
Abstract
Background
Methamphetamine use can be associated with involvement with correctional services and incarceration. Traditionally, treatments for methamphetamine use have been delivered in-person – however, lockdowns initiated during the COVID-19 pandemic significantly reduced access to such in-person support in prisons. Therefore, in May 2020 a digital cognitive-behavioral therapy (CBT) program for substance use disorders - 'Breaking Free from Substance Abuse' - was made available across prisons in Ohio in order to meet this treatment gap. This represents the first time this digital CBT intervention has been made widely available to incarcerated people residing in prisons or jails in the United States (US). This was a within-subjects study using data from 2187 Ohio prison residents who engaged with this digital CBT program to address their methamphetamine use.
Results
Participants reported multiple psychosocial risk factors, including moderate to severe substance dependence, depression and anxiety; interpersonal conflict; aggressive behavior; paranoia; and difficulties with work, education and accommodation. Significant reductions in substance dependence, depression/anxiety and biopsychosocial impairment, and improvements in quality of life, were identified in the sample. Risk factors were associated with less positive outcomes, specifically interpersonal conflict and poor mental health. Completion of specific components of the program were associated with more positive outcomes – a dose response was also identified.
Conclusions
Digital CBT can be delivered in secure US correctional settings and may help to fill unmet needs for in-person treatment. Specifically, this digital CBT program may support incarcerated individuals to address methamphetamine use, with outcomes being associated with psychosocial risk factors and program engagement.
Similar content being viewed by others


Background
During the COVID-19 pandemic in-person substance use disorder (SUD) treatment was limited, with many services moving to digital and telehealth delivery (Monaghesh & Hajizadeh 2020). However, delivering technology-mediated treatment in secure correctional settings is challenging – despite this, there have been examples of correctional services working innovatively to meet the needs of their populations during the pandemic. This study therefore reports data from prison residents across Ohio who accessed digital cognitive behavioral therapy (CBT) for SUD during the pandemic. This study focuses on methamphetamine-involved residents given the links between use of the drug and involvement with correctional services.
The links between methamphetamine use and involvement in correctional services
Prevalence of methamphetamine use amongst people in the United States (US) in 2019 was 1.2 million for past-month use (Center for Behavioral Health Statistics and Quality 2020). Methamphetamine use is associated with an unstable lifestyle and psychosocial risk factors that are linked to involvement in correctional services (Cumming et al. 2020), including mental health disorders such as psychosis (Chiang et al. 2019), homelessness (Jones et al. 2020), financial difficulties (McKetin et al. 2020) and interpersonal conflict (Maltman et al. 2020). These factors may increase likelihood of both acquisitive (Goldsmid & Willis 2016) and violent crimes (Liu et al. 2017).
Mental health and other psychosocial difficulties (e.g. homelessness), SUD and offending interact in multiple ways (Hamilton 2014). The “self-medication” hypothesis (Robinson et al. 2011) suggests that some people use substances as a means of coping with their mental health difficulties, or conversely, substance use may directly cause, or exacerbate, pre-existing mental health difficulties (e.g. Boden & Fergusson 2011). Alternatively there may be some other common factor that increases vulnerability to mental health and substance use issues, such as chronic stress (Brady & Sinha 2005) or certain personality traits (Kotov et al. 2010). Substance use and mental health difficulties may start in late childhood and early adolescence (Deas & Brown 2006), often alongside significant childhood adversity (Johnson et al. 2006), with these difficulties then contributing to an increased risk of offending in adulthood (Wiesner et al. 2005).
Psychosocial risk factors are found in models describing criminogenic risk factors, one of the most influential being the ‘risk-need-responsivity’ model (RNR: Andrews et al. 2006). Risk factors identified within the model include family and/or marital issues, difficulties at school or work, leisure or recreation issues, and substance abuse, in addition to anti-social behaviours, cognitions, personality patterns, and associates. These risk factors provide targets for assessment and intervention in populations involved in correctional services – higher-risk offenders may experience greater reductions in recidivism from RNR-informed interventions compared to lower-risk offenders (Bonta & Andrews 2007).
Treatment for methamphetamine use and the impact of the COVID-19 pandemic
Methamphetamine-involved offenders have unique treatment needs – use of the drug is often associated with cognitive impairments (Potvin et al. 2018) and risk-taking and erratic behaviors (Homer et al. 2008), and people who use the drug often experience complex mental health issues including psychosis (Cumming et al. 2020). In contrast with other substances associated with involvement with correctional services, e.g. opioids (Chen et al. 2022) and alcohol (Akbar et al. 2018), there are no accepted pharmacological treatments for methamphetamine use (Siefried et al. 2020). The only existing treatments are psychosocial and behavioral – a systematic review demonstrated CBT and contingency management to be effective in reducing use of the drug (AshaRani et al. 2020), and therapeutic communities have also been demonstrated to confer therapeutic benefits in correctional (Joe et al. 2010) and community settings (Šefránek & Miovský 2017). However, there may be barriers to accessing treatment for methamphetamine use, including financial costs and lack of available places in programs (Cumming et al. 2016).
A significant barrier to accessing both community and correctional in-person SUD services since March 2020 has been the COVID-19 pandemic. Krebs and colleagues (2021) examined the impact of the pandemic on corrections agencies across Ohio – 75% of respondents reported restrictions that impacted rehabilitative programming, including SUD treatment. Massachusetts (Donelan et al. 2021) and New York State (Wang et al. 2021) implemented telehealth approaches to provide medications for opioid use disorders during the pandemic. Such technology-mediated approaches have been explored for the treatment of methamphetamine use in community settings (Rubenis et al. 2021) – this review not find significant reductions in methamphetamines use and suggested this could be due to app design features such as whether content was personalized, and participant characteristics such as personality style.
