
Abstract
Background
Physical restraint has been commonly indicated to patients with brain dysfunction in neurocritical care. The effect of physical restraints on outcomes of critically ill adults remains controversial as no randomized controlled trials have compared its safety and efficacy, and the association between physical restraint requirement and neurological outcome in patients with subarachnoid hemorrhage (SAH) has not been fully examined. The aim of this study was to examine the association between physical restraint requirement and neurological outcomes in patients with SAH.
Methods
A single-center, retrospective study was conducted on patients with acute phase SAH treated for > 72 h in the intensive care unit from 2014 to 2020. Patients were divided into three groups based on the amount of time required for physical restraint during the first 24–72 h after admission: no, intermittent, and continuous use of physical restraint. Unfavorable neurologic outcome, assessed using the modified Rankin scale upon hospital discharge, has been considered as primary end point.
Results
Overall, 101 patients were included in the study, with 52 patients (51.5%) having unfavorable neurological outcomes. Among them, 46 patients (45.5%) did not use physical restraint, and 55 (54.5%) patients used physical restraint during the first 24–72 h after admission: 26 (25.7%) intermittent and 29 (28.7%) continuous. Multivariable logistic regression analysis showed that continuous use of physical restraint during the first 24–72 h after admission was significantly associated with unfavorable neurological outcomes in patients with SAH (odds ratio, 3.54; 95% confidence interval, 1.05–13.06; p = 0.042) compared with no physical restraint.
Conclusions
Continuous use of physical restraint during the first 24–72 h after admission was more significantly associated with unfavorable neurological outcomes than no physical restraint among patients with SAH during the acute phase.
Similar content being viewed by others

Background
Physical restraint defined as “any manual method, physical, or mechanical device, material, or equipment that immobilizes or reduces the ability of a patient’s movement” have been commonly indicated for patients with brain dysfunction in neurocritical care [1,2,3]. Its effect on outcomes of critically ill adult patients remains controversial as no randomized controlled trials (RCTs) have compared its safety and efficacy [1, 4].
Agitation, consciousness fluctuation, and delirium after a subarachnoid hemorrhage (SAH) have been associated with unfavorable neurological outcome [5,6,7]. However, the association between physical restraint requirement and neurological outcomes in patients with SAH has not been fully examined.
Therefore, this study aimed to examine the association between physical restraint requirement and neurological outcome in patients with SAH.
Methods
Study design and setting
This single-center, retrospective study was conducted at the Kagawa University Hospital, a 613-bed teaching institution with an 8-bed intensive care unit (ICU) managed by a neurointensivist. Medical records were reviewed with the approval of the institutional review board (approval number: 2020-053) and in accordance with the ethical standards established in the 1964 Declaration of Helsinki and its later amendments. The requirement for patient consent was waived due to the retrospective nature of the study.
Study participants and inclusion criteria
We included patients aged ≥ 18 years who were consecutively admitted to the ICU between July 1, 2014 and July 31, 2020, with a confirmed diagnosis of aneurysmal SAH. Patients who met the following inclusion criteria were included: acute phase of SAH treated for > 72 h in the ICU. Exclusion criteria were patients who did not undergo treatment (coil or clip) for aneurysmal SAH, patients provided with comfort care only, or patients admitted to the ICU for < 72 h. Additionally, those with Hunt and Kosnik (H & K) grade 5, Richmond Agitation–Sedation Scale (RASS) score of − 5, or neuromuscular blockade use during the first 24–72 h after admission were excluded.
General management of SAH in the ICU
All patients were managed in accordance with Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage by the American Heart Association/American Stroke Association [8]. In addition to the general intensive care, all patients were monitored for clinical deterioration or cerebral infarction development due to delayed cerebral ischemia (DCI). Fever was treated aggressively with acetaminophen, nonsteroidal anti-inflammatory medications, or cooling devices.
Analgosedation management
A meeting was held every morning and evening, and the depth of sedation was determined in patients undergoing mechanical ventilation. The depth of sedation was assessed using the RASS [9, 10]. If increased intracranial pressure was noted or highly suspected, deep sedation targeting a RASS score of − 5 with neuromuscular blockade was initiated as needed. The minimum amount of sedatives, such as propofol, midazolam, or dexmedetomidine (DEX), which were necessary to prevent ventilator dyssynchrony and patient discomfort, were used. Analgesics, including acetaminophen, nonsteroidal anti-inflammatory medications, and fentanyl, were administered as required. Each physician was responsible for the choice of sedatives.
