
Abstract
Background
Pharmacists must cater to seniors’ needs and communicate better in delivering pharmaceutical care. However, pharmaceutical care for seniors is unique since they commonly depend on support from their social environment. Our study aimed to collect perceptions and experiences of Asian seniors regarding social support.
Methods
A qualitative systematic review of peer-reviewed articles between January 2012 and January 2022 was conducted using PubMed, Scopus, Academic Search Complete via EBSCOhost, ProQuest, and Google Scholar. Selected studies were extracted, and thematic synthesis was performed.
Results
A total of 23 qualitative studies with diverse rigor were included in this review. Themes that emerged around perceptions and experiences of social support were (1) family orientation, (2) having faith in religion, (3) the importance of the elderly providing support, (4) taboos, (5) elderly self-reliance, (6) elderly fear of being a burden, and (7) differences on perceptions and experiences regarding social support. A discussion on how these results may contribute to pharmacy practice is provided.
Conclusion
This study reviews the available social support for seniors and highlights its importance for pharmacists.
Similar content being viewed by others

Background
The role of pharmacists in providing pharmaceutical care for seniors is rising due to an aging population worldwide. The global population aged 60 and over reached 1 billion in 2019 and was estimated to increase to 2.1 billion in 2050 [1]. Nevertheless, those aged 60 and over are generally prone to develop medication‐related problems, such as adverse drug reactions [2], poor adherence to therapy, and inappropriate drug selection [3], because of several health conditions and the use of poly-medication to control their comorbidities. This condition challenges pharmacists to provide more patient-oriented pharmaceutical services.
Providing pharmaceutical care for seniors differs from other populations. It needs more comprehension, with proficiency not only in the clinical aspects but also in the social context in which the pharmaceutical service is delivered [4, 5]. For instance, to improve treatment adherence and prevent medication-related problems, pharmacists must not only know the pharmacokinetic–pharmacodynamic changes in seniors but also notice the need for and availability of family and neighborhood support.
Social support is one of seniors' most important social determinants of health [6, 7]. It is defined as “an exchange of resources between two individuals perceived by the provider or the recipient to be intended to enhance the well-being of the recipient” [8]. The types of support are usually emotional, instrumental or tangible, informational, and appraisal [9]. The expression of emotional caring or concern, the instrumental aid, the provision of advice and guidance, and the encouragement to take opportunities are examples of each type of social support subsequently [10, 11].
It is known that seniors are in greater need of social support than adults, regarding not only receiving but also providing support [12]. Social support is important because later life is related to stressful events such as health problems, a close person’s illness or death, and loss of sources of income [13]. With declining physical and mental capacities leading to geriatric syndromes, many seniors also need informal support in medication management activities, such as obtaining medications, preparing pill boxes, assisting in medication administration, organizing and tracking medications, collecting information, and making treatment decisions [14].
However, it is also known that cultural differences play an important aspect in social support [15]. In Asia, seniors rely on their children and family members for care in old age. Multigenerational co-residence and extended family practice are also prevalent in many Asian countries [16].
Previous quantitative studies have shown that social support was essential to medication adherence in the senior population [17,18,19,20]. However, there was scarcely discussion on how seniors perceived and received social support and how understanding that support could equip pharmacists for their practice. Knowledge of social support from the perspective of Asian seniors could help pharmacists appreciate the nature of seniors’ social environment to provide pharmaceutical care that meets their needs, especially in the Asian pharmacy practice. Accordingly, we aimed to collect all available qualitative evidence and use individual qualitative data. The following research question was formulated: What themes emerged around social support from the perspective of Asian seniors?
Methods
Design, protocol registration, and reporting
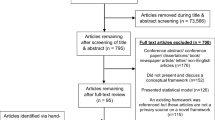
This study was conducted as a qualitative systematic review. The protocol was registered in PROSPERO (CRD42022301602). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [21] flow chart was used for the search process, and the Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) statement [22] was used to guide a more specific reporting of a qualitative systematic review.
Data sources and search strategy
PubMed, Scopus, Academic Search Complete via EBSCOhost, ProQuest, and Google Scholar were searched using predetermined search concepts and related terms (Table 1).
