surgical situation included the grading of the operation, the classification of incision, and the healing of the incision.
Screening for risk factors
Patients were categorized into MDRO-infected and non-MDRO-infected groups in accordance with the presence or absence of MDRO infection during the ICU. We combined Lasso and stepwise regression to screen risk factors. Lasso regression used tenfold cross validation to select the optimal penalty coefficient (lambda). The variables whose coefficients were not zero had a significant relationship with the dependent variable and were preserved [19]. Lasso can avoid adding too many independent variables into the BPNN model, thereby reducing the network's complexity and computation and improving the model's prediction accuracy. Then, stepwise regression was applied to further select the optimal combination of independent variables. This method was the introduction of variables one after the other. After introducing a new variable, the old variables that had been selected in the regression model were tested one by one, and the variables that were not meaningful were deleted [20]. This process continued until no new variables were introduced and no old variables were deleted. Variables with bilateral P < 0.05 were identified as independent risk factors for MDRO infection.
Development and validation of the BPNN model
These confirmed independent risk factors for MDRO infection were used as input variables to construct a BPNN model. The BPNN algorithm employed gradient descent to continuously adjust the weights and thresholds among layers through backpropagation to minimize the sum of error squares of the network [21].
These data of the primary cohort were randomly divided into a training set and a test set in an 8:2 ratio, where the training set was utilized to construct the model, and the test set was utilized to evaluate the model's ability to discriminate new samples. To further evaluate the generalization ability and universality of the model, external validation was performed by period validation, that is, patients from the same study center at different times. At this stage, patient data were mainly collected based on independent risk factors confirmed during model construction.
Statistical analysis
All variables in this study had less than 5% missing values, and mean interpolation was accomplished. Outliers were values that were less than the difference between the first quartile and 1.5 quartile spacing or more than the sum of the third quartile and 1.5 quartile spacing. Outliers in the data were replaced using mean values [22].
Continuous data were described as means ± standard deviation or median and interquartile range (IQR), and group comparisons were performed using the Students' t test or Mann–Whitney U test. Categorical data were expressed as frequency and percentage, and comparisons were made using the Chi-square or Fisher's exact test between groups.
In this study, Lasso and stepwise regression were performed using "glmnet" and "MASS" packages of R 4.2.3. The BPNN model was constructed with the "nnet" package of R 4.2.3. The model's predictive performance was evaluated in terms of calibration and discrimination. The discrimination was assessed by accuracy, sensitivity, specificity, and area under the curve (AUC). Calibration curves investigated the calibration of the model.
Results
Baseline characteristics
Figure 1 shows the flow chart of patient screening. There were 3673 patients enrolled, including 2764 and 909 patients in the primary cohort and validation set. In the primary cohort, 2031 patients were eliminated due to not meeting inclusion and exclusion criteria. Ruling out 46 patients with community-acquired MDRO infection, a total of 688 patients were identified, including 550 patients in the training set and 138 in the test set. The incidence of MDRO infection in the ICU was 15.84% (109/688), with the highest detection rate of Carbapenem-resistant Acinetobacter baumannii (CR-AB). The detection rate of other types of drug-resistant bacteria was depicted in Additional file 1: Table S1. There were 259 (37.65%) females and 429 (62.35%) males. The median age was 65.50 (IQR, 53.00–74.00) years. The body mass index was 23.88 (IQR, 21.48–26.44) kg/m2. The length of hospitalization and ICU stay were 19.00 (IQR, 11.00–29.00) days and 9.00 (IQR, 5.00–16.00) days, respectively (Table 1).

Flowchart for patients selection
Excluding 658 patients without meeting inclusion and exclusion criteria and 13 patients with non-first ICU admission, 238 patients were enrolled to validate externally. The prevalence of nosocomial infection of MDRO was 13.00% (31/288). The specific characteristics of the patients are summarized in Table 2. The comparisons of parameters between the primary cohort and validation set were presented in Additional file 1: Table S2.
Independent risk factors for MDRO infection
In our study, lasso adopted nested tenfold cross verification to select the largest lambda with mean error within one standard deviation (lambda.1se) as the optima lambda. As shown in Fig. 2, the optimal lambda was 0.033, corresponding to 11 variables with non-zero coefficients: NRS-2002 score, APACHE II, number of antibiotics and duration of combination, chronic lung disease, hypoproteinemia, invasive operation before ICU, antibiotic use before ICU, length of ICU stay, long-term bed rest.

