
Abstract
Background
In many low- and middle-income countries, the 2019 novel coronavirus (COVID-19) has challenged efforts to ensure access to and availability of quality maternal, newborn, and child health (MCH) services and essential MCH commodities.
Objectives
This study evaluated the impact of COVID-19 pandemic on the availability of maternal and child health products and childhood vaccines at selected health facilities in Ethiopia.
Methods
We have prospectively assessed 28 maternal–child health products and 14 childhood vaccines and accessories, which are listed in the Ethiopian national essential medicines list. Data were collected from 5 hospitals located in the Jimma zone of Oromia regional state in the southwestern part of Ethiopia. We extracted data on drug availability, and order fill rates for these pharmaceutical products between May 2019 and August 2020.
Results
The overall mean availability of selected maternal and child health products was 43.2%. It was 52.9% (range 21.0–63.6%) prior COVID-19 and 42.6% (range 19–56.4) during COVID-19 time. The average monthly orders fill rates of hospitals for the selected products ranged from 39 to 79%. Before COVID-19 the average order fill rate was near 70% of total orders placed by the hospitals. However, immediately after the COVID-19 case notification in Ethiopia, the percentage of order filled correctly in items and quantities began decreasing.
Conclusion
This study illustrates that the availability of key essential medicines for maternal and child health in the study area was low. The overall stock-out situation of MCH products has worsened during COVID-19 compared to pre-COVID-19 pandemic. None of the surveyed MCH products met the ideal availability benchmark of 80% in the public hospitals. To allow governments to guarantee these products are constantly available and affordable, a variety of policy frameworks and choices addressing inevitable epidemics should exist.
Similar content being viewed by others


Background
In many low- and middle-income countries (LMICs), the novel coronavirus disease-2019 (COVID-19) has challenged efforts to ensure access to and availability of quality maternal and child health (MCH) services and essential MCH commodities [1, 2]. Maintaining MCH service and ensuring the availability of commodities at health facilities remains critical because, without them, women and children may suffer, and even die, from preventable causes. However, COVID-19 has worsened existing challenges in many LMICs [3, 4]. Since the first COVID-19 outbreak, LMICs' health supply chains have been forced to respond to new demands, such as changes in patient consumption dynamics, upstream supply shocks, and the requirement to guarantee that health care professionals have access to proper personal protective equipment [5, 6].
The disruptive effects of the COVID-19 pandemic and government response measures, such as lockdowns, may further negatively influence healthcare systems, with women and children among the most vulnerable to its consequences. Pregnant women and children under the age of five face the highest risk of death immediately before, during, and after birth [7, 8]. However, ensuring the availability of a limited set of high-impact, essential MCH services and commodities can mitigate these risks and improve MCH outcomes. In the context of COVID-19, ensuring consistent availability of these commodities at health facilities is critical because decreased antenatal care outpatient visits and primary care consultations for children have been reported [9, 10], which suggests that opportunities to administer care and treatment are more limited than ever. Lack of commodity stock may further discourage MCH care-seeking behavior; a full supply of essential MCH commodities is important.
According to the official data published by World Health Organization (WHO) and United Nations International Children’s Emergency Fund (UNICEF) more than 23 million children missed out on basic childhood vaccines through routine health services in 2020, which was the highest number since 2009 and 3.7 million more than in 2019 [11, 12]. Direct and indirect effects of the pandemic on MCH services could be devastating, and jeopardize the important gains made over the last several decades [12]. Similarly, the COVID-19 pandemic is expected to have profound effects on the healthcare systems of Ethiopia. The government of Ethiopia has concerns about diminished access to maternal health products and childhood vaccines [13, 14], but little evidence exists on service provision, utilization, or availability of those essential medicines. Understanding the impact of COVID-19 pandemic on the availability of key MCH medications is critical for effectively managing supply chain disruptions in the event of a future pandemic. Access to essential health services is critical to effective pandemic response. Therefore, this study aimed to assess the knock-on effect of COVID-19 on the availability of MCH products and vaccines in southwest Ethiopia.