Physical restraint
Physical restraint was initiated based on the RASS score. Examples of physical restraints include Mitten restraints, vests, straps/belts, limb ties, and bedside rails [11].
RASS − 3 to − 1: Delirium is assessed using the Confusion Assessment Method for the ICU (CAM-ICU). Physical restraint is considered in patients receiving mechanical ventilation to prevent accidents.
RASS 0: Basically, physical restraint was initiated, but only occasionally when patients are expected to experience delirium at night time to prevent accidents.
RASS ≥ 1: Analgesia and sedative drugs were titrated to obtain the RASS-2 in patients receiving mechanical ventilation. In patients expected to pull or remove tubes or catheters, Mitten restraints were used in addition to limb ties. Further, application of vests was considered to prevent accidental events.
Assessment of delirium in SAH patients in the ICU
Delirium was assessed by ICU nurses. ICU patients were routinely assessed for the occurrence of delirium through the CAM-ICU. In addition, delirium was defined based on a positive RASS score, or bedside nurse’s judgments according to the presence of agitation, hallucination, dangerous behavior, and use of pharmacologic treatments for agitation and hyperactive delirium such as antipsychotic drugs (risperidone or haloperidol). During the ICU stay, delirium was assessed three times a day and when patient’s status changed. Delirium during the first 48–72 h after admission was obtained to clarify the phase differences between physical restraint requirement and delirium development.
Data sampling
The following data were collected: age, sex, H & K grade, Fisher score, World Federation Neurological Surgeons (WFNS) grade, treatment modality (coil or clip), sedatives and analgesia administration, RASS score, physical restraint duration during the first 24–72 h after admission (no, intermittent, and continuous use of physical restraint), delirium during the first 48–72 h after admission, laboratory data on admission, aneurysm location [12], modified Rankin scale (mRS) upon hospital discharge, DCI rate, mechanical ventilation duration, ICU stay duration, hospital stay duration, and hospital mortality.
The physical restraint duration was determined during the first 24–72 h after admission because various treatment strategies (emergency surgical operation or angiography with general anesthesia, deep sedation followed by treatment on the next day, computed tomography followed by treatment, and so on) were initiated for the first 24 h; therefore, this phase was excluded in the present study.
Continuous physical restraint was defined as the patients who required continuous physical restraint during the first 24–72 h after admission. Intermittent physical restraint was defined as the patients who required any physical restraint during the first 24–72 h after admission.
Outcome measures
Unfavorable neurologic outcome was considered as the primary end-point, which was assessed using the mRS upon hospital discharge [13]. mRS is a global disability measurement tool and comprises seven outcome categories: no symptoms at all, no significant disability, slight disability, moderate disability, moderately severe disability, severe disability, and death. All patients with SAH were examined in real time using mRS upon hospital discharge and listed their medical records. The neurologic outcome was defined as unfavorable when the mRS score was 3–6 and as favorable when the mRS score was 0–2. The secondary outcome was the occurrence of delirium evaluated by ICU nurses.
Statistical analysis
To obtain the association between physical restraint in the acute phase and neurological outcomes, patients were divided into three groups based on the amount of time required for physical restraint during the first 24–72 h after admission: no, intermittent, and continuous use of physical restraint. Demographic factors and baseline characteristics were summarized using descriptive statistics. The groups were compared using Kruskal–Wallis test or Mann–Whitney U test, and categorical comparisons were drawn using the Fisher’s exact test or chi-square test, as deemed appropriate. Univariate and multivariate analyses were performed to explore independent factors that predicted the unfavorable neurologic outcomes. Covariates of age (> 65 years), H & K grade, treatment modality (coil or clip), aneurysm location (anterior cerebral arteries or not), and physical restraint were included in the multivariable analysis. The Cochran–Armitage trend test was used to examine the trend between physical restraint during the first 24–72 h after admission and incidence of delirium during the first 48–72 h after admission. Subgroup analysis was performed on patients with RASS of ≥ − 2 and Hunt & Kosnik grade of 1–3. We also repeated the analysis using different definitions of physical restraint during the first 24–72 h after admission as a continuous variable. Statistical analyses were performed using the JMP version 12 statistical software (SAS Institute, Cary, NC, USA). A two-sided p value < 0.05 was considered statistically significant for all analyses. Missing data were not replaced or estimated.
Results
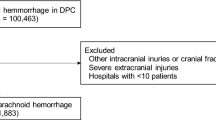
Among 129 patients with SAH who were admitted to the ICU, 119 met the inclusion criteria. Among those who met the inclusion criteria, 18 were excluded due to H & K grade 5 or RASS-5 without analgosedation or neuromuscular blockade use during the first 24–72 h after admission. The remaining 101 patients were ultimately included for analyses (Fig. 1).