The potential of digital cognitive behavioral therapy in treating methamphetamine use
Digital technology can also be used to deliver CBT for SUD (e.g. Carroll et al. 2009; Kay-Lambkin et al. 2009), although these programs have largely been delivered in community settings due to the security challenges that exist in prisons and jails. The only digital CBT intervention for SUD that has been delivered in secure settings is ‘Breaking Free from Substance Abuse’, which has been available in UK prisons since 2015 (Davies et al. 2017; Elison et al. 2015). The program addresses dependence to multiple substances and also has demonstrated efficacy in community treatment services (e.g. Elison, Jones, et al. 2017; Elison, Ward, et al. 2017), for people using alcohol (Ward et al. 2019), cannabis (Elison-Davies, Wardell, et al. 2021) and opiates (Elison-Davies, Märtens, et al. 2021). The program has demonstrated user acceptability (e.g. Dugdale et al. 2017; Elison et al. 2015) and characteristics of individuals accessing the program via UK treatment services have also been reported (e.g. Elison, Jones, et al. 2017; Elison-Davies, Hayhurst, et al. 2021).
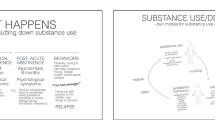
The program is modular and targets the psychological and lifestyle factors that underlie SUDs. When an individual first uses it they complete a baseline assessment, which includes the ‘Recovery Progression Measure’ (RPM: Elison et al. 2016) – the RPM measures levels of functioning in six biopsychosocial domains (see Fig. 1). The program uses data provided by the individual when they complete the RPM to populate a visual depiction of a theoretical CBT framework, the ‘Lifestyle Balance Model’ (LBM: Davies et al. 2015), which shows them the extent to which they may be experiencing impairments in the six domains of functioning measured by the RPM and represented in the LBM. The program achieves this by color coding each of the six components of the LBM – red domains represent significant impairment, amber moderate impairment, and green low/no impairment. The LBM is based on the five-factor model used in CBT (Williams & Garland 2002) and incorporates principles contained in the RNR model, in terms of focusing on the interplay between an individual’s cognitions, emotions, behaviors and lifestyle factors (Bonta & Andrews 2007).

The lifestyle balance model
Within the program are 12 evidence-based ‘behavioral change techniques’ (BCTs: Dugdale et al. 2016; Michie et al. 2013) that are effective in reducing substance use and biopsychosocial impairment – these 12 BCTs are located within the six components of the LBM. Each component of the LBM contains two BCTs – a psychoeducational ‘Information Strategy’ and a skills-building interactive ‘Action Strategy’. In order to complete a component of the LBM, an individual has to complete both the Information and Action Strategy associated with that component. Table 1 provides a full description of the BCTs contained in the program.
The program provides tailoring advice and recommends that users focus on first completing the components of the program that will allow them to address the areas of functioning where they are experiencing the most impairment, i.e. the areas of the LBM that are colored red – research indicates people follow this tailoring advice (Elison, Jones, et al. 2017). A ‘dose response’ has also been demonstrated, which suggests the more components of the program someone completes, the better their outcomes (Elison-Davies, Wardell, et al. 2021). Significant reductions in substance dependence, depression and anxiety, and biopsychosocial impairment, and improvements in quality of life, have been demonstrated for individuals who engage with the program in UK community settings (Elison et al. 2014; Elison, Ward, et al. 2017) and prisons (Davies et al. 2017; Elison et al. 2015).
Delivery of Breaking Free from Substance Abuse across Ohio Department of Rehabilitation and Correction
Since May 2020 Breaking Free from Substance Abuse has been available via secure tablets to prison residents across Ohio Department of Rehabilitation and Correction (ODRC). ODRC have had access to secure devices for some time – these devices were originally introduced to deliver educational content. Following rigorous security checks, Breaking Free from Substance Abuse was added as additional content to the devices at the start of the COVID-19 pandemic when in-person rehabilitative programs became unavailable. The program was rolled-out across all 28 adult facilities in a phased manner between May and November 2020. During this period, the developers of the program trained over 100 staff across ODRC so they could support residents using the it.
Aims
Delivery of the program across ODRC has allowed, for the first time, data to be collected from incarcerated individuals in the US engaging with this digital CBT for SUD. This study reports data from methamphetamine users given the high rates of psychosocial risk factors experienced by this population, the significant links between methamphetamine use and incarceration (Cumming et al. 2020) and the lack of pharmacological treatments for use of the drug (Siefried et al. 2020). To date, all published data from this digital CBT program has come from individuals engaging with it via UK treatment services (e.g. Elison-Davies, Hayhurst, et al. 2021), where methamphetamine is not a commonly used drug – a recent government report from 2020 to 2021 showed that only 505 members of the UK treatment population reported methamphetamine use (Office for Health Improvement and Disparities 2021). Therefore, this study also provides the first opportunity to report data from people engaging with the program for methamphetamine use.
This study uses a within-subjects design to examine changes over time on a number of measures collected at baseline and post-engagement. These data are used to examine: i) baseline psychosocial risk factors experienced by Ohio prison residents, ii) changes in their scores on measures of substance dependence, mental health, quality of life and biopsychosocial impairment when engaging with the program and iii) whether baseline psychosocial risk factors are associated with these changes. Additionally, iv) patterns of engagement with components of the program, and the extent to which program engagement is associated with changes in scores on the measures used, is also reported.
Methods
Design
Quantitative within-subjects, non-randomized observational study to examine associations between psychosocial risk factors, and engagement with a digital CBT program for SUD, with changes in scores on a range of measures, for prison residents who used the program to address their methamphetamine use during the COVID-19 pandemic.
Participants
Two thousand one hundred and eighty-seven ODRC residents who engaged with digital CBT to address their methamphetamine use between May 2020 and September 2021.
Procedure
Approval to analyze data provided by participants was granted by the ODRC Human Subjects Research Review Committee on May 3rd 2021. Residents who had been referred to prison SUD services were offered the digital CBT program whilst in-person services were unavailable due to COVID-19 restrictions. The program was made available via secure tablet computers – participants could sign-in to the tablet using their own unique login credentials to access the program, which was available via a link on the tablet landing page. Before participants could activate an account on the program they had to agree to a ‘Privacy and Cookies Policy’ and ‘End User License Agreement’. After account activation all participants were required to complete a baseline assessment containing several standardized measures:
-
a)
Severity of Dependence Scale (SDS: Gossop et al. 1997): 5-item scale measuring severity of substance dependence (e.g., cravings and substance-related cognitions). Internal reliability: α = .81–.90; test-retest reliability ICC = .89.