Features selection by Lasso. A Tenfold cross validation for the optimal lambda (λ) parameter selection in the LASSO model. There are two dashed lines in the cross-validation diagram, one is the input value with the minimum Mean Square deviation and the other is the input value of the minimum Mean Squared Error(MSE). We take the value of λ with the minimum MSE as the optimal λ. B Binomial deviance curve was plotted versus log (λ), where λ is the tuning parameter Lasso regression cross-validation results. LASSO: least absolute shrinkage and selection operator
On this basis, variables were further analyzed using backward stepwise regression. APACHE II (OR 1.06, CI 1.02–1.10; P = 0.002), quantity of antibiotics (O R 1.81, CI 1.18–2.78; P = 0.002), chronic lung disease (OR 2.02, CI 1.02–3.97; P = 0.04), hypoproteinemia (OR 3.59, CI 1.21–10.35; P = 0.01), invasive operation before ICU (OR 2.20, CI 1.17–4.11; P = 0.01), antibiotics use before ICU (OR 2.95, CI 1.58–5.53; P < 0.001), length of hospitalization (OR 1.04, CI 1.02–1.10; P < 0.001), length of ICU stay (OR 1.02, CI 1.00–1.05; P = 0.04), and long-term bed rest (OR 3.69, CI 1.80–8.12; P < 0.001) were risk factors for MDRO infections (Table 3).
Construction and evaluation of the BPNN model
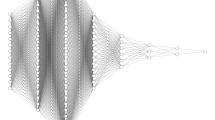
Nine independent risk factors screened above were employed as input variables to develop the BPNN model (Fig. 3). The parameters of the model were Activation (nonlinear function): logistic, hidden_layer (number of hidden layers): 1, sizes (Number of hidden layer nodes): 3, max_iter (number of iterations): 10, and linout (output function): logistic.

BPNN model for predicting MDRO infection. BPNN: backpropagation neural network; MDRO: multidrug-resistant organism
The model's prediction performance was assessed by AUC, accuracy, sensitivity, and specificity, as shown in Table 4. The AUC of the training set and test set were 0.889 and 0.919, respectively. The validation set revealed the same result (AUC = 0.811). Comparisons of the AUC for the model training set, test set, and validation set are depicted in Fig. 4. Calibration curves of the test and validation set showed that the model had good calibration ability (Fig. 5).

AUCs of the BPNN model of MDRO infection. The x-axis represents 1-specifcity, and the y-axis represents sensitivity. The part below the red, green and blue lines are the AUCs of the train, testing and validation set. AUC: area under the curve; BPNN: backpropagation neural network; MDRO: multidrug-resistant organism

Calibration curves of the BPNN model. The x-axis represents the predicted probability of MDRO infection. The y-axis represents the actual diagnosed of MDRO infection. The blue solid line represents the perfect prediction with the same predicted probability as the actual probability. The black line represents the performance of the nomogram. The closer the calibration curve of the model is to the black line, the better the model prediction is represented. A Calibration curve of the test set. B Calibration curve of the validation set. BPNN: backpropagation neural network; MDRO: multidrug-resistant organism
Features importance ranking in the BPNN model
In the BPNN model, the top 5 risk factors affecting MDRO infection were the length of hospitalization, the length of ICU stay, long-term bed rest, antibiotics use before ICU, and APACHE II (Fig. 6).

Ranking of features importance in the BPNN model. BPNN: backpropagation neural network
Discussion
In this study, we developed and validated an MDRO infection prediction model for ICU patients based on the BPNN algorithm. The model included nine scientifically and clinically accessible independent risk factors: length of hospitalization, length of ICU stay, long-term bed rest, antibiotics use before ICU, APACHE II, invasive operation before ICU, quantity of antibiotics, chronic lung disease, and hypoproteinemia. Utilizing a handful of variables, the BPNN model achieved good performance with high accuracy and sensitivity for predicting the incidence of MDRO infection in ICU patients. Furthermore, we found that the drug-resistant bacteria causing infection in ICU patients were mainly Gram-negative bacteria, especially CR-AB. CR-AB can survive for several days on dry surfaces, and can also be asymptomatic to colonize the skin, respiratory tract, and intestines. Therefore, active monitoring of CR-AB should be strengthened for the high-risk population of MDRO infection.