We define social support as emotional, instrumental, informational, and appraisal support perceived or received by the elderly [9]. We did not limit the search to the concept of pharmacist or medicine to obtain a greater possibility of social support studies (pre-planned). Therefore, the reviewers involved were medical sociologists, geriatricians, and pharmacists.
Eligibility criteria
Full-text and peer-reviewed studies with Asian seniors as participants (60 years or older) living in Asian countries, aimed at exploring perception and experience about social support or resulting in any perception and experience regarding social support, published in English, from January 2012 to January 2022, were sought. We included any settings (community, healthcare, nursing homes) and a wide range of health conditions (physical and mental health, well-being) of the participants but excluded cognitive impairment since the condition would affect perceptions or conveying experiences of seniors. Qualitative data were defined as first-order (participants’ quotes) or second-order constructs (researcher interpretation, statements, assumptions, and ideas) [23]. Therefore, a mixed-method study would be included for the qualitative parts. We also excluded study protocols, reviews, comments, editorials, and qualitative evaluations of a social support intervention.
Study selection and extraction
All titles and abstracts retrieved from the database searches were sent to the Mendeley reference manager. After removing duplicates, two team members altogether screened all titles and abstracts to identify studies that could meet the inclusion and exclusion criteria. The full texts of potentially eligible studies were retrieved, assessed, and extracted independently using a data extraction sheet.
Quality assessment
The quality of the included studies was evaluated independently by two team members using the Critical Appraisal Skills Programme (CASP) appraisal tool for qualitative research [24]. Differences of opinion were resolved by consensus. We assessed the included studies for the scope and purpose, design, reflexivity, ethical consideration, analysis and interpretation, and transferability [25] to describe the rigor of the studies. We added a percentage of the + (answer yes) after each CASP 10-question to summarize the study appraisal. This summary would not be a reason to exclude the already included study.
Data synthesis
Two team members conducted a thematic synthesis with an inductive approach that consists of three stages: the free line-by-line coding of the findings of primary studies, the organization of these free codes into related areas to construct descriptive themes, and the development of analytical themes [26]. All the texts labeled as Results or Findings in the included study were entered verbatim into QSR’s NVivo 12 Pro software for qualitative data analysis. The lines of text from a study were coded according to their meaning. The lines of text from the next studies were then coded into pre-existing or new codes. Descriptive themes were created to capture the essence of groups of initial codes. Analytical themes were then made from a group of descriptive themes to address the perceptions and experiences of social support. These stages were dependent on the judgment and insights of the reviewers. To address the heterogeneity of the included studies, we stratified the studies by settings and then identified settings of primary studies that constitute themes.
Results
Characteristics of the included studies and quality assessment
Twenty-three studies were included in this review after a search utilizing the PRISMA chart (Fig. 1). The total number of seniors who participated in the included studies was 527 individuals aged 60–94. Table 2 provides the relevant study characteristic data for the 23 included studies. The studies initially might not seek experience or perception of seniors regarding social support, but the themes obtained as the results were about support in various circumstances. Additional file 1 summarizes the quality assessment of the included studies.

PRISMA chart
Perceptions and experiences of Asian seniors regarding social support
We identified seven analytical themes on how Asian seniors perceive and experience social support: (1) family orientation, (2) having faith in religion, (3) the importance of the elderly providing support, (4) taboos, (5) elderly self-reliance, (6) elderly fear of being a burden, and (7) differences on perceptions and experiences regarding social support. The first analytical theme, “family orientation,” was prominent since 22 out of 23 studies showed experiences and perceptions of support for family [27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48]. This analytical theme was built upon many descriptive themes and codes which showed that family almost always be the directions or underlying view of mind. The second analytical theme, “having faith in religion,” was also prominent since 17 of 23 articles showed experiences and perceptions of support for seniors’ religious faith [27, 28, 32,33,34,35,36,37,38,39, 41,42,43, 45,46,47, 49]. Table 3 provides the themes, examples of quotations, and settings of primary studies that constitute themes.
Although Asian seniors were thought to rely on family, some included studies provided the perspectives of seniors who have no family or live without family. They tend to act practically than rely on praying [27] or choose nursing homes as their “homes” [49]. However, younger seniors, in good physical condition and capable of self-care, prefer home-based care rather than institutionalized care. Those who find it difficult to live alone intend to receive supportive care from society [31].