-
b)
Patient Health Questionnaire-4 (PHQ-4: Kroenke et al. 2009): 4-item scale measuring severity of depression and anxiety. Threshold scores on the PHQ are 0–3 no depression/anxiety, 3–5 ‘mild’, 6–8 ‘moderate’ and 9–12 ‘severe’. Internal reliability, α = .81.
-
c)
Five items (1, 2, 17, 18, 20) from the World Health Organization Quality of Life measure (WHOQoL-BREF: Skevington et al. 2004). Items selected were generic enough to measure general quality of life as opposed to specific aspects of quality of life. Internal reliability of these five items, α = .84.
-
d)
Recovery Progression Measure (RPM: Elison et al. 2016; Elison, Dugdale, et al. 2017): 36-item scale measuring functioning in the six domains of biopsychosocial functioning represented by the components of the LBM (see Fig. 1). Within each of the six RPM domains there are five dichotomous ‘yes/no’ items measuring presence or absence of specific biopsychosocial difficulties within that domain, and an 11-point Likert ‘impact scale’ assessing level of severity of impairment in that domain. Internal consistency, α = .89; test-retest reliability, ICC = .73.
-
e)
In addition to the standardized measures the baseline assessment also contained the following:
-
Demographic items: age, gender, and ethnicity.
-
Questions about what substances each participant was experiencing difficulties with – this information was also used to determine whether participants were poly-substance users.
The program’s backend database also automatically captured program engagement data: i) whether participants completed a follow-up assessment, and ii) which BCTs they had completed.
After baseline assessment completion, participants were provided with access to the program and engaged with it in a self-directed manner. Each participant’s account was available to them for 12-months and they could choose to engage with the program for as long as they wanted to during this period. The program prompts users to complete mandatory ‘Progress Check’ assessments every two weeks – people can also choose to complete Progress Check assessments more frequently. Data from the Progress Checks allow an individual to monitor their progress as they work through the program via a personalized dashboard.
Data analysis
The majority or variables reasonably approximated a non-normal distribution (skewness > 1, kurtosis > 2, Shapiro-Wilks < .05). Kruskall-Wallis tests were used to compare baseline assessment measure scores of i) participants who had completed a Progress Check and ii) those that had not completed a Progress Check to ascertain whether differences between these groups might explain why some participants completed a Progress Check assessment and some did not. For participants that did complete a Progress Check assessment, comparisons of scores on the assessment measures included from baseline to most recent Progress Check data were conducted using repeated-measure Mann-Whitney U tests and Cohen’s effect sizes. Whilst controlling for the confounding effects of baseline scores on outcomes on the assessment measures included, linear regressions were used to examine associations between psychosocial risk factors reported at baseline and outcomes scores obtained from most recent Progress Check assessment – this was done in order to ascertain whether baseline psychosocial risk factors might predict outcomes. Associations between whether or not each of the six components in the program had been completed and outcomes scores obtained from most recent Progress Check were also examined using linear regressions – this was done to ascertain whether completion of specific components of the program might predict outcomes. Finally, linear regressions were also used to examine associations between the number of components completed and outcomes on each of the assessment measures included, in order to determine whether there may be a ‘dosage effect’. Due to the number of comparisons in the analyses, a more conservative significance level of p = .01 was adopted.
Results
Sociodemographic characteristics
The largest age group was 25–34 years (896, 41%), followed by 35–44 years (766, 35%), 45–54 years (236, 11%), 18–24 years (223, 10%), 55–64 years (48, 2%), with the smallest age group being 65 years and over (6, 0.4%) – 12 (0.6%) participants did not provide their age. There were approximately twice as many male as female participants – 1416 (65%) reported identifying as male and 734 (33.5%) reported identifying as female. A total of 23 (1%) participants identified as belonging to a different gender group and 14 participants (0.5%) did not provide their gender. The largest ethnic group was White Americans (1854, 85%), followed by those having mixed heritage (121, 5.5%), Black or African Americans (86, 4%), Hispanic or Latino Americans (56, 2.6%), American Indian or Alaskan Natives (24, 1%), Asian Americans (7, 0.3%), with the smallest ethnic group being Native Hawaiian and other Pacific Islanders (3, 0.1%). A total of 36 (1.5%) participants did not provide their ethnicity.
Psychosocial risk factors
A total of 1427 (65%) participants reported engaging with the program to address their methamphetamine use only, 695 (32%) to address their use of methamphetamine plus one other substance, and 65 (3%) to address their use of methamphetamine plus two other substances. 1511 (69%) participants reported moderate to severe substance dependence (SDS total score ≥ 4) and 1259 (58%) participants reported moderate to severe depression/anxiety (PHQ-4 total score ≥ 6). Participants reported a number of risk factors measured by the RPM including difficult close relationships (1358, 62%), interpersonal conflict (1040, 48%), risk taking behaviors (1176, 54%), aggression (1137, 52%) and paranoid thoughts (989, 45%). Lifestyle difficulties were also reported including poor health (989, 45%), problems with work and education (625, 29%), unstable accommodation (1062, 49%) and financial difficulties (1127, 52%).
Comparison of baseline and Progress check assessment data
Of the 2187 participants who completed a baseline assessment, 1150 (53%) completed a Progress Check assessment – of those that did complete a Progress Check assessment, the mean number of assessments completed was four. The mean number of days between baseline assessment and most recent Progress Check assessment was 77.32 days (SD 96.20) or 11.05 weeks. No baseline differences were found between those participants who did complete a Progress Check assessment and those that did not (see Table 2).
For those participants that did complete a Progress Check, significant changes were found in scores across all measures (see Table 3), including reductions in methamphetamine dependence (SDS), depression/anxiety (PHQ), and biopsychosocial impairment (RPM), and improvements in quality of life (WHOQoL-BREF) (all p < .001). Effect size calculations demonstrated small effects for reductions in substance dependence (SDS: d = .45) and depression/anxiety (PHQ-4: d = 0.49), and improvements in quality of life (WHOQoL-BREF: d = 0.47), and a medium effect for reductions in biopsychosocial impairment (RPM: d = 0.54).