Patient flow
Baseline characteristics of the study population
The study population included 101 patients (median age, 65 years; 58 (57.4%) were women). Unfavorable neurological outcomes were observed in 52 patients (51.5%) (Table 1).
Among them, 46 patients (45.5%) did not use physical restraint and 55 (54.5%) patients used physical restraint during the first 24–72 h after admission: 26 (25.7%) intermittent and 29 (28.7%) continuous. The median duration of physical restraint during the first 24–72 h after admission was 11 h (interquartile range, 0–48). Their distribution is shown in Supplemental Figure 1.
Baseline characteristics were compared according to three groups of physical restraint during the first 24–72 h after admission. Significant differences were observed in the outcome at discharge and duration of mechanical ventilator use. The proportion of unfavorable outcome at discharge was 37.0, 53.9, and 72.4% in patients with no, intermittent, and continuous use of physical restraint, respectively (Table 1). A comparison of baseline characteristics according to favorable and unfavorable outcomes is shown in Supplemental Table 1.
Association between physical restraint and sedative and antipsychotic medication use
Among three groups, a significant difference was observed in incidences of propofol and DEX use (Table 2). Regarding the evaluation of RASS score, the differences in maximum and minimum RASS score, agitated state (RASS ≥ 1), and deep sedation (RASS score ≤ − 3) were also significant among the three groups. Differences in antipsychotic medications use were not significant (Table 2).
Multivariable logistic regression analysis
Regarding the primary outcome, this study found that continuous use of physical restraint during the first 24–72 h after admission was significantly associated with unfavorable neurological outcomes at discharge in patients with SAH (odds ratio (OR), 3.54; 95% confidence interval (CI), 1.05–13.06; p = 0.042) compared with no physical restraint (Table 3).
Association between physical restraint and delirium
Among all participants, delirium during the first 48–72 h after admission was assessed in 85 patients and was found in 37 patients (43.5%). A linear trend was observed in the development of delirium among three groups (4 patients (10.8%) in the no physical restraint, 12 (50.0%) in the intermittent, and 21 (87.5%) in the continuous; p < 0.001) (Fig. 2).

Associations between physical restraint during the first 24–72 h after admission and delirium during the first 48–72 h after admission. The proportion of delirium during the first 48–72 h after admission was 4 patients (10.8%) in the no physical restraint, 12 (50.0%) in the intermittent, and 21 (87.5%) in the continuous. Error bars indicate 95% confidence interval
Subgroup and sensitivity analysis
In patients with RASS of ≥ − 2 during the first 24 to 72h after admission, continuous use of physical restraint was significantly associated with unfavorable neurological outcomes at discharge than no physical restraint in patients with SAH (OR, 6.88; 95% CI, 1.69–32.36; p = 0.007). In patients with H & K grade (1–3) on admission, continuous use of physical restraint during the first 24 to 72h after admission was more significantly associated with unfavorable neurological outcomes at discharge than no physical restraint in patients with SAH (OR, 6.94; 95% CI, 1.66–33.92; p = 0.007) (Table 4). In the analysis using different definitions of physical restraint during the first 24–72 h after admission as a continuous variable, physical restraint was significantly associated with unfavorable outcomes (OR, 1.13; 95% CI, 1.01–1.28; p = 0.039; Table 4).
Discussion
In this study, continuous use of physical restraint during the first 24–72 h after admission was found to be more significantly associated with unfavorable neurological outcomes at discharge than no physical restraint in patients with SAH. Continuous use of physical restraint during the first 24–72 h after admission was also associated with the occurrence of delirium during the first 48–72 h ICU stay.
A recent study performed by Reznik et al. demonstrated that a longer duration of agitation in the acute setting may be associated with more favorable outcomes in patients with SAH with RASS score > 0 [6]. This result seemed to be inconsistent with the results of the present study. Moreover, even in the subgroup analysis limited to patients with RASS ≥ − 2 during the first 24–72 h after admission in the present study, the stronger conclusion that continuous use of physical restraint during the first 24–72 h after admission was more significantly associated with unfavorable neurological outcomes than no physical restraint was obtained. Because Reznik et al. included only patients with RASS scores > 0 and assessed outcome at 3 months, the populations and outcomes of the two studies were not the same. In addition, because agitation was not evaluated directly in the present study, the discrepancy between two studies could not be confirmed precisely. Further study is required to establish whether the cause is due to a difference in analysis, a difference in race, or other factors.