Most included studies also discussed faith or spiritual support. Many Asian seniors have a deep faith in religion which is a significant source of strength when facing life stressors [43]. However, although social support generally assists seniors positively, sometimes that support provides a negative experience, such as disrespect [32, 33, 43] or feeling of being a burden [43, 46, 47].
Discussions
Understanding how family and religious faith support (or unsupported) seniors might sensitize pharmacists to psychological and sociological factors that might be subsequently involved in medication taking and health-related behaviors. It is known that patient survival is improved when social and emotional factors are explicitly considered by healthcare providers [50]. Moreover, understanding social support would improve pharmacist communication, which previously noted as ineffective two-way communication between pharmacist and patient [51]. Since the nonadherence problems are located within the inefficient communication process or in the lack of rapport with patients [52], improving communication might improve patient adherence.
Assessing whether seniors have appropriate family support is the most important since family or relatives will assist seniors in adhering to and benefiting from treatment recommendations. Some studies indicated pharmacists should understand that family members are essential to patients’ medication [33, 48]. A study in Thailand also revealed that elderly individuals with a daughter as a caretaker were approximately eight times more likely to adhere to their antihypertensive treatment than patients with no caretaker [53].
However, there is an increasing trend of seniors living alone in Asia, such as Japan, South Korea, and Taiwan [54]. Nevertheless, living alone does not necessarily mean no family support because nonresident family members can still provide support [55]. For seniors living in households separate from family members, pharmacists might help these seniors maintain their independence. Pharmacists should be aware that seniors expect to be self-reliant and not to be a burden to anyone.
Religious or spiritual support might correspond with medication use and adherence. Pharmacists may encounter scenarios and circumstances where communication about faith becomes necessary, such as discussing chronic disease management in religious communities. Because believing in a higher power enables seniors to face difficult times with an optimistic and resilient attitude [37], pharmacists should not go against this faith. Instead, encouraging seniors to develop self-reflexivity through communication might promote better adherence.
Other things to be considered are that receiving and providing support is also crucial for seniors [37]. Being involved and active in any community, such as a church community [45], would make seniors feel useful as they can provide emotional support and friendship to others, share information and encouragement [32], and remain active as long as possible. A previous study even proved that providing social support for elders is more important than receiving it [12]. To address this need, there are usually ranges of communities a pharmacist can suggest to seniors, from neighborhood-based to hospital-based communities.
Pharmacists must understand taboos and other sensitive issues around seniors’ conditions. Discussing death with seniors might be considered taboo [45], but pharmacists involved in end-of-life and palliative care would eventually encounter this conversation with seniors. Pharmacists must also know that discussing seniors’ needs would be challenging as imposing needs and problems on others might also be considered inappropriate, as the included studies indicated [37, 41].
However, seniors’ perceptions and experiences regarding social support may vary across regions and circumstances. The included studies indicated that younger-old, male, or living with a family will have different needs or perspectives than older-old, female, or having no family. Tailoring the health education message to the needs of seniors would be more helpful. Patients take information and process it within their cognitive framework based on their interpretation of their own experiences [4]. Thus, even seniors would act differently and selectively based on their needs and circumstances.
Implication for pharmacy practice
Improving pharmacist communication with seniors is the central recommendation from this review. The authors suggest points that might be incorporated into a standard procedure of pharmacist communication with seniors, such as ensuring the availability and ability of social support as well as assessing faith and beliefs related to medicine or health behavior. Since it is common in Asian culture to greet and ask about the condition of somebody’s family and relatives, it might be easier for pharmacists to do this communication. It will give insight into how pharmacists may involve any support available for individual seniors. For example, for independent seniors, it might be appropriate to ensure that their medication self-management at home is correct and to encourage them to be active in the community; for more dependent seniors who live with family members, it might be appropriate to educate through their family; or for seniors who live without family, it might be appropriate to ensure the availability of nearby relatives or neighbors to take them to regular check-ups, and so on.