The prediction model can forecast the risk of individual MDRO infection based on predictors, providing theoretical support for the early identification of high-risk groups and better guidance for formulating MDRO infection management strategies [23, 24]. More and more scholars have begun to explore the construction of the MDRO infection prediction model. Wang et al. collected the data from 331 patients, adopting the method of univariate analysis followed by multivariate analysis. Finally, three risk factors were integrated to build an MDRO infection prediction model with an AUC of 0.77 (95% CI 0.70–0.84) [11]. However, the model's poor performance in predicting MDRO infection risk may be due to other valuable independent variables ignored during the data analysis. The relationships between variables in the ICU are complex, including linear or nonlinear relationships. Nevertheless, LR was used by default to deal with linear relationships between independent and dependent variables and may oversimplify complex nonlinear relationships. BPNN was widely applied in the medical field with its unique advantages, including disease diagnosis, disease classification, prognosis prediction, etc. In this study, the MDRO infection prediction model was constructed using BPNN. The AUC of the training and test sets were 0.889 and 0.918, respectively. Compared with the previous MDRO infection models [25,26,27], the prediction performance of our BPNN model constructed was improved. In addition, we collected 238 ICU patients' data for external verification. The AUC, accuracy, sensitivity, and specificity were 0.811, 0.852, 0.806, and 0.715, respectively. These results demonstrated that the BPNN model had good discrimination. That suggested that our model had good external applicability and could be used clinically for early prediction of MDRO infection in ICU patients.
In the BPNN model, length of hospitalization, length of ICU stay, long-term bed rest, antibiotics use before ICU, and APACHE II score were the top 5 predictors of MDRO infection. Length of hospitalization and ICU stay were correlated with MDRO infection in ICU patients, which agreed with the conclusions of previous studies [28]. Compared with the non-ICU environment, there are more bacterial isolates in the ICU environment, and the susceptibility is generally lower. ICU patients are more likely to be directly or indirectly exposed to MDRO [29]. As previous evidence indicated, this study also found that long-term bed rest was an independent risk factor for MDRO infection [30]. A meta-analysis showed that prior use of antibiotics, especially third-generation cephalosporin antibiotics, was higher in the multidrug-resistant Gram-negative infection group than in the non-infected group, significantly increasing Gram-negative resistance [31]. This study showed the same results: antibiotics use before ICU was an independent risk factor for MDRO infection. APACHE II score is a tool for evaluating the severity of patients' disease and predicting prognosis. The previous study found that the higher the APACHE II score, the greater the likelihood of MDRO infection and mortality [32]. This study similarly found that the APACHE II score was positively associated with MDRO infection. The previous study showed the association between MDRO and major surgery operation before admission to ICU [33], quantity of antibiotics [34], chronic lung disease [35] and hypoproteinemia [36].
This study has the following advantages. We combined Lasso and stepwise regression to screen for risk factors to avoid multiple collinearity and overfitting of variables. In addition, compared with LR, the BPNN algorithm had strong fault tolerance, nonlinear mapping ability, self-learning and adaptive ability, and generalization ability. Thus, BPNN was employed to mine data characteristics and develop our study's MDRO infection model for ICU patients.
However, it was undeniable that our study had some drawbacks. First, the current study was a single-center retrospective modeling study, which restricted us from determining causal relationships between predictors and outcomes. Therefore, further prospective clinical trials are needed to verify the validity of our model. Second, the retrospective and observational data may result in selection bias. Finally, although external validation was performed in this study, it was limited to data from the same center. In subsequent studies, the sample size can be further expanded, and multicenter studies can be added to optimize the structure of the BPNN model.
Conclusion
We combined Lasso and backward stepwise regression to screen out nine predictors and built the BPNN model for MDRO infection in ICU patients based on them. The model has proven good prediction performance, which may be an effective instrument for identifying high-risk groups of MDRO infection in the early stage and helping medical personnel intervene early to reduce the rate of MDRO infection in critically ill patients.
Availability of data and materials
The data that support the findings of this study are available on request from the corresponding author upon reasonable request.