The increasing exposure of patients to potentially harmful sedative and antipsychotic medications can be reduced with the use of physical restraint [14]; however, sedative drug use such as midazolam and propofol was paralleled to physical restraint in this study because the target sedation could not be reached even if the appropriate sedative dose was used. The use of sedatives decreased in parallel with the minimum RASS score, but increased in parallel with the maximum RASS score in this study. Other reasons include the fact that in the case of deepening sedation, physical restraint is also used because bedside nurses feel that patients should not be moved frequently. That feeling gets stronger, which is a psychological characteristic of Japanese. In neurocritically ill patients, delirium was independently associated with worse neurological outcome [7, 15], and continuous use of physical restraint was associated with the occurrence of delirium in the acute phase in this study. In the present study, information on delirium during the first 48–72 h after admission was obtained to clarify the phase differences between physical restraint requirement and development of delirium. Of the 37 patients with delirium during 48–72 h after admission, 31 (84%) had already required physical restraint, including intermittent and continuous restraints before 48 h after admission. Thus, continuous use of physical restraint during the first 24–72 h after admission was considered to be more associated with unfavorable neurological outcomes. Another hypothesis could be that the patients with no physical restraint had a shorter ventilation period than those in the two physical restraint groups. Thus, more patients with good consciousness levels after initial treatment might have been included in the no physical restraint group. However, in our subgroup analysis, the significant association between the physical restraint requirement and unfavorable outcome persisted in a limited number of patients with non-severe SAH (H&K grade 1–3).
Although physical restraint was the exposure, not the intervention in the present study, the hypothesis that continuous use of physical restraint during the first 24–72 h after admission was more significantly associated with unfavorable neurological outcomes than no physical restraint might be generated. In addition, our subgroup analysis results suggested that its association in patients with non-severe SAH (H&K grade 1–3) was stronger than primary analysis. However, application of physical restraint is closely associated with sedative and antipsychotic medication use [16,17,18]. Moreover, no RCT has explored the safety and efficacy of physical restraint use in critically ill adult patients [1]. Thus, further study to explore the safety and efficacy of physical restraint for patients with SAH will be required. In the study, establishing appropriate outcomes such as post-aSAH syndrome [19], and harmful sedative and antipsychotic medication use to prevent self-extubation, tube dislodgement, and/or medical device removal may be required.
This study has several limitations that should be addressed. First, this was a retrospective single-center study with a small sample size; hence, the possible selection bias and uncontrolled confounding factors should be considered. Moreover, some patients who received unrecorded physical restraints might have been categorized into the no physical restraint group, which could be a misclassification bias. Further RCT or prospective and multicenter studies are warranted to confirm our findings. Second, no physical restraint criteria have been established. Although the treatment management was decided by discussion at the conference, the person in charge of the neurointensive care unit was the same throughout the study period, and no major change was made in the treatment protocol for physical restraint and sedation. Third, the details of the devices for physical restraint were not examined because of the small sample size. Finally, as the primary end point was unfavorable neurological outcome at hospital discharge, differences in the time of evaluation may have affected the results. Further studies to evaluate with long-term outcomes are needed.
Conclusions
This study found that continuous use of physical restraint during the first 24–72 h after admission was significantly more associated with unfavorable neurological outcomes than no physical restraint at discharge in patients with SAH.
Availability of data and materials
The datasets used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Abbreviations
- SAH:
-
Subarachnoid hemorrhage
- ICU:
-
Intensive care unit
- RASS:
-
Richmond Agitation–Sedation Scale
- DCI:
-
Delayed cerebral ischemia
- DEX:
-
Dexmedetomidine
- CAM-ICU:
-
Confusion Assessment Method for the ICU
- WFNS:
-
World Federation Neurological Surgeons
- mRS:
-
Modified Rankin scale
- OR:
-
Odds ratio
- CI:
-
Confidence interval
References
Devlin JW, Skrobik Y, Gelinas C, Needham DM, Slooter AJC, Pandharipande PP, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46(9):e825–e73.
Meyfroidt G, Smith M. Focus on delirium, sedation and neuro critical care 2019: towards a more brain-friendly environment? Intensive Care Med. 2019;45(9):1292–4.
Mion LC. Physical restraint in critical care settings: Will they go away? Geriatr Nurs. 2008;29(6):421–3.
Unoki T, Sakuramoto H, Ouchi A, Fujitani S, Japanese Society of Education for P, Trainees in Intensive Care Nursing Research G. Physical restraints in intensive care units: a national questionnaire survey of physical restraint use for critically ill patients undergoing invasive mechanical ventilation in Japan. Acute Med Surg. 2019;6(1):68–72.