Strength and limitations
From the pharmacy perspective, this review gives insights into pharmacist communication approach to elderly patients. Nevertheless, this review had some limitations. First, as a qualitative synthesis, data retrieved were thrice removed, which means we interpreted the experiences and perceptions that the original researchers interpreted from the interpretation of the seniors themselves as study participants [56]. We were not in the place and context when the primary data were collected, but rather we discussed the data in a quite diverse expertise background of reviewers. Second, we only included articles in English; there might be other comprehensive studies from Asia using non-English languages. Third, the search strategy in this review was not directly associated with pharmacy or medicine, but our discussion attempts to link the available evidence about social support with pharmacy practice.
Conclusions
The present review affirmed the evidence from Asian seniors that they are more affected by family support and religious faith. Pharmacists should incorporate family and religious faith approaches in communication with seniors for an effective pharmaceutical service.
Availability of data and materials
All data for analysis in this review is in the public domain.
Abbreviations
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- ENTREQ:
-
Enhancing Transparency in Reporting the Synthesis of Qualitative Research
- CASP:
-
Critical Appraisal Skills Programme
References
United Nations Department of Economic and Social Affairs. World population ageing 2019. New York: United Nations; 2020.
Lampela P, Hartikainen S, Sulkava R, Huupponen R. Adverse drug effects in elderly people–a disparity between clinical examination and adverse effects self-reported by the patient. Eur J Clin Pharmacol. 2007;63(5):509–15.
Cárdenas-Valladolid J, Martín-Madrazo C, Salinero-Fort MA, Carrillode-Santa Pau E, Abánades-Herranz JC, de Burgos-Lunar C. Prevalence of adherence to treatment in homebound elderly people in primary health care. Drugs Aging. 2010;27(8):641–51.
Wertheimer AI, Smith MC. Pharmacy practice: social and behavioral aspects third edition. Williams & Wilkins; 1989.
Taylor K, Nettleton S, Harding G. Sociology for pharmacists second edition. 2003.
Al-Kandari YY, Crews DE. Social support and health among elderly Kuwaitis. J Biosoc Sci. 2014;46(4):518–30.
Bai Y, Bian F, Zhang L, Cao Y. The impact of social support on the health of the rural elderly in China. Int J Environ Res Public Health. 2020;17(6):2004.
Shumaker SA, Brownell A. Toward a theory of social support: closing conceptual gaps. J Soc Issues. 1984;40(4):11–36.
Tengku Mohd TAM, Yunus RM, Hairi F, Hairi NN, Choo WY. Social support and depression among community dwelling older adults in Asia: a systematic review. BMJ Open. 2019;9(7): e026667.
Dykstra P. Aging and social support. In: Ritzer G, editor. The blackwell encyclopedia of sociology. John Wiley & Sons Ltd; 2015.
Scheurer D, Choudhry N, Swanton KA, Matlin O, Shrank W. Association between different types of social support and medication adherence. Am J Manag Care. 2012;18(12):e461–7.
Zanjari N, Momtaz YA, Kamal SHM, Basakha M, Ahmadi S. The influence of providing and receiving social support on older adults’ well-being. Clin Pract Epidemiol Ment Heal. 2022;18(1): e174501792112241.
Herrera MS, Fernández MB. Stressful events in old age: who are most exposed and who are most likely to overcome them. Gerontol Geriatr Med. 2020;1(6):1–9.
Look KA, Stone JA. Medication management activities performed by informal caregivers of older adults. Res Social Adm Pharm. 2018;14(5):418–26.
Zheng S, Masuda T, Matsunaga M, Noguchi Y, Ohtsubo Y, Yamasue H, et al. Cultural differences in social support seeking: the mediating role of empathic concern. PLoS ONE. 2022;16(12): e0262001.
Hashimoto A, Ikels C. Filial piety in changing Asian societies. In: Johnson ML, editor. The Cambridge handbook of age and ageing. Cambridge: Cambridge University Press; 2005. p. 437–42.
Sari DN, Utami W, Zairina E. The influence of feeling lonely and received social support on medication adherence in elderly with hypertension. J Farm dan Ilmu Kefarmasian Indones. 2022;9(3):252–61.