Abbreviations
- APACHE II:
-
Acute physiology and chronic health evaluation II
- AUC:
-
Area under the curve
- BPNN:
-
Backpropagation neural network
- CR-AB:
-
Carbapenem-resistant Acinetobacter baumannii
- ICU:
-
Intensive care unit
- IQR:
-
Interquartile range
- Lasso:
-
Least absolute shrinkage and selection operator
- LR:
-
Logistic regression
- MDRO:
-
Multidrug-resistant organism
- NRS:
-
Nutrition risk screening
References
Taitt CR, Leski TA, Stockelman MG, et al. Antimicrobial resistance determinants in Acinetobacter baumannii isolates taken from military treatment facilities. Antimicrob Agents Chemother. 2014;58(2):767–81.
Iwu CD, Patrick SM. An insight into the implementation of the global action plan on antimicrobial resistance in the WHO African region: a roadmap for action. Int J Antimicrob Agents. 2021;58(4): 106411.
Golli AL, Cristea OM, Zlatian O, et al. Prevalence of multidrug-resistant pathogens causing bloodstream infections in an intensive care unit. Infect Drug Resist. 2022;15:5981–92.
Kollef MH, Bassetti M, Francois B, et al. The intensive care medicine research agenda on multidrug-resistant bacteria, antibiotics, and stewardship. Intensive Care Med. 2017;43(9):1187–97.
Fan Y, Zou J, Cao X, et al. Data on antibiotic use for detecting clusters of healthcare-associated infection caused by multidrug-resistant organisms in a hospital in China, 2014 to 2017. J Hosp Infect. 2019;101(3):305–12.
World Health Organization. Antimicrobial resistance: global report on surveillance [EB/OL]. [2023/7/25]. https://www.who.int/publications/i/item/9789241564748
Wang M, Earley M, Chen L, et al. Clinical outcomes and bacterial characteristics of carbapenem-resistant Klebsiella pneumoniae complex among patients from different global regions (CRACKLE-2): a prospective, multicentre, cohort study. Lancet Infect Dis. 2022;22(3):401–12.
Salomão MC, Freire MP, Boszczowski I, et al. Increased risk for carbapenem-resistant enterobacteriaceae colonization in intensive care units after hospitalization in emergency department. Emerg Infect Dis. 2020;26(6):1156–63.
González Del Castillo J, Julián-Jiménez A, Gamazo-Del Rio JJ, et al. A multidrug-resistant microorganism infection risk prediction model: development and validation in an emergency medicine population. Eur J Clin Microbiol Infect Dis. 2020;39(2):309–23.
Seo SM, Jeong IS, Song JY, et al. Development of a nomogram for carbapenem-resistant enterobacteriaceae acquisition risk prediction among patients in the intensive care unit of a Secondary Referral Hospital. Asian Nurs Res. 2021;15(3):174–80.
Wang L, Huang X, Zhou J, et al. Predicting the occurrence of multidrug-resistant organism colonization or infection in ICU patients: development and validation of a novel multivariate prediction model. Antimicrob Resist Infect Control. 2020;9(1):66.
Wei W, Yang X. Comparison of diagnosis accuracy between a backpropagation artificial neural network model and linear regression in digestive disease patients: an empirical research. Comput Math Methods Med. 2021;2021:6662779.
Wang Z, Zhou L, Hao W, et al. Comparative antioxidant activity and untargeted metabolomic analyses of cherry extracts of two Chinese cherry species based on UPLC-QTOF/MS and machine learning algorithms. Food Res Int. 2023;171: 113059.
Carracedo-Reboredo P, Liñares-Blanco J, Rodríguez-Fernández N, et al. A review on machine learning approaches and trends in drug discovery. Comput Struct Biotechnol J. 2021;19:4538–58.
Jovanovic P, Salkic NN, Zerem E. Artificial neural network predicts the need for therapeutic ERCP in patients with suspected choledocholithiasis. Gastrointest Endosc. 2014;80(2):260–8.
Li Z, Li Y. A comparative study on the prediction of the BP artificial neural network model and the ARIMA model in the incidence of AIDS. BMC Med Inform Decis Mak. 2020;20(1):143.
Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–9.
Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–81.
Cai W, van der Laan M. Nonparametric bootstrap inference for the targeted highly adaptive least absolute shrinkage and selection operator (LASSO) estimator. Int J Biostat. 2020. https://doi.org/10.1515/ijb-2017-0070.
Tang X, Bai G, Wang H, et al. Elaboration of multiparametric MRI-based radiomics signature for the preoperative quantitative identification of the histological grade in patients with non-small-cell lung cancer. J Magn Reson Imaging. 2022;56(2):579–89.