Reznik ME, Schmidt JM, Mahta A, Agarwal S, Roh DJ, Park S, et al. Agitation after subarachnoid hemorrhage: a frequent omen of hospital complications associated with worse outcomes. Neurocrit Care. 2017;26(3):428–35.
Reznik ME, Mahta A, Schmidt JM, Frey HP, Park S, Roh DJ, et al. Duration of agitation, fluctuations of consciousness, and associations with outcome in patients with subarachnoid hemorrhage. Neurocrit Care. 2018;29(1):33–9.
Oldenbeuving AW, de Kort PL, Jansen BP, Algra A, Kappelle LJ, Roks G. Delirium in the acute phase after stroke: incidence, risk factors, and outcome. Neurology. 2011;76(11):993–9.
Connolly ES Jr, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2012;43(6):1711–37.
Sessler CN, Gosnell MS, Grap MJ, Brophy GM, O'Neal PV, Keane KA, et al. The Richmond Agitation-Sedation Scale: validity and reliability in adult intensive care unit patients. Am J Respir Crit Care Med. 2002;166(10):1338–44.
Riker RR, Fugate JE. Clinical monitoring scales in acute brain injury: assessment of coma, pain, agitation, and delirium. Neurocrit Care. 2014;21(Suppl 2):S27–37.
Retsas AP. Survey findings describing the use of physical restraints in nursing homes in Victoria, Australia. Int J Nurs Stud. 1998;35(3):184–91.
Jaja BN, Lingsma H, Steyerberg EW, Schweizer TA, Thorpe KE, Macdonald RL. Neuroimaging characteristics of ruptured aneurysm as predictors of outcome after aneurysmal subarachnoid hemorrhage: pooled analyses of the SAHIT cohort. J Neurosurg. 2016;124(6):1703–11.
Banks JL, Marotta CA. Outcomes validity and reliability of the modified Rankin scale: implications for stroke clinical trials: a literature review and synthesis. Stroke. 2007;38(3):1091–6.
Shehabi Y, Bellomo R, Reade MC, Bailey M, Bass F, Howe B, et al. Early intensive care sedation predicts long-term mortality in ventilated critically ill patients. Am J Respir Crit Care Med. 2012;186(8):724–31.
Naidech AM, Beaumont JL, Rosenberg NF, Maas MB, Kosteva AR, Ault ML, et al. Intracerebral hemorrhage and delirium symptoms. Length of stay, function, and quality of life in a 114-patient cohort. Am J Respir Crit Care Med. 2013;188(11):1331–7.
Benbenbishty J, Adam S, Endacott R. Physical restraint use in intensive care units across Europe: the PRICE study. Intensive Crit Care Nurs. 2010;26(5):241–5.
De Jonghe B, Constantin J-M, Chanques G, Capdevila X, Lefrant J-Y, Outin H, et al. Physical restraint in mechanically ventilated ICU patients: a survey of French practice. Intensive Care Med. 2013;39(1):31–7.
Luk E, Sneyers B, Rose L, Perreault MM, Williamson DR, Mehta S, et al. Predictors of physical restraint use in Canadian intensive care units. Crit Care. 2014;18(2):R46.
Haug Nordenmark T, Karic T, Roe C, Sorteberg W, Sorteberg A. The post-aSAH syndrome: a self-reported cluster of symptoms in patients with aneurysmal subarachnoid hemorrhage. J Neurosurg. 2019;132(5):1556–1565.
Acknowledgements
None
Funding
None
Author information
Authors and Affiliations
Contributions
KA and AI contributed equally to this work. TH takes responsibility for the paper as a whole. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the institutional review board of the Kagawa University Hospital (approval number: 2020-053). The requirement for patient consent was waived due to the retrospective nature of the study.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplemental Figure 1.
Distribution of physical restraint duration during the first 24–72 h after admission. Continuous physical restraint was defined as the patients who required continuous physical restraint during the first 24–72 h after admission. Intermittent physical restraint was defined as the patients who required any physical restraint during the first 24–72 h after admission.
Additional file 2: Supplemental Table 1.
Comparison of baseline characteristics with favorable (mRS 0–3) and unfavorable (mRS 4–6) outcomes.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Akiyama, K., Inoue, A., Hifumi, T. et al. Association between physical restraint requirement and unfavorable neurologic outcomes in subarachnoid hemorrhage. j intensive care 9, 24 (2021). https://doi.org/10.1186/s40560-021-00541-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40560-021-00541-z