Uchmanowicz B, Chudiak A, Uchmanowicz I, Rosińczuk J, Froelicher ES. Factors influencing adherence to treatment in older adults with hypertension. Clin Interv Aging. 2018;13:2425–41.
Voils CI, Steffens DC, Bosworth HB, Flint EP. Social support and locus of control as predictors of adherence to antidepressant medication in an elderly population. Am J Geriatr Psychiatry. 2005;13(2):157–65.
Ayonote UA, Akujuobi OM, Ogbonna AN. Family social support perceptions and medication adherence among elderly diabetics in a tertiary health institution in Lagos, Nigeria. Curre Res Diabetes Obes J. 2022;16(1): 555927.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, The PRISMA, et al. statement: an updated guideline for reporting systematic reviews. BMJ. 2020;2021:88.
Tong A, Flemming K, McInnes E, Oliver S, Craig J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med Res Methodol. 2012;12(1):181.
Butler A, Hall H, Copnell B. A guide to writing a qualitative systematic review protocol to enhance evidence-based practice in nursing and health care. Worldviews Evid-Based Nurs. 2016;13(3):241–9.
Critical Appraisal Skills Programme. CASP appraisal tool for qualitative research [Internet]. 2019 [cited 2021 Dec 20]. Available from: https://casp-uk.net/casp-tools-checklists/.
Walsh D, Downe S. Appraising the quality of research. Midwifery. 2006;22(2):108–19.
Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8(1):45.
Almazan JU, Cruz JP, Alamri MS, Albougami ASB, Alotaibi JSM, Santos AM. Coping strategies of older adults survivors following a disaster: disaster-related resilience to climate change adaptation. Ageing Int. 2019;44(2):141–53.
Amin I. Perceptions of successful aging among older adults in Bangladesh: an exploratory study. J Cross Cult Gerontol. 2017;32(2):191–207.
Kwan C, Tam HC. Ageing in place in disaster prone rural coastal communities: a case study of Tai O village in Hong Kong. Sustainability. 2021;13(9):4618.
Lao SSW, Le LLP, Wong KKY. Older residents’ perceptions of family involvement in residential care. Int J Qual Stud Health Well-being. 2019;14(1):1611298.
Liu JE, Tian JY, Yue P, Wang YL, Du XP, Chen SQ. Living experience and care needs of Chinese empty-nest elderly people in urban communities in Beijing, China: a qualitative study. Int J Nurs Sci. 2015;2(1):15–22.
Maria MAS, Bonanza AAC, Arcega PAS. Quality of support in the social networks of older Filipino church members: an exploratory study. Qual Ageing Older Adults. 2018;19(1):42–53.
Nazari S, Foroughan M, Shahboulaghi FM, Rassouli M, Sadeghmoghadam L, Farhadi A, et al. Perceived social support in Iranian older adults: a qualitative study. Educ Gerontol. 2016;42(6):443–52.
Pathike W, O’Brien A, Hunter S. Moving on from adversity: an understanding of resilience in rural Thai older people. Aging Ment Heal. 2019;23(3):311–8.
Rittirong J, Prasartkul P, Rindfuss RR. From whom do older persons prefer support? the case of rural Thailand. J Aging Stud. 2014;31:171–81.
Seah B, Espnes GA, Ang ENK, Lim JY, Kowitlawakul Y, Wang W. Supporting the mobilization of health assets among older community dwellers residing in senior-only households in Singapore: a qualitative study. BMC Geriatr. 2020;20(1):1–15.
Shiraz F, Hildon ZLJ, Vrijhoef HJM. Exploring the perceptions of the ageing experience in Singaporean older adults: a qualitative study. J Cross Cult Gerontol. 2020;35(4):389–408.
Tabari F, Khaghanizade M, Dehghan-Nayeri N, Najafi-Mehri S. Mental health and old age: a qualitative study in Iranian population. J Clin Diagnostic Res. 2017;11(11):5–8.
Badriah S, Sahar J. Family support in caring for older people with diabetes mellitus: a phenomenology study. Enferm Clin. 2018;28:245–9.
Tsuji K, Khan HTA. Exploring the relationship between social support and life satisfaction among rural elderly in Japan. Ageing Int. 2016;41(4):414–26.