Methods
Study setting and period
The study was conducted at hospitals found in Jimma Zone, Oromia regional state in Ethiopia (Fig. 1). The zone has 7 hospitals (one new and the rest have been providing services for at least more than 2 years). The current study was conducted at 5 selected hospitals found in the zone. Data on stock availability, order requested and issued were extracted from the health commodity management information system of the facilities. We included 8 months pre-pandemic (May 2019–December 2019) and eight months during pandemic (January 2020–August 2020) data.

Map of Ethiopia and study area
Study design
Institutional-based cross-sectional study was employed to assess the availability of life-saving MCH products and vaccines and key challenges. In addition to quantitative approach, the study adopted the qualitative case study design, which is used as an empirical inquiry that investigates a contemporary phenomenon in depth and within its real-life context to know how COVID-19 pandemic affected the availability and stock status of MCH products.
Selection of pharmaceutical products and measurement
According to the United Nations Population Fund (UNFPA), UNICEF, and WHO recommendations [15, 16], the commodities evaluated were among the priority medicines for mothers and children, which are used to treat primary causes of maternal death and as well as vaccine used for prevention of. The availability of MCH products and childhood vaccines was measured by using a selected supply chain management performance measuring matrix by function during the COVID-19 pandemic. This utilizes the selected indicators for each logistics activity. This assessment revealed the sum of stock levels available at the service delivery points (hospitals). Using the Logistics Management Information System (LMIS) tools one year data before the COVID-19 outbreak was compared with its status during COVID-19.
Data source and type
The study used health facility records, pharmacy professionals working as store managers in the selected health facilities, and physical observation as data sources. Observation, physical inventory, and review of facility records, as well as DAGU (software program for managing medications) and structured interviews with health-institution pharmacy professionals, were used to collect primary data. The data included stock status, availability of MCH pharmaceutical products commodities, childhood vaccines, and the availability of various LMIS formats.
Data collection
The investigators recruited five trained pharmacy professionals as data collectors. They received training that included the assessment’s purpose and data collection tool administration. The investigators worked closely with the data collectors and provided regular recommendations. The team visited the study facilities to check for the accuracy and completeness of the information collected.
Quantitative data were collected using a modified logistics indicator assessment tool (LIAT) developed by the USAID-Deliver Project [17] for the assessment of facility-based logistics indicators. This structured tool was used to collect data quantitatively from different source materials from health facilities stores and relevant units at the facility. And each finding was recorded for analysis.
Data processing and analysis
Data were checked for completeness and consistency and then entered into the Statistical package for social sciences (SPSS) version 25. Descriptive statistics were used to summarize the findings and the results were presented as frequency tables and graphs. The availability of individual medicines was calculated as the percentage of sampled medicine facilities where the medicine was found. Product availability was assessed based on the WHO’s availability index A product is available if available in the health facility providing a service on the day of the visit or during the specified period. The following ranges were used for describing availability: < 30%—very low; 30–49%—low; 50–80%—fairly high; > 80%—high [18, 19].
Ethical consideration
Before commencing data collection, ethical approval was obtained from the Institutional Review Board (IRB) of the Institute of Health, Jimma University in Ethiopia. Then, the selected hospitals were communicated with a formal letter from the health research and innovation office of Jimma University. The study was conducted in the selected health facilities after getting permission from the medical directors/managers of respective health facilities. Participants of the study were asked for written consent before participating in the study.
Results
Quantitative data
Availability of MCH products and vaccines
The stock status of MCH products and vaccines products at each hospital was measured; this included a review of stock availability for both the stock levels during COVID-19 (January 2020–August 2020) and stock levels for the 8 months before COVID-19 (May 2019–December 2019). It was calculated as:
The finding of the current study revealed that the overall mean availability of selected MCH products was 43.2%. It was 52.9% (range 21.0–63.6%, standard deviation = 13.4) before COVID-19 and 42.6% (range 19.0–56.4%, standard deviation = 9.8) during COVID-19 time. The outbreak created significant changes in the availability of MCH products in the hospitals.
The mean availability of antibiotics was fairly high before and during the outbreak of the COVID-19 pandemic. Methyldopa was fairly available before COVID-19 pandemic (56%) and its availability was decreased to 32% during the outbreak. The availability of dexamethasone 4 mg/1 ml Injection was significantly changed during COVID-19 (48%) as compared to prior the outbreak (76%). The overall mean availability of all products showed differences before and during the COVID-19 pandemic. None of the surveyed hospitals had any stocks of cefixime for the treatment of sexually transmitted diseases (Table 1).