Sun Q, Zheng J, Zhang Y, et al. Altered spontaneous brain activities in maintenance hemodialysis patients with cognitive impairment and the construction of cognitive function prediction models. Ren Fail. 2023;45(1):2217276.
Zhang Z. Multiple imputation with multivariate imputation by chained equation (MICE) package. Ann Transl Med. 2016;4(2):30.
Moons KG, Royston P, Vergouwe Y, et al. Prognosis and prognostic research: what, why, and how? BMJ (Clinical research ed). 2009;338: b375.
Steyerberg EW, Moons KG, van der Windt DA, et al. Prognosis Research Strategy (PROGRESS) 3: prognostic model research. PLoS Med. 2013;10(2): e1001381.
Mora-Jiménez I, Tarancón-Rey J, Álvarez-Rodríguez J, et al. Artificial intelligence to get insights of multi-drug resistance risk factors during the First 48 hours from ICU admission. Antibiotics (Basel, Switzerland). 2021;10(3):239.
Vasudevan A, Mukhopadhyay A, Li J, et al. A prediction tool for nosocomial multi-drug Resistant Gram-Negative Bacilli infections in critically ill patients - prospective observational study. BMC Infect Dis. 2014;14:615.
Song JY, Jeong IS. Development of a risk prediction model of carbapenem-resistant Enterobacteriaceae colonization among patients in intensive care units. Am J Infect Control. 2018;46(11):1240–4.
Caglayan C, Barnes SL, Pineles LL, et al. A data-driven framework for identifying intensive care unit admissions colonized with multidrug-resistant organisms. Front Public Health. 2022;10: 853757.
Sader HS, Farrell DJ, Flamm RK, et al. Antimicrobial susceptibility of Gram-negative organisms isolated from patients hospitalized in intensive care units in United States and European hospitals (2009–2011). Diagn Microbiol Infect Dis. 2014;78(4):443–8.
Huang SF, Chang JS, Sheu CC, et al. An antibiotic decision-making tool for patients with pneumonia admitted to a medical intensive care unit. Int J Antimicrob Agents. 2016;48(3):286–91.
Ang H, Sun X. Risk factors for multidrug-resistant Gram-negative bacteria infection in intensive care units: a meta-analysis. Int J Nurs Pract. 2018;24(4): e12644.
Baek JE, Choi IH, Cho YW, et al. Clinical characteristics and outcomes of Clostridioides difficile infection in the intensive care unit: a KASID multi-centre study. J Hosp Infect. 2023;139:106–12.
Boscolo A, Sella N, Pettenuzzo T, et al. Multidrug-resistant and extended-spectrum β-lactamase gram-negative bacteria in bilateral lung transplant recipients: incidence, risk factors, and in-hospital mortality. Chest. 2022;162(6):1255–64.
Versporten A, Zarb P, Caniaux I, et al. Antimicrobial consumption and resistance in adult hospital inpatients in 53 countries: results of an internet-based global point prevalence survey. Lancet Glob Health. 2018;6(6):e619–29.
Sirichayanugul T, Srisawat C, Thummakomut C, et al. Development and internal validation of simplified predictive scoring (ICU-SEPSA score) for mortality in patients with multidrug resistant infection. Front Pharmacol. 2022;13: 938028.
Zhou T, Yang W, Yang Q, et al. Distribution, diagnosis, and analysis of related risk factors of multidrug-resistant organism in patients with malignant neoplasms. Int J Clin Exp Pathol. 2020;13(10):2648–55.
Acknowledgements
We acknowledge the patients who participated in this study.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Conceptualization: YW, GW, SG, XP; methodology: YW, GW; investigation: YW, YZ, CC, JL, JY; formal analysis: YW, YZ, CW, GW; writing—original draft: YW, CC, YD; writing—review and editing: YW, GW, SG, XP; supervision: SG, XP. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The research contents and research programs were reviewed and approved by the Ethics Committee of Qingdao University Medicine (QDU-HEC-2021173). As this study was retrospective and data were anonymized, informed consent was waived.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Table S1
. Frequency of isolated MDRO species. Table S2. Comparison of patients’ demographic and clinical characteristics in the primary cohort and validation set.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, Y., Wang, G., Zhao, Y. et al. A deep learning model for predicting multidrug-resistant organism infection in critically ill patients. j intensive care 11, 49 (2023). https://doi.org/10.1186/s40560-023-00695-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40560-023-00695-y