
Abstract
Background
For more than a decade, direct oral anticoagulants (DOACs) have been approved in clinical practice for multiple indications such as stroke prevention in non-valvular atrial fibrillation treatment of deep vein thrombosis and pulmonary embolism. This study aimed to explore the nature and contributory factors related to medication errors associated with DOACs in hospital settings.
Methods
Analysis of error reports using data from (a) Saudi Food and Drug Authority pharmacovigilance database and (b) local incidents reporting system from two tertiary care hospitals were included. Errors reported between January 2010 to December 2020 were also included. Statistical analyses were performed using IBM (SPSS) Statistics Version 24.0 software.
Results
A total of 199 medication error incidents were included. The mean (range) age of affected patients was 63.5 (19–96) years. The mean reported duration of treatment when incidents happened was 90 days, with a very wide range from one day to 12 months. Prescribing error was the most common error type representing 81.4% of all errors. Apixaban was the most frequent drug associated with error reporting with 134 (67.3%) incidents, followed by rivaroxaban (18.6%) and dabigatran (14.1%). The majority of the patients (n = 188, 94.5%) showed comorbidities in addition to the conditions related to DOACs. Polypharmacy, an indication of treatment and duration of therapy were amongst the important contributory factors associated with errors.
Conclusions
This observational study demonstrates the nature of DOAC related medication errors in clinical practice. Developing risk prevention and reduction strategies using the expertise of clinical pharmacists are imperative in promoting patient safety associated with DOAC use.
Similar content being viewed by others

Introduction
Direct oral anticoagulants (DOACs), or the non-vitamin K antagonist oral anticoagulants (NOACs) includes dabigatran, rivaroxaban, edoxaban, apixaban and betrixaban. In Saudi Arabia, clinicians follow recommendations of a recently published clinical pathway for DOACs by the Saudi Society of Clinical Pharmacy [1]. The Saudi Food and Drug Authority approved rivaroxaban in 2011, apixaban in 2014 edoxaban in 2018 and dabigatran in 2009 for stroke prevention in NVAF, and treatment or prevention of venous thromboembolism (VTE) [2]. Rivaroxaban also has other indications such as indefinite anticoagulation, stable coronary arterial disease or peripheral arterial disease, VTE prophylaxis in acutely ill medical patients and in total hip or knee arthroplasty. Apixaban and dabigatran also have approval for VTE prophylaxis in total hip or knee arthroplasty [1].
DOACs have gained popularity in clinical practice because they have fixed dosing and do not need frequent monitoring, have fewer drug and food interactions and offers less risk of bleeding compared to warfarin [3,4,5,6,7,8,9]. These characteristics have made them an attractive choice for the management of conditions requiring anticoagulation therapy [10]. They are labelled as high-risk medications due to the risk of causing significant patient harm if used inappropriately [11].
DOACs can cause bleeding if overdosed or exacerbate thromboembolic events if a therapeutic failure occurs, and it could further increase mortality [12]. Factors that could lead to inappropriate prescribing of DOACs could range from inaccurate dosing due to renal dysfunction, non-consideration of patients' body weight or age or concomitant polypharmacy [13]. Currently, there is a lack of research about medication errors associated with DOACs in Saudi Arabia [14]. Identifying DOACs most commonly involved with errors, type of errors, contributory factors, and patient characteristics that are linked with frequent occurrence of errors can enable identifying appropriate strategies to improve patient safety. This study aims to explore the types of medication errors and contributory factors associated with DOACs in hospital settings in Saudi Arabia using national and hospital local datasets. Specific objectives were to (a) identify the DOACs most commonly involved in the medication errors and (b) identify the stages in the medication journey where the errors occurred in order to understand the contributory factors.
Methods
Study design
The design of this study was a retrospective observational using incidents reporting databases from two healthcare institutions and the pharmacovigilance database of a national regulatory body, the Food and Drug Administration (FDA) in Saudi Arabia.
The hospital-based data were retrieved from the electronic medical record system for all errors reported from the year of such medications became available in Saudi Arabia, January 2010, to December 2020. They included patients’ demographic data (age, gender, weight, and height), drug name and its indication, comorbidities, dosing regimen and duration of treatment, type of medication error (prescribing, administration, and dispensing) and renal function test results.
The Pharmacovigilance Electronic Reporting Service in the Saudi FDA is an online spontaneous reporting system for reporting side effects, medication errors, and any defect in the quality of pharmaceutical preparations. It also allows sending and submitting communications to report a drug shortage by health practitioners, pharmacies, health institutions, companies, and community members. It receives voluntary reports of safety concerns from health practitioners and patients.
All reports associated with DOACs errors in adult population generated from 2010 to 2020 were included in the study for the final analysis. Reports without drug names or not related to DOACs were excluded. The local collaborators at the main centres in Saudi Arabia communicated with the respective departments to obtain the required medication error reports for the said period. The data were retrieved electronically from the institutions’ reporting systems using drug names as the search terms. The extracted data were cleaned for any duplications, and all variables were compiled in an excel file.
Statistical analyses were performed using IBM (SPSS) Statistics Version 24.0* software. Quantitative data (age in years) were described using median, range and Interquartile range after data distribution exploration normality using Kolmogorov–Smirnov (K–S test) and Shapiro tests. Descriptive analysis was undertaken to describe numbers and proportions. For all statistical tests, a significance level was determined below 5%. Monte Carlo exact test was used for comparing the categorical variables instead of the Chi-square test because the assumptions of conducting a Chi-square test were violated [> 20% of the cells had an expected count less than 5].
This study was reviewed and approved by a research ethics committee University of Birmingham (ERN_20-0551). Approvals were also obtained from King Abdullah International Medical Research Center (KAIMRC) at Ministry of National Guard, Saudi Arabia (SP/212/R), and from KFMMC (AFHER-IRB-2020-015), as well as from Saudi Food and Drug Authority (SFDA).
Results
After reviewing the reported safety incidents of medication errors in all involved Saudi Arabia institutions, the database revealed that a total of 199 medication error incidents were found related to direct oral anticoagulants (DOAC); 109 errors were reported from the hospitals and 90 errors reported from Saudi Food and Drugs Authority (SFDA) from January 2010 to December 2020. Table 1 illustrates patients’ characteristics with the reported incidents.
Medication errors related to specific DOAC and indication
Medication errors were reported for three DOAC drugs: the higher incidents were reported with apixaban (67%) followed by rivaroxaban (19%) and dabigatran (14%) as shown in Fig. 1. Most of the indications for DOACs were found to be related to atrial fibrillation at (56.8%), followed by deep vein thrombosis at (27.6%), pulmonary embolism at (10.1%), cerebral venous thrombosis at (1.0%), and others at (4.5%) as shown in Fig. 2.

Proportions of direct-acting anticoagulants (DOACs) associated with medical errors

Different indications of direct oral anticoagulants (DOACs) in the medication error reports
Errors as per the stages of medication journey
The most commonly identified subtype of prescribing errors related to prescribing incorrect dose accounting for 44 incidents (22.1%) followed by 33 (16.6%) incidents of duplicate prescribing, 30 (15.5%) incidents of dispensing incorrect quantity, prescribing incorrect frequency with (n = 29, 14.6%), 25 (12.6%) incidents of dispensing to the wrong patient and 11 (5.5%) incidents of prescribing an incorrect duration.
Figure 3 shows incidents of medication errors related to the stages of the medication use process.

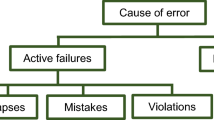
Different types of medication errors reported with direct oral anticoagulants (DOACs)
The other sub-types represented minimal incidents (less than 5%), such as delayed preparation, improper or lack of documentation. Figure 4 summarizes the percentages for all the identified types of medication errors.

Sub-types of medication errors associated with direct oral anticoagulants (DOACs)
Errors classified as per specific DOAC and their indications
Whilst analysing the indication of the DOAC drugs among the collected reports, it was found that apixaban was mainly prescribed for atrial fibrillation (n = 73, 54.5%). It was also prescribed to the cases of deep vein thrombosis (n = 34, 25.4%), pulmonary embolism (n = 17, 12.7%), cerebral venous thrombosis (n = 2, 1.5%), and others such as hip or knee replacement surgery representing about 6%. Likewise, rivaroxaban was mainly prescribed for atrial fibrillation (n = 27, 73%), deep vein thrombosis (n = 8, 21.6%), and pulmonary embolism (n = 2, 5.4%). Dabigatran was prescribed equally for atrial fibrillation and deep vein thrombosis (n = 13, 46.4%, each), and also it was prescribed to single cases of pulmonary embolism and others, as shown in Table 2.
Errors classified as per specific DOAC and stages of medication journey
Whilst analysing the phases and types of medication errors associated with the three DOAC drugs, it was found that 103 (76.8%) of apixaban incidents occurred during the prescribing phase, 20 (15.0%) during the dispensing phase, 7 (5.2%) occurred during the administration phase, 3 (about 2.3%) occurred during the storage process, and only one incidents (about 0.7%) reported during the monitoring phase. For dabigatran, almost all the errors (n = 27, 96.7%) were within the prescribing phase, with only one reported incident during the dispensing phase. For rivaroxaban, the majority of errors (n = 32, 86.5%) occurred during the prescribing phase, with 3 (8.1%) incidents during the monitoring phase, and two incidents (5.4%) during the administration phase. There was a statistically significant difference in the percentage of medication errors among the three reported drugs during the prescribing phase (p = 0.001), while the other phases did not exert statistical significance, as shown in Table 3.
Discussion
DOACs are considered high-risk medication and have the potential to cause harm when used erroneously [15]. This study explored the reported medication errors related to the three approved DOAC medications in the Kingdom of Saudi Arabia for the first time. Previous studies provide evidence of improper utilization associated with DOACs and potentially inappropriate prescribing leading to adverse events [15, 16]. In a retrospective study, medication errors were identified as a common root cause in 40% of anticoagulation-related adverse events [12].
In Saudi hospitals, several quality measures have been put in place at institutional levels, including restricting prescribing DOAC to certain specialities, e.g., (cardiology, haematology, internist, and through clinical pharmacy involvement). In addition, institutional guidelines have been developed based on different international guidelines, including American Heart Association and Chest guidelines. Furthermore, both the pharmacy department and the pharmacoeconomic centre monitor Medication Utilization Evaluation (MUE) of all DOAC listed in the hospital formulary. It is important that prescribers and healthcare professionals responsible for dispensing and administration of drugs are aware of the up-to-date guidelines and embrace additional safety practices when dealing with DOACs.
Among the three DOACs drugs, apixaban was the most frequently prescribed anticoagulant and hence associated with a higher number of errors. In our study, we were limited by the type of data that could be retrieved from the institutional safety reporting system, and this limited further investigation and follow-up for the seriousness of the reported medication errors. Previous studies have found that anticoagulants are often associated with underdosing and overdosing [17]. In one study, approximately a third of the patients received inappropriate dose including lower doses at (18%) and higher doses at (15%) [18].
This study also showed that DOACs-associated medication errors were most often reported during the prescribing phase. Most of these errors were typical and included wrong dose, medication, frequency, and duration. These results are in line with prior studies that found most reported medication errors occur in the prescribing stage. Raccah et al. found that prescribing errors with DOACs occur in nearly a third of the patients with AF [19]. Dreijer et al. observed that errors with anticoagulant therapy were most often seen during prescribing and administration phases [20]. In our study, the least type of errors reported were administration error, e.g., apixaban 5.2% and rivaroxaban (5.4%, which usually occurs during the administration of drugs by nurses in hospitals or by patients at home. In France, a prospective nationwide cohort study in primary care reported that 39% of the patients received at least one inappropriate DOAC prescription, mostly were inappropriate underdosing [21]. Another cross‐sectional study of oral anticoagulant use in patients with AF demonstrated underdosing in 13.1% of prescriptions, and unfortunately, 39.4% of their patients had not been prescribed an indicated DOACs [22].
This observational study is limited due to its retrospective design and the small number of variables available to undertake detailed evaluation of the nature and causes of errors. The sample size was limited despite including both national and local datasets suggesting the extent of under-reporting of medication errors. Furthermore, the consequences, including clinical, humanistic and cost-related outcomes of these errors, could not be estimated from the available data. Pharmacists and nurses are the main healthcare professionals reporting these prescribing errors in the institution, yet we do not have clear data on the reporting proportion.
Conclusion
Further development and standardization of risk prevention measures is crucial to minimize the harm from medication errors with DOACs. Most of the reported DOACs-associated medication errors relate to prescribing stage, characteristically in the form of inappropriate dose, the inappropriate agent chosen, frequency, and duration. It is important to reinforce the education of healthcare professionals on the safe and effective use of DOACs, and the importance of medication error reporting. Pharmacists can play an integral role in minimizing medication error incidents through the development of safe and effective pharmacotherapeutic plans at the initial assessment and prescribing phase. Safety issues can also be identified and addressed during medicines reviews, medicines reconciliation and patient counselling. Healthcare professionals’ awareness and the need to have clear prescribing guidelines are imperative for safe DOACs prescribing.
Availability of data and materials
All data generated or analysed during this study are included in this published article.
Abbreviations
- UK:
-
United Kingdom
- DOACs:
-
Direct oral anticoagulants; NOACs: Non-vitamin k antagonist oral anticoagulants
- VTE:
-
Venous thromboembolism
- PE:
-
Pulmonary embolism
- DVT:
-
Deep vein thrombosis
- NVAF:
-
Non-valvular atrial fibrillation
References
Saudi Society of Clinical Pharmacy. Direct Oral Anticoagulants (DOACs) Clinical Pathway. 2020; https://www.cchi.gov.sa/AboutCCHI/CCHIprograms/Documents/Direct%20Oral%20Anticoagulants%20(DOACs)%20.pdf. Accessed 16 Sept 2021.
Saudi Food and Drug Authority. Human Drug List. https://old.sfda.gov.sa/EN/DRUG/SEARCH/Pages/default.aspx?PageIndex=644. Accessed 16 Sept 2021.
Almarshad F, Alaklabi A, Bakhsh E, Pathan A, Almegren M. Use of direct oral anticoagulants in daily practice. Am J Blood Res. 2018;8(4):57–72.
Alshammari TMAS, Mahmoud MA, Alhawassi TM, Aljadhey HS. Signals of bleeding among direct-acting oral anticoagulant users compared to those among warfarin users: analyses of the post-marketing FDA Adverse Event Reporting System (FAERS) database, 2010–2015. Ther Clin Risk Manag. 2018;14:803–9.
Hersi AS, Alhebaishi YS, Hamoui O, et al. Practical perspectives on the use of non-vitamin K antagonist oral anticoagulants for stroke prevention in patients with nonvalvular atrial fibrillation: a view from the Middle East and North Africa. J Saudi Heart Assoc. 2018;30(2):122–39.
Mayet AY, Alsaqer AI, Alhammad AM, Al-Omar HA. Rivaroxaban prescribing in a Saudi tertiary care teaching hospital. Saudi Pharm J. 2018;26(6):775–9.
Al Yami MS, Alzahrani MY, Alshehri AM, et al. Real-World Effectiveness and Safety of Apixaban versus Warfarin in patients with acute venous thromboembolism: experience of a large tertiary hospital in Saudi Arabia. Int J Gen Med. 2021;14:4031–7.
Andreica I, Grissinger M. Oral anticoagulants: a review of common errors and risk reduction strategies. Pa Patient Saf Advis. 2015;12(2):54–61.
Valentine D, Gaunt M, Grissinger M. Identifying patient harm from direct oral anticoagulants. Pa Patient Saf Advis. 2018;15:2.
Loo SY, Dell’Aniello S, Huiart L, Renoux C. Trends in the prescription of novel oral anticoagulants in UK primary care. Br J Clin Pharmacol. 2017;83(9):2096–106.
National Health Service (Midlands Partnerships). List of high-risk medicines. https://www.mpft.nhs.uk/application/files/5915/5159/0841/High-Risk-Drugs-List.pdf. Accessed 14 Sept 2021.
Piazza G, Nguyen TN, Cios D, et al. Anticoagulation-associated adverse drug events. Am J Med. 2011;124(12):1136–42.
Haque H, Alrowily A, Jalal Z, et al. Direct oral anticoagulant-related medication incidents and pharmacists’ interventions in hospital in-patients: evaluation using reason’s accident causation theory. Int J Clin Pharm. 2021.
Thomas B, Paudyal V, MacLure K, et al. Medication errors in hospitals in the Middle East: a systematic review of prevalence, nature, severity and contributory factors. Eur J Clin Pharmacol. 2019;75(9):1269–82.
Henriksen JN, Nielsen LP, Hellebek A, Poulsen BK. Medication errors involving anticoagulants: data from the Danish patient safety database. Pharmacol Res Perspect. 2017;5(3):e00307.
Barr D, Epps QJ. Direct oral anticoagulants: a review of common medication errors. J Thromb Thrombolysis. 2019;47(1):146–54.
Steinberg BA, Shrader P, Thomas L, et al. Off-label dosing of non-vitamin K antagonist oral anticoagulants and adverse outcomes: the ORBIT-AF II Registry. J Am Coll Cardiol. 2016;68(24):2597–604.
Ruiz Ortiz M, Muniz J, Rana Miguez P, et al. Inappropriate doses of direct oral anticoagulants in real-world clinical practice: prevalence and associated factors. A subanalysis of the FANTASIIA Registry. Europace. 2018;20(10):1577–83.
Raccah P, Bruria H, Erlichman Y, Pollak A, Matok I, Muszkat M. Prescribing errors with direct oral anticoagulants and their impact on the risk of bleeding in patients with atrial fibrillation. J Cardiovasc Pharmacol Therap. 2021;1:10742484211019656.
Dreijer AR, Diepstraten J, Bukkems VE, et al. Anticoagulant medication errors in hospitals and primary care: a cross-sectional study. Int J Qual Health Care. 2019;31(5):346–52.
Ferrat E, Fabre J, Galletout P, et al. Inappropriate direct oral anticoagulant prescriptions in patients with non-valvular atrial fibrillation: cross-sectional analysis of the French CACAO cohort study in primary care. Br J Gen Pract. 2021;71(703):e134–9.
Angel Y, Zeltser D, Berliner S, et al. Hospitalization as an opportunity to correct errors in anticoagulant treatment in patients with atrial fibrillation. Br J Clin Pharmacol. 2019;85(12):2838–47.
Acknowledgements
None.
Funding
AA was sponsored by the Saudi Ministry of Education for the PhD programme. No other funding was received for the conduct of this study.
Author information
Authors and Affiliations
Contributions
This study relates to AA’s PhD research. VP, ZJ supervised AA for his PhD. All authors co-designed the study. Search was performed by AA and verified by NO and MHA. The data analysis and interpretation was conducted by AA and reviewed by VP, ZJ and MA. The first manuscript draft was written by AA. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by University of Birmingham Ethics Committee (Ref: ERN_20-0551) and the departmental Approval for Undertaking a Research Study at KFMMC as (Approval no. IRB-F-005 and the departmental Approval for Undertaking a Research Study at King Abdulaziz Medical City in Riyadh as (Approval No. IRB SP20/212/R).
Competing interests
The authors declare that they have no competing interests.
Additional information
Handling editor: Zaheer Babar, University of Huddersfield, UK.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Alrowily, A., Jalal, Z., Abutaleb, M.H. et al. Medication errors associated with direct-acting oral anticoagulants: analysis of data from national pharmacovigilance and local incidents reporting databases. J of Pharm Policy and Pract 14, 81 (2021). https://doi.org/10.1186/s40545-021-00369-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40545-021-00369-w