Availability of childhood vaccines and accessories
The findings of the current study revealed that the overall availability of selected childhood vaccines and accessories was 62.3% (range 26–74%, standard deviation = 11.8) before COVID-19 pandemic. It was 54.7% (range 34–78.2%, standard deviation = 8.2) during COVID-19 pandemic. The outbreak created significant changes in the availability of childhood vaccines and accessories in the hospitals. Except for the safety box, the overall mean availability of childhood vaccines and their accessories showed differences before and during the COVID-19 pandemic (Table 2).
Overall orders fill rates
This indicator was used to measure the percentage of the difference between the amount ordered and the amount received for each pharmaceutical product in each month. This was calculated as:
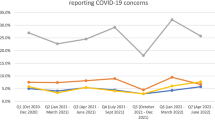
The average monthly orders fill rates of hospitals for the selected products range from 39 to 82%. Before COVID-19 the average order fill rate was near 70% of total orders placed by the hospitals. The highest (79%) order fill rate was recorded in August 2019. However, starting from the month of COVID-19 case notification, the percentage of selected medicines order(s) filled correctly in terms of items and quantities started decreasing. In March 2020, when the first COVID-19 case was reported in Ethiopia, there was a significant decrease in the order fill rate of the products at health facilities. In March 2020 only 60% of orders requested were resupplied. There was a sharp decrease in stock supply starting from March 2020 through August 2020 (Fig. 2).

The average monthly order fill rates of hospitals
Discussion
The availability of MCH medicines makes the difference between life and death and has the biggest impact on reducing maternal mortality [15]. Hence, priority attention to ensuring commodity security should be given in countries like Ethiopia where the maternal mortality ratio remains high. Unless access is ensured, the Sustainable Development Goals (SDG) target to reduce maternal mortality with no country having over 140 per 100,000 live births by 2030 will not be achieved [20].
In the current study, the availability of MCH medicines fell short of the 80% target set by WHO. The overall mean availability of selected MCH products was 43.2%. It was slightly higher than other similar surveys conducted in east African Countries, which showed the average availability in Tanzania (37.9%), Uganda (37.9%), and Zambia (38.6%) [21]. But, it was lower when compared with the same study from Kenya (46.6%) [21] and Myanmar 52.9% [22], The results from the studies confirm the poor availability of priority medicines for women and children in the LMICs.
Across the world, the pandemic affects the supply of essential medicines used for maternal and child health. For example, similar to the report from Nepal [23], in the study area, the pandemic has made it harder to get Misoprostol (16%). Similarly, in the previous studies, the average availability of dexamethasone injection was between 84.9% and 91.4% [24, 25] in the health facilities. However, its availability significantly decreased to 48% during the pandemic. This might be associated with the rise in demand for dexamethasone after some study finds the medication can be used to manage severe cases of COVID-19 [26, 27] and global problem in the supply of essential medicines.
Relative to other MCH products antibiotics were fairly available before and during the COVID-19 pandemic. However, similar to other previous studies [28, 29] the cefixime 400 mg, the antibiotic used for the treatment of sexually transmitted diseases was completely absent in selected health facilities. This might be due to the dependence on the previous guideline and also the intention to reserve the antibiotics for other infections caused by resistance pathogens.
Before COVID-19 pandemic, oxytocin (76%) and magnesium sulphate (66%) was fairly available. This was in line with a study from sub-Saharan Africa which also reported their average availability of 81%, and 54%, respectively [30]. However, the mean availability of the two medicines decreased during the COVID-19 pandemic. This was lower than the study report from Mali [31], where the availability of magnesium sulfate (73.7%) and oxytocin (99.5%) was reported from facilities. This might be due to differences in data collection time and level of health facilities. The study from Mali also included pre-COVID-19 time and assessed data from lower primary care hospitals.
In the current study, the availability of 14 childhood vaccines and accessories was assessed. The overall mean availability of selected childhood vaccines and accessories was 62.3%. This was similar to a study from Libya [32], which reported average availability of 60%. This is indicative of plummeting rates of basic vaccinations among the world’s children. Stock management concerns, vaccine quality issues, procurement delays, worldwide vaccine shortages, financing delays, and other unspecified challenges have been mentioned as reasons for stockouts in LMICs [33]
Moreover, the pandemic worsened the shortages of autodisable (AD) syringes. For example, the average availability of Syringe (A–D) 0.5 ml was 64% before COVID-19 pandemic and decreased to 52% during the pandemic. Such shortage was reported in most of LMICs [34]. In LMICs, nearly all vaccines are administered with a 0.5-mL AD syringe. This might be associated with the increase in the rollout of COVID-19 vaccines, which increases a massive syringe shortage due to high consumption. In general, the current study showed that the mean availability of childhood vaccines and their accessories was less than 70%. This is expected to impact the SDG of universal health coverage by 2030. Therefore, achieving the bold vision laid out in the global immunization agenda 2030 [35, 36], which aims to vaccinate 90% of children and adolescents worldwide, will be possible only with strong multilateral cooperation energized by political will.
Ethiopia already faced a chronic shortage of essential neonatal health drugs and commodities [37]. The COVID-19 pandemic could worsen the shortage by disrupting procurement and importation, and transportation of essential neonatal health commodities. One of the raised issues as a problem for the shortage of the products was the financial capacity to procure commodities. Particularly, in LMICs' capacity to procure essential neonatal health commodities are compromised by economic losses from the COVID-19 pandemic, countries restricting the export of medical supplies, as well as the shrinking global development assistance from different donors [38,39,40]. Moreover, transportation of essential commodities through global supply chains becomes a challenge due to the travel bans and restrictions imposed across borders [41]. This is a significant lesson learned from the COVID-19 pandemic, in which geographical diversification of vaccine production is required to fulfill local demands and increase immunization uptake, particularly in LMICs.
Limitation of the study
Despite the fact that the current study provided critical evidence on the impact of the COVID-19 pandemic on the availability of critical MCH medications and childhood vaccines, the qualitative aspects of the study were weak. One of its limitations was its small sample size which will not adequately describe the magnitude of the challenges in the supply management of life-saving MCH products and vaccines.
Conclusion
This study illustrates that the availability of key essential medicines for maternal and child health in the study area was low. The overall stock-out situation of MCH pharmaceutical products in the study area has worsened during COVID-19 compared to pre-COVID-19 time. None of the surveyed MCH products met the ideal availability benchmark of 80% in the public hospitals. The COVID-19 pandemic continues to have broad-reaching effects on MCH and seems to be affecting the availability of MCH services and commodities. To allow governments to guarantee these products are constantly available and affordable, a variety of policy frameworks and choices addressing inevitable epidemics should exist. Creative solutions in the supply chain are needed to offer new ways to tackle COVID-19-related challenges.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- COVID-19:
-
Corona virus disease-2019
- IRB:
-
Institutional review board
- LIAT:
-
Logistics Indicator Assessment Tool
- LMICs:
-
Low- and middle-income countries
- LMIS:
-
Logistics Management Information System
- MCH:
-
Maternal and Child Health
- SPSS:
-
Statistical Package for Social Sciences
- UNFPA:
-
United Nations Population Fund
- UNICEF:
-
United Nations Children’s Fund
- WHO:
-
World Health Organization
References
Balogun M, et al. Actions and adaptations implemented for maternal, newborn and child health service provision during the early phase of the COVID-19 pandemic in Lagos, Nigeria: qualitative study of health facility leaders. Ann Global Health. 2022; 88(1).
Ivankovich M, et al. Effects of COVID-19 on essential MNCHN/FP/RH care and the strategies and adaptations emerging in response.
Jnr MLK. National Response to COVID-19 Pandemic in Nigeria and South Africa: A comparative study of the impact on health inequality and health infrastructure on urban and rural residents.
Chauke HL. Fit for purpose? The strengths and weaknesses of Gauteng maternity services health care organisation/configuration in the context of reducing maternal deaths. 2021, University of the Free State.
Ullah F. COVID-19 Impact on Global Supply Chains and Environment-A Systematic Literature Review. 2021.
Riley T, et al. Estimates of the potential impact of the COVID-19 pandemic on sexual and reproductive health in low-and middle-income countries. Int Perspect Sex Reprod Health. 2020;46:73–6.
Lawn JE, et al. 4 million neonatal deaths: when? Where? Why? The Lancet. 2005;365(9462):891–900.
Ronsman C, Graham WJ. en representación del grupo de dirección de Lancet Maternal Survival, “Maternal Mortality: Who, When, Where, and Why? Maternal Survival”. The Lancet Maternal Survival Series, 2006: 13–23.
Hailemariam S, Agegnehu W, Derese M. Exploring COVID-19 related factors influencing antenatal care services uptake: a qualitative study among women in a rural community in Southwest Ethiopia. J Prim Care Community Health. 2021;12:2150132721996892.
Goyal M, et al. The effect of the COVID-19 pandemic on maternal health due to delay in seeking health care: experience from a tertiary center. Int J Gynecol Obstet. 2021;152(2):231–5.
Causey K, et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: a modelling study. The Lancet. 2021;398(10299):522–34.
Unicef, Averting a lost COVID generation: a six-point plan to respond, recover and reimagine a post-pandemic world for every child. 2020: UNICEF.
Desta AA, et al. Impacts of COVID-19 on essential health services in Tigray, Northern Ethiopia: a pre-post study. PLoS ONE. 2021;16(8): e0256330.
Assefa N, et al. Reported barriers to healthcare access and service disruptions caused by COVID-19 in Burkina Faso, Ethiopia, and Nigeria: a telephone survey. Am J Trop Med Hyg. 2021;105(2):323.
Jonathan H, Stoltenberg RHJ. UN commission on life-saving commodities for women and children. New York: United Nations; 2012.
Organization, W.H., Priority life-saving medicines for women and children 2012. 2012, World Health Organization.
Snow, J., Logistics indicators assessment tool (LIAT). 2008.
Organization, W.H., Measuring medicine prices, availability, affordability and price components. 2008, World Health Organization.
Organization WH. Technical definitions of shortages and Stockouts of medicines and vaccines. Geneva: World Health Organization; 2017.
Ethiopia, F.D.R., Ethiopia Demographic and Health Survey 2016. Addis Ababa Ethiopia, and Rockville. 2016, CSA ICF Maryland, USA.
Ooms GI, et al. Access to sexual and reproductive health commodities in East and Southern Africa: a cross-country comparison of availability, affordability and stock-outs in Kenya, Tanzania, Uganda and Zambia. BMC Public Health. 2020;20(1):1–14.
Myanmar Ministry of Health, U.N.P.F., 2015 Health facility assessment for reproductive health commodities and services. 2016, Department of Medical Research, Department of Public Health, Department of ….
Relief, D., Shortages of a Lifesaving Medication Threatened Mothers in Nepal. Direct Relief Is Sending 34,000 Doses. https://reliefweb.int/report/nepal/shortages-lifesaving-medication-threatened-mothers-nepal-direct-relief-sending-34000#:~:text=But%20the%20pandemic%20has%20also,t%20have%20misoprostol%20on%20hand., 2021.
Workineh Getahun, H.T., Edmealem Ejigu,Antenane Korra, Health Facility Assessment on Availability of the 13 Reproductive, Maternal, Newborn, and Child Health Commodities Prioritized by the UN Commission on Life-Saving Commodities for Women and Children. https://siapsprogram.org/publication/health-facility-assessment-on-availability-of-the-13-reproductive-maternal-newborn-and-child-health-commodities-prioritized-by-the-un-commission-on-life-saving-commodities-for-women-and-children/, 2016.
Damtew D, et al. Availability of lifesaving maternal and child health commodities and associated factors in public and private health facilities of Addis Ababa, Ethiopia. Health Serv Res Managerial Epidemiol. 2019;6:2333392819892350.
Dian Zhang, U.T., Demand for dexamethasone rises after study finds COVID-19 benefits, FDA data shows. https://www.usatoday.com/story/news/2020/07/02/coronavirus-drug-cheap-steroid-shortage-after-increased-demand/5355016002/, 2020.
Ed Silverman, S., Hospitals see shortages of a cheap steroid that one study says helps Covid-19 patients. https://www.statnews.com/pharmalot/2020/06/25/covid19-coronavirus-dexamethasone-shortages/, 2020.