Yoo S. The context of perceived and desired social support among Korean older adults. Psychol Heal Med. 2013;18(1):47–55.
Carandang RR, Asis E, Shibanuma A, Kiriya J, Murayama H, Jimba M. Unmet needs and coping mechanisms among community-dwelling senior citizens in the Philippines: a qualitative study. Int J Environ Res Public Health. 2019;16(19):3745.
Cassum LA, Cash K, Qidwai W, Vertejee S. Exploring the experiences of the older adults who are brought to live in shelter homes in Karachi, Pakistan: a qualitative study. BMC Geriatr. 2020;20(1):1–12.
Cheng Y, Xi J, Rosenberg MW, Gao S. Intergenerational differences in social support for the community-living elderly in Beijing, China. Heal Sci Reports. 2018;1(11): e96.
Chuang YH, Abbey JA, Yeh YC, Tseng IJ, Liu MF. As they see it: a qualitative study of how older residents in nursing homes perceive their care needs. Collegian. 2015;22(1):43–51.
Han E, Shiraz F, Haldane V, Koh JJK, Quek RYC, Ozdemir S, et al. Biopsychosocial experiences and coping strategies of elderly ESRD patients: a qualitative study to inform the development of more holistic and person-centred health services in Singapore. BMC Public Health. 2019;19(1):1107.
Harnirattisai T, Vuthiarpa S. The perception of independent living among Thai older adults. Ageing Int. 2020;45(2):181–90.
Kristianingrum ND, Wiarsih W, Astuti YN. Perceived family support among older persons in diabetes mellitus self-management. BMC Geriatr. 2018;18(Suppl 1):304.
Ghani NA, Noordin N, Zulkifli NI, Abdullah B, Ghazalli FSM. Social support for the elderly at Darul Hanan nursing home, Penang, Malaysia. Man India. 2016;96(12):5209–28.
Smith TB, Workman C, Andrews C, Barton B, Cook M, Layton R, et al. Effects of psychosocial support interventions on survival in inpatient and outpatient healthcare settings: a meta-analysis of 106 randomized controlled trials. PLoS Med. 2021;18(5): e1003595.
Keshishian F, Colodny N, Boone RT. Physician-patient and pharmacist-patient communication: geriatrics’ perceptions and opinions. Patient Educ Couns. 2008;71(2):265–84.
Weiss GL, Copelton DA. The sociology of health, healing, and illness. Routledge; 2020.
Woodham N, Taneepanichskul S, Somrongthong R, Auamkul N. Medication adherence and associated factors among elderly hypertension patients with uncontrolled blood pressure in rural area, Northeast Thailand. J Heal Res. 2018;32(6):449–58.
Yeung W-JJ, Cheung AK-L. Living alone: one-person households in Asia. Demogr Res. 2015;S15(40):1099–112.
Kendig HL, Hashimoto A, Coppard LC. World Health Organization. Family support for the elderly: the international experience. Oxford University Press; 1992.
Sandelowski M, Barroso J. Handbook for synthesizing qualitative research. Springer Publishing Company; 2006.
Acknowledgements
The authors would like to thank Faculty of Pharmacy Universitas Gadjah Mada for the license of QSR's NVivo 12 Pro software. The authors would like to thank Enago (www.enago.com) for the English language review.
Funding
This study was supported by Universitas Gadjah Mada.
Author information
Authors and Affiliations
Contributions
SS, CW, NNW, and RSP developed the concept and search strategy. NNW conducted the retrieval and data extraction. NNW and RSP did thematic synthesis. CW and NNW conducted critical appraisals. NNW drafted the manuscript. SS and P added the draft into the agreed final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
An ethics approval number was not required as this study did not include any confidential participant data and interventions.
Consent for publication
Not applicable.
Competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
The summary of quality assessment of the included studies.
Additional file 2.
ENTREQ Statement.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Widyakusuma, N.N., Suryawati, S., Wiedyaningsih, C. et al. Equipping pharmacists for delivering pharmaceutical care to seniors: a qualitative systematic review of Asian seniors’ social support. J of Pharm Policy and Pract 16, 75 (2023). https://doi.org/10.1186/s40545-023-00576-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40545-023-00576-7