Associations between psychosocial risk factors and outcomes
Whilst controlling for baseline scores, a number of psychosocial risk factors appeared to predict scores at most recent Progress Check assessment (see Table 4). Results of the linear regressions conducted indicated that there was a collective significant effect between each of the risk factors included in the analysis on scores at most recent Progress Check: substance dependence (SDS: F (12,1136) = 18.700, p < .001, R2 = 0.165), depression/anxiety (PHQ-4: F(12,1137) = 24.721, p <,001, R2 = 0.207), quality of life (WHOQoL-BREF: F(12,1137) = 12.233, p < .001, R2 = 0.114) and biopsychosocial impairment (RPM: F(12,1137) = 12.537, p < .001, R2 = 0.117).
Individual risk factors appeared to be significant predictors of scores at most recent Progress Check. Conflict with others was significantly positively associated with depression/anxiety scores (PHQ-4: t = 2.409, p = .016) and problems with work or education was significantly negatively associated with quality of life scores (WHOQoL-BREF: t = − 2.416, p < .001). Additionally, baseline depression/anxiety was significantly negatively associated with quality of life scores (WHOQoL-BREF: t = − 6.195, p < .001) and significantly positively associated with biopsychosocial impairment scores (RPM: t = 5.996, p < .001).
Associations between program engagement and outcomes
Program engagement was also examined, including the number of components completed (out of a possible maximum of six), and which individual ‘Information Strategies’ and ‘Action Strategies’ (the 12 BCTs in the program) were completed. In order to complete a component of the program, an individual has to complete both the Information Strategy and corresponding Action Strategy contained within a component. The mean number of components completed by participants who provided Progress Check assessment data was 2.44 (SD 2.63), and 0.17 (SD 0.73) for those who did not provide Progress Check data. Table 5 demonstrates the numbers of both Progress Check assessment completers and non-completers who completed each of the 12 individual BCTs included in the six components of the program (the six Information Strategies and the six Action Strategies).
Whilst controlling for baseline scores, completion of the six components in the program appeared to predict scores at most recent Progress Check assessment (see Table 6). Results of the linear regressions conducted indicated that there was a collective significant effect between completion of program components on each of the scores at most recent Progress Check: substance dependence (SDS: F(7,1141) = 37.361, p < .001, R2 = 0.432), depression/anxiety (PHQ-4: F(7,1142) = 61.187, p <,001, R2 = 0.273), quality of life (WHOQoL-BREF: F(7,1142) = 59.729, p < .001, R2 = 0.268) and biopsychosocial impairment (RPM: F(7,1142) = 66.206, p < .001, R2 = 0.289) (see Table 6).
Completion of individual program components appeared to significantly predict some scores at most recent Progress Check. Completion of the Difficult Situation component was significantly negatively associated with biopsychosocial impairment scores (RPM: t = − 2.693, p = .007). Completion of the Unhelpful Behaviors component was significantly negatively associated with substance dependence (SDS: t = − 1.998, p = .046) depression/anxiety (PHQ-4: t = − 2.119, p = .034) and biopsychosocial impairment scores (RPM: t = − 3.244, p = .001). Completion of the Lifestyle component was significantly negatively associated with depression/anxiety (PHQ-4: t = − 2.659, p = .008) and biopsychosocial impairment scores (RPM: t = − 3.201, p = .001), and significantly positively associated with quality of life scores (WHOQoL-BREF: t = 2.934, p = .003).
A dose response was also identified, with the total number of program components completed being significantly negatively associated with substance dependence (SDS: F(2,1146) = 130,063, p < .001, R2 = 0.185), depression/anxiety (PHQ-4: F(2,1147) = 202.043, p <,001, R2 = 0.261) and biopsychosocial impairment scores at most recent Progress Check (RPM: F(2,1147) = 207.762, p < .001, R2 = 0.266), and positively associated with quality of life scores (WHOQoL-BREF: F(2,1147) = 205.271, p < .001, R2 = 0.0.264).
Discussion
This study reports data from 2187 methamphetamine-involved Ohio prison residents who engaged with a digital CBT program for SUD, ‘Breaking Free from Substance Abuse’, during the COVID-19 pandemic. Although there were twice as many male as female participants, females were over-represented in relation to Ohio’s prison population – there are only two women’s facilities in the state compared to 23 men’s facilities. This might demonstrate that women with SUD may be more receptive to digital CBT programs and deserves further investigation.
Participants reported a range of psychosocial risk factors that are common amongst methamphetamine uses, including interpersonal conflict (Dadhe & Bettman 2019; Maltman et al. 2020), mental health difficulties including paranoia (Dadhe & Bettman 2019; McKetin et al. 2019), impulsive and aggressive behaviors (Lanesman et al. 2019) and unstable accommodation and homelessness (Jones et al. 2020; Moxley et al. 2020). These difficulties have also been identified in the literature as criminogenic risk factors (Andrews et al. 2006) and are commonly experienced by incarcerated individuals who use methamphetamine (Semple et al. 2008).
Half of participants completed both a baseline assessment and a Progress Check assessment – significant reductions were found in scores for severity of substance dependence, depression/anxiety and biopsychosocial functioning impairment, and a significant increase in quality of life was demonstrated. Effect sizes for changes in substance dependence severity, depression/anxiety, and quality of life were small, and the effect size for changes in biopsychosocial functioning impairment was medium. Studies of other CBT interventions for methamphetamine use (AshaRani et al. 2020; Lee & Rawson 2008), and previous studies of this digital CBT program with UK prison populations (Davies et al. 2017; Elison et al. 2015), have obtained similar findings.
Psychosocial risk factors reported were significantly associated with most recent Progress Check assessment scores. Interpersonal conflict was significantly associated with poorer mental health and quality of life outcomes, and more severe depression/anxiety was significantly associated with poorer quality of life and biopsychosocial functioning outcomes. Research has demonstrated that such psychosocial risk factors may predict treatment outcomes in methamphetamine users, for example, interpersonal/relationship instability (Brecht & Herbeck 2014) and mental health difficulties (McKetin et al. 2018).
Participants who completed a Progress Check assessment completed more of the BCTs and components in the program that those that did not complete a Progress Check. For both Progress Check completers and non-completers, the Action and Information Strategies completed by the most participants were those in the Difficult Situations component of the program, and strategies completed by the least participants were those in the Unhelpful Behaviors component of the program. The Difficult Situations component supports individuals to develop skills to avoid and cope with difficult or risky situations – having these skills is particularly important in a prison environment where there may be multiple risks. However, the Unhelpful Behaviors component supports individuals to plan positive activities for each day of the week – the constraints of the prison environment could prevent incarcerated people from being able to identify activities that they can feasibly enact.