Abrha S, et al. Availability and affordability of priority life-saving medicines for under-five children in health facilities of Tigray region, northern Ethiopia. BMC Pregnancy Childbirth. 2018;18(1):1–9.
Hailu AD, Mohammed SA. Availability, price, and affordability of WHO priority maternal and child health medicine in public health facilities of Dessie, north-East Ethiopia. BMC Med Inform Decis Mak. 2020;20(1):1–10.
Pronyk PM, et al. The UN Commission on Life Saving Commodities 3 years on: global progress update and results of a multicountry assessment. Lancet Glob Health. 2016;4(4):e276–86.
Program, U.G.H.S.C., Mali’s health supply chain delivers critical commodities for moms and babies. https://www.ghsupplychain.org/news/medicines-mothers-can-rely, 2021.
Organization, R.G.o.L.a.W.H., Critical Childhood Routine Vaccines Availability Assessment—Monthly Districts Health Situation Report. https://reliefweb.int/report/libya/critical-childhood-routine-vaccines-availability-assessment-monthly-districts-health, 2022.
Organization, W.H., 2018 assessment report of the Global Vaccine Action Plan: strategic advisory group of experts on immunization. 2018, World Health Organization.
Threatened, P.P.A.f., The syringe shortage, explained. https://www.path.org/articles/syringe-shortage-explained/, 2021.
O'Brien K, Lindstrand A, Nandy R. The Immunization Agenda 2030: a vision of global impact, reaching all, grounded in the realities of a changing world. Available at SSRN 3830709, 2021.
Organization, W.H., Immunization as an essential health service: guiding principles for immunization activities during the COVID-19 pandemic and other times of severe disruption, 1 November 2020. 2020.
Institute, E.P.H., Services Availability and Readiness Assessment (SARA) 2018 Final Report. https://www.ephi.gov.et/images/pictures/download_2011/Ethiopia-Service-Availability-and-Rediness-Assessment-SARA-report-2018.pdf. 2018.
Miguel E, Mobarak AM. The economics of the COVID-19 pandemic in poor countries. Annu Rev Econ. 2021;14:253.
Shumba C, et al. Reorienting nurturing care for early childhood development during the COVID-19 pandemic in Kenya: a review. Int J Environ Res Public Health. 2020;17(19):7028.
Rosa-Mangeret F, et al. 2.5 million annual deaths—are neonates in low-and middle-income countries too small to be seen? A bottom-up overview on neonatal Morbi-mortality. Trop Med Infect Dis. 2022;7(5):64.
Sharma A, Gupta P, Jha R. COVID-19: impact on health supply chain and lessons to be learnt. J Health Manag. 2020;22(2):248–61.
Acknowledgements
We would like to extend our appreciation and thank our data collectors, and study participants. We also extend our sincere gratitude to health care professionals, and managers at service delivery points for providing us with necessary data/information, and for their kind cooperation, and assistance throughout the data collection process. Additionally, we would like to express our heartfelt gratitude to the Jimma Emergency Operation Center for financially supporting this research. Last but not least, our acknowledgment extends to the Institute of the health of Jimma University for supporting us in the ethical approval process and the official communication of our respective offices and health facilities.
Funding
This work was supported by the Jimma Emergency Operation Center (JEOC), Jimma University, Ethiopia.
Author information
Authors and Affiliations
Contributions
TSM, DA, and ZM designed the study. TSM, ZM, DA, and TK drafted the first version of the manuscript. TSM, ZM, DA, MG, TK, and FG discussed the analytic strategy. TSM, ZM, and MG did the data curation and performed the analysis. All authors reviewed the final paper and made creative and substantial contributions, approved the final version, and consented to publication. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study received approval from the Institutional Review Board of the Institute of Health, Jimma University in Ethiopia.
Consent for publication
Not required.
Competing interests
None declared.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Melaku, T., Assefa, D., Gashe, F. et al. Impact of COVID-19 pandemic on the availability of maternal and child health products and childhood vaccines. J of Pharm Policy and Pract 16, 35 (2023). https://doi.org/10.1186/s40545-023-00541-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40545-023-00541-4