Completion of some components within the program was significantly associated with scores at most recent Progress Check. Completion of the Difficult Situations component was significantly associated with better biopsychosocial functioning scores, and completion of the Unhelpful Behaviors component was significantly associated with lower substance dependence, and better mental health and biopsychosocial functioning scores. Completion of the Lifestyle component was significantly associated with better mental health, biopsychosocial functioning and quality of life scores. These findings indicate that interventions for methamphetamine use should incorporate self-efficacy and coping skills development components (Moos 2007), in addition to clinical approaches to support emotional regulation (Kang et al. 2019) and positive lifestyle changes (Juel et al. 2017). The dose response identified in previous studies of this specific digital CBT program (Elison, Jones, et al. 2017; Elison-Davies, Wardell, et al. 2021), and other digital CBT for SUD studies (Mattila et al. 2016), was replicated in this study.
Findings suggest that greater clinical complexity at baseline might mean some individuals may benefit from support to enhance their level of engagement with the components of the program, in order to ensure they can experience optimal clinical benefits. When this digital CBT program is delivered alongside practitioner support, this can enhance retention and improve outcomes (Elison et al. 2014; Elison, Ward, et al. 2017). The literature demonstrates that individuals with SUD may be at risk of dropping out of treatment if they are not appropriately supported (Şimşek et al. 2019). Additionally, the literature around digital CBT for depression and anxiety demonstrates greater adherence and better outcomes when such programs are delivered alongside practitioner support (Andersson et al. 2019). Similar findings have been obtained for digital CBT for alcohol use disorder (Sundström et al. 2016), although there are gaps in the literature around whether practitioner guided or unguided digital CBT is most appropriate for other kinds of substance use disorders (Boumparis et al. 2019).
Although this study demonstrates that digital technologies can enhance rehabilitative programming, traditional in-person delivery may still be preferred by prison residents and staff. Introduction of such technologies can sometimes be perceived by staff as being disruptive as they may not feel they have the capacity to become familiar with new technologies (Davies et al. 2017). There may also be concerns around the security implications of providing digital technologies in secure settings – there have been examples of incarcerated people using digital technologies for nefarious means. However, work can be done to ensure rehabilitative technologies undergo thorough security checks before they are introduced into correctional settings, as was the case during the introduction of Breaking Free from Substance Use across ODRC.
As digital rehabilitative programming becomes more common, many of the benefits people experience from in-person support might be lost – however, digital programs need not eradicate the role of staff in program delivery. Many digital CBT programs are designed to be delivered as self-directed interventions and also ‘computer-assisted therapies’, with users being supported to engage with program content by staff. Additionally, digital programs are not necessarily designed to replace in-person support but augment it, especially during times when in-person support may be limited.
Had Breaking Free from Substance Use been introduced across ODRC before the pandemic it is not known whether the same amount of engagement would have been seen. However, the interactive nature of digital programs may be appealing to people in prisons and jails who may be bored or may have difficulties with concentration – work completed by the authors years before the COVID-19 pandemic indicated that even in non-pandemic times this treatment modality can be well received by incarcerated individuals (Davies et al. 2017; Elison et al. 2015). And regardless, it looks likely that health service delivery, and rehabilitation programming delivery, has been changed for the long-term as a result of the heavy reliance on digital technology during the COVID-19 pandemic.
Limitations
Limitations include that participants were self-selecting and a comparison group was not included given this study was an exploratory observational study, not a randomized controlled trial (RCT). Only half of participants completed a Progress Check assessment – the reasons for this could not be determined from data available. Attrition rates in digital intervention studies have been identified as a problem (Eysenbach 2005), with a recent review finding that even in highly controlled RCTs, the average attrition rate is 48% (Torous et al. 2020) – attrition in studies with SUD populations can also be high (Radtke et al. 2017). Additionally, it is difficult to determine whether changes in assessment scores were due to the clinical impact of the program or because some participants had higher levels of motivation and readiness to change. Therefore, determining effectiveness of the program for methamphetamine users via a RCT is an appropriate next step – a RCT could also build in longitudinal follow-up to explore how people fare when they return back to the community from prison.
Conclusions
This study reports data from US prison residents engaging with a digital CBT program for SUD. This study identified high rates of psychosocial risk factors commonly associated with methamphetamine use, and that these risk factors were associated with biopsychosocial changes experienced by people engaging with this program. Despite the clinical complexity of the group, they experienced significant reductions in substance dependence, depression/anxiety, and biopsychosocial impairment, and significant improvements in quality of life. Program engagement was associated with these changes and a dose response was identified, indicating that some prison residents might benefit from support when engaging with digital programs such as Breaking Free from Substance Abuse.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available for data privacy and security reasons. However, data can be made available upon request to the Corresponding Author for specific studies that have been reviewed and approved by a Research Ethics Board/Committee.
Abbreviations
- BCT:
-
behavioral change technique
- CBT:
-
cognitive behavioral therapy
- ODRC:
-
Ohio Department of Rehabilitation and Corrections
- PHQ-4:
-
Patient Health Questionnaire-4
- RPM:
-
Recovery Progression Measure
- SDS:
-
Severity of Dependence Scale
- SUD:
-
substance use disorder
- UK:
-
United Kingdom
- US:
-
United States
- WHOQoL-BREF:
-
World Health Organization Quality of Life Scale
References
Akbar, M., Egli, M., Cho, Y.-E., Song, B.-J., & Noronha, A. (2018). Medications for alcohol use disorders: An overview. Pharmacology & Therapeutics, 185, 64–85. https://doi.org/10.1016/j.pharmthera.2017.11.007.
Andersson, G., Titov, N., Dear, B. F., Rozental, A., & Carlbring, P. (2019). Internet-delivered psychological treatments: From innovation to implementation. World Psychiatry, 18(1), 20–28. https://doi.org/10.1002/wps.20610.
Andrews, D. A., Bonta, J., & Wormith, J. S. (2006). The recent past and near future of risk and/or need assessment. Crime and Delinquency, 52(1), 7.
AshaRani, P. V., Hombali, A., Seow, E., Ong, W. J., Tan, J. H., & Subramaniam, M. (2020). Non-pharmacological interventions for methamphetamine use disorder: A systematic review. Drug and Alcohol Dependence, 212, 108060.
Boden, J. M., & Fergusson, D. M. (2011). Alcohol and depression. Addiction, 106(5), 906–914.
Bonta, J., & Andrews, D. (2007). Risk-need-responsivity model for offender assessment and rehabilitation. Rehabilitation, 6, 1–22.
Boumparis, N., Schulte, M. H. J., & Riper, H. (2019). Digital mental health for alcohol and substance use disorders. Current treatment options in psychiatry, 6(4), 352–366. https://doi.org/10.1007/s40501-019-00190-y.
Brady, K. T., & Sinha, R. (2005). Co-occurring mental and substance use disorders: The neurobiological effects of chronic stress. American Journal of Psychiatry, 162(8), 1483–1493. https://doi.org/10.1176/appi.ajp.162.8.1483.
Brecht, M.-L., & Herbeck, D. (2014). Time to relapse following treatment for methamphetamine use: A long-term perspective on patterns and predictors. Drug and Alcohol Dependence, 139, 18–25. https://doi.org/10.1016/j.drugalcdep.2014.02.702.
Carroll, K., Ball, S., Martino, S., Nich, C., Babuscio, T., & Rounsaville, B. (2009). Enduring effects of a computer-assisted training program for cognitive behavioral therapy: A 6-month follow-up of CBT4CBT. Drug and Alcohol Dependence, 100(1), 178–181.
Chen, Q., Sterner, G., Segel, J., & Feng, Z. (2022). Trends in opioid-related crime incidents and comparison with opioid overdose outcomes in the United States. International Journal of Drug Policy, 101, 103555. https://doi.org/10.1016/j.drugpo.2021.103555.
Chiang, M., Lombardi, D., Du, J., Makrum, U., Sitthichai, R., Harrington, A., … Fan, X. (2019). Methamphetamine-associated psychosis: Clinical presentation, biological basis, and treatment options. Human Psychopharmacology: Clinical and Experimental, 34(5), e2710.
Cumming, C., Kinner, S. A., McKetin, R., Li, I., & Preen, D. (2020). Methamphetamine use, health and criminal justice system outcomes: A systematic review. Drug and Alcohol Review, 39(5), 505–518. https://doi.org/10.1111/dar.13062.
Cumming, C., Troeung, L., Young, J. T., Kelty, E., & Preen, D. B. (2016). Barriers to accessing methamphetamine treatment: A systematic review and meta-analysis. Drug and Alcohol Dependence, 168, 263–273.
Davies, G., Elison, S., Ward, J., & Laudet, A. (2015). The role of lifestyle in perpetuating substance dependence: A new explanatory model, the lifestyle balance model. Substance Abuse Treatment, Prevention, and Policy, 10(2), e1–e18.
Davies, G., Ward, J., Elison, S., Weston, S., Dugdale, S., & Weekes, J. (2017). Implementation and evaluation of the breaking free online and pillars of recovery treatment and recovery programmes for substance-involved offenders: Reflections from the north-west prisons ‘gateways’ pathfinder. Advancing Corrections, 3, 95–113.
Deas, D., & Brown, E. S. (2006). Adolescent substance abuse and psychiatric comorbidities. Journal of Clinical Psychiatry, 67(7), e02. https://doi.org/10.4088/jcp.0706e02.
Donelan, C. J., Hayes, E., Potee, R. A., Schwartz, L., & Evans, E. A. (2021). COVID-19 and treating incarcerated populations for opioid use disorder. Journal of Substance Abuse Treatment, 124, 108216.
Dugdale, S., Elison, S., Davies, G., Ward, J., & Dalton, M. (2017). A qualitative study investigating the continued adoption of breaking free online across a national substance misuse organisation: Theoretical conceptualisation of staff perceptions. The Journal of Behavioral Health Services and Research, 44(1), 89–101. https://doi.org/10.1007/s11414-016-9512-0.
Dugdale, S., Ward, J., Hernen, J., Elison, S., Davies, G., & Donkor, D. (2016). Using the behavior change technique taxonomy v1 to conceptualize the clinical content of breaking free online: A computer-assisted therapy program for substance use disorders. Substance Abuse Treatment, Prevention, and Policy, 11(1), 26.
Elison, S., Davies, G., & Ward, J. (2016). Initial development and psychometric properties of a new measure of substance misuse ‘recovery progression’: The recovery progression measure (RPM). Substance Use and Misuse, 51(9), 1195–1206.
Elison, S., Dugdale, S., Ward, J., & Davies, G. (2017). The ‘rapid recovery progression measure’ (rapid-RPM) a brief assessment of psychosocial functioning change during problematic substance use recovery progression. Substance Use and Misuse, 52(9), 1160–1169.
Elison, S., Jones, A., Ward, J., Dugdale, S., & Davies, G. (2017). Examining effectiveness of tailorable computer-assisted therapy programmes for substance misuse: Programme usage and clinical outcomes data from breaking free online. Addictive Behaviors, 74, 140–147.
Elison, S., Ward, J., Davies, G., Lidbetter, N., Dagley, M., & Hulme, D. (2014). An outcomes study of eTherapy for dual diagnosis using breaking free online. Advances In Dual Diagnosis, 7(2), 52–62.
Elison, S., Ward, J., Williams, C., Espie, C., Davies, G., Dugdale, S., … Smith, K. (2017). Feasibility of a UK community-based, eTherapy mental health service in greater Manchester: Repeated-measures and between-groups study of ‘living life to the full interactive’, ‘Sleepio’ and ‘breaking free online’ at ‘self help services’. BMJ Open, 7(7), 1–10.
Elison, S., Weston, S., Davies, G., Dugdale, S., & Ward, J. (2015). Findings from mixed-methods feasibility and effectiveness evaluations of the “breaking free online” treatment and recovery programme for substance misuse in prisons. Drugs: Education, Prevention and Policy, 23(2), 1–10.
Elison-Davies, S., Hayhurst, K., Jones, A., Welch, Z., Davies, G., & Ward, J. (2021). Associations between participant characteristics, digital intervention engagement and recovery outcomes for participants accessing ‘breaking free online’ at ‘change grow live’. Journal of Substance Use, 26(5), 497–504. https://doi.org/10.1080/14659891.2020.1851407.
Elison-Davies, S., Märtens, K., Yau, C., Davies, G., & Ward, J. (2021). Associations between baseline participant demographic, clinical and complexity characteristics on treatment outcomes for individuals accessing ‘breaking free online’, a computer-assisted therapy program for opioid use disorders. American Journal of Drug and Alcohol Abuse, 47(3), 360–372.
Goldsmid, S., & Willis, M. (2016). Methamphetamine use and acquisitive crime: Evidence of a relationship. Trends and Issues in Crime and Criminal Justice, 516, 1–14.
Gossop, M., Best, D., Marsden, J., & Strang, J. (1997). Test–retest reliability of the severity of dependence scale. Addiction, 92(3), 353–353.
Hamilton, I. (2014). The 10 most important debates surrounding dual diagnosis. Advances In Dual Diagnosis, 7(3), 118–128. https://doi.org/10.1108/ADD-05-2014-0013.
Homer, B. D., Solomon, T. M., Moeller, R. W., Mascia, A., DeRaleau, L., & Halkitis, P. N. (2008). Methamphetamine abuse and impairment of social functioning: A review of the underlying neurophysiological causes and behavioral implications. Psychological Bulletin, 134(2), 301.
Joe, G. W., Rowan-Szal, G. A., Greener, J. M., Simpson, D. D., & Vance, J. (2010). Male methamphetamine-user inmates in prison treatment: During-treatment outcomes. Journal of Substance Abuse Treatment, 38(2), 141–152. https://doi.org/10.1016/j.jsat.2009.08.002.
Johnson, R. J., Ross, M. W., Taylor, W. C., Williams, M. L., Carvajal, R. I., & Peters, R. J. (2006). Prevalence of childhood sexual abuse among incarcerated males in county jail. Child Abuse and Neglect, 30(1), 75–86. https://doi.org/10.1016/j.chiabu.2005.08.013.
Jones, A. A., Gicas, K. M., Seyedin, S., Willi, T. S., Leonova, O., Vila-Rodriguez, F., … Vertinsky, A. T. (2020). Associations of substance use, psychosis, and mortality among people living in precarious housing or homelessness: A longitudinal, community-based study in Vancouver, Canada. PLoS medicine, 17(7), e1003172.
Juel, A., Kristiansen, C. B., Madsen, N. J., Munk-Jørgensen, P., & Hjorth, P. (2017). Interventions to improve lifestyle and quality-of-life in patients with concurrent mental illness and substance use. Nordic Journal of Psychiatry, 71(3), 197–204.
Kang, D., Fairbairn, C. E., & Ariss, T. A. (2019). A meta-analysis of the effect of substance use interventions on emotion outcomes. Journal of Consulting and Clinical Psychology, 87(12), 1106–1123. https://doi.org/10.1037/ccp0000450.
Kay-Lambkin, F. J., Baker, A. L., Lewin, T. J., & Carr, V. J. (2009). Computer-based psychological treatment for comorbid depression and problematic alcohol and/or cannabis use: A randomized controlled trial of clinical efficacy. Addiction, 104(3), 378–388. https://doi.org/10.1111/j.1360-0443.2008.02444.x.
Kotov, R., Gamez, W., Schmidt, F., & Watson, D. (2010). Linking "big" personality traits to anxiety, depressive, and substance use disorders: A meta-analysis. Psychological Bulletin, 136(5), 768–821. https://doi.org/10.1037/a0020327.
Krebs, A., D’Amato, C., Khade, N., Edgemon, T., Newsome, J., & Schweitzer Smith, M. (2021). Survey of Correctional Agencies to Determine the Impact of the COVID-19 Pandemic: University of Cincinnati.
Kroenke, K., Spitzer, R. L., Williams, J. B., & Löwe, B. (2009). An ultra-brief screening scale for anxiety and depression: The PHQ–4. Psychosomatics, 50(6), 613–621.
Lanesman, T. H., Gouse, H., Bantjes, J., Stein, D. J., & Lochner, C. (2019). Correlates and predictors of impulsivity in adults with methamphetamine use disorder. Journal of Substance Use, 24(4), 361–367. https://doi.org/10.1080/14659891.2019.1572803.
Lee, N. K., & Rawson, R. A. (2008). A systematic review of cognitive and behavioural therapies for methamphetamine dependence [10.1080/09595230801919494]. Drug and Alcohol Review, 27(3), 309–317. https://doi.org/10.1080/09595230801919494.
Liu, Y., Hao, B., Shi, Y., Xue, L., Wang, X., Chen, Y., & Zhao, H. (2017). Violent offences of methamphetamine users and dilemmas of forensic psychiatric assessment. Forensic Sciences Research, 2(1), 11–17.
Maltman, K., Savic, M., Manning, V., Dilkes-Frayne, E., Carter, A., & Lubman, D. I. (2020). ‘Holding on’and ‘letting go’: A thematic analysis of Australian parent’s styles of coping with their adult child’s methamphetamine use. Addiction Research & Theory, 28(4), 345–353.
Mattila, E., Lappalainen, R., Välkkynen, P., Sairanen, E., Lappalainen, P., Karhunen, L., … Ermes, M. (2016). Usage and dose response of a Mobile acceptance and commitment therapy app: Secondary analysis of the intervention arm of a randomized controlled trial. JMIR mHealth and uHealth, 4(3), e90.
McKetin, R., Boden, J., Foulds, J., Najman, J., Ali, R., Degenhardt, L., … Weatherburn, D. (2020). The contribution of methamphetamine use to crime: Evidence from Australian longitudinal data. Drug and Alcohol Dependence, 216, 108262. https://doi.org/10.1016/j.drugalcdep.2020.108262.
McKetin, R., Kothe, A., Baker, A., Lee, N., Ross, J., & Lubman, D. (2018). Predicting abstinence from methamphetamine use after residential rehabilitation: Findings from the methamphetamine treatment evaluation study [10.1111/dar.12528]. Drug and Alcohol Review, 37(1), 70–78. https://doi.org/10.1111/dar.12528.
McKetin, R., Leung, J., Stockings, E., Huo, Y., Foulds, J., Lappin, J., … Degenhardt, L. (2019). Mental health outcomes associated with of the use of amphetamines: A systematic review and meta-analysis. EClinical Medicine, 16, 81–97.
Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., … Wood, C. E. (2013). The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Annals of Behavioral Medicine, 46(1), 81–95.
Monaghesh, E., & Hajizadeh, A. (2020). The role of telehealth during COVID-19 outbreak: A systematic review based on current evidence. BMC Public Health, 20(1), 1193. https://doi.org/10.1186/s12889-020-09301-4.
Moos, R. H. (2007). Theory-based active ingredients of effective treatments for substance use disorders. Drug and Alcohol Dependence, 88(2), 109–121.
Moxley, V. B. A., Hoj, T. H., & Novilla, M. L. B. (2020). Predicting homelessness among individuals diagnosed with substance use disorders using local treatment records. Addictive Behaviors, 102, 106160. https://doi.org/10.1016/j.addbeh.2019.106160.
Potvin, S., Pelletier, J., Grot, S., Hébert, C., Barr, A. M., & Lecomte, T. (2018). Cognitive deficits in individuals with methamphetamine use disorder: A meta-analysis. Addictive Behaviors, 80, 154–160. https://doi.org/10.1016/j.addbeh.2018.01.021.
Radtke, T., Ostergaard, M., Cooke, R., & Scholz, U. (2017). Web-based alcohol intervention: Study of systematic attrition of heavy drinkers. Journal of Medical Internet Research, 19(6), e217.
Robinson, J., Sareen, J., Cox, B. J., & Bolton, J. M. (2011). Role of self-medication in the development of comorbid anxiety and substance use disorders: A longitudinal investigation. Archives of General Psychiatry, 68(8), 800.
Rubenis, A. J., Baker, A. L., & Arunogiri, S. (2021). Methamphetamine use and technology-mediated psychosocial interventions: A mini-review. Addictive Behaviors, 121, 106881. https://doi.org/10.1016/j.addbeh.2021.106881.
Šefránek, M., & Miovský, M. (2017). Treatment outcome evaluation in therapeutic communities in the Czech Republic: Changes in methamphetamine use and related problems one year after discharge. Journal of Groups in Addiction & Recovery, 12(2–3), 68–85. https://doi.org/10.1080/1556035X.2017.1280718.
Semple, S. J., Zians, J., Strathdee, S. A., & Patterson, T. L. (2008). Methamphetamine-using felons: Psychosocial and behavioral characteristics. American Journal on Addictions, 17(1), 28–35. https://doi.org/10.1080/10550490701756294.
Siefried, K. J., Acheson, L. S., Lintzeris, N., & Ezard, N. (2020). Pharmacological treatment of methamphetamine/amphetamine dependence: A systematic review. CNS Drugs, 34(4), 337–365. https://doi.org/10.1007/s40263-020-00711-x.
Şimşek, M., Dinç, M., & Ögel, K. (2019). Determinants of the addiction treatment drop-out rates in an addiction counseling Centre: A cross-sectional study. Psychiatry and Clinical Psychopharmacology, 29(4), 446–454. https://doi.org/10.1080/24750573.2018.1505283.
Skevington, S. M., Lotfy, M., & O'Connell, K. A. (2004). The World Health Organization's WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. A report from the WHOQOL group. Quality of Life Research, 13(2), 299–310.
Sundström, C., Gajecki, M., Johansson, M., Blankers, M., Sinadinovic, K., Stenlund-Gens, E., & Berman, A. H. (2016). Guided and unguided internet-based treatment for problematic alcohol use – A randomized controlled pilot trial. PLoS One, 11(7), e0157817. https://doi.org/10.1371/journal.pone.0157817.
Torous, J., Lipschitz, J., Ng, M., & Firth, J. (2020). Dropout rates in clinical trials of smartphone apps for depressive symptoms: A systematic review and meta-analysis. Journal of Affective Disorders, 263, 413–419.
Wang, L., Weiss, J., Ryan, E. B., Waldman, J., Rubin, S., & Griffin, J. L. (2021). Telemedicine increases access to buprenorphine initiation during the COVID-19 pandemic. Journal of Substance Abuse Treatment, 124, 108272. https://doi.org/10.1016/j.jsat.2020.108272.
Ward, J., Elison-Davies, S., Davies, G., Dugdale, S., & Jones, A. (2019). Clinical and demographic patient characteristics, alcohol treatment goal preference and goal attainment during computer-assisted therapy with breaking free online. Journal of Substance Use, 24(6), 681–687.
Wiesner, M., Kim, H. K., & Capaldi, D. M. (2005). Developmental trajectories of offending: Validation and prediction to young adult alcohol use, drug use, and depressive symptoms. Development and Psychopathology, 17(1), 251–270. https://doi.org/10.1017/s0954579405050133.
Williams, C., & Garland, A. (2002). A cognitive–behavioural therapy assessment model for use in everyday clinical practice. Advances in Psychiatric Treatment, 8(3), 172–179.
Center for Behavioral Health Statistics and Quality. (2020). Results from the 2019 National Survey on drug use and health. https://www.samhsa.gov/data/
Dadhe, G., & Bettman, C. (2019). The lived experiences of adult crystal methamphetamine users: A qualitative study. Psychotherapy and Counselling Journal of Australia, 7(1), e1.
Elison-Davies, S., Wardell, J., Quilty, L., Ward, J., & Davies, G. (2021). Examining correlates of cannabis users’ engagement with a digital intervention for substance use disorder: An observational study of clients in UK services delivering ‘breaking free online’. Journal of Substance Abuse Treatment, 123(4), e1.
Eysenbach, G. (2005). The law of attrition. Journal of Medical Internet Research, 7(1), e1.
Office for Health Improvement and Disparities. (2021). National statistics: Adult substance misuse treatment statistics 2020 to 2021 - report. https://www.gov.uk/government/statistics/substance-misuse-treatment-for-adults-statistics-2020-to-2021/adult-substance-misuse-treatment-statistics-2020-to-2021-report
Acknowledgments
The authors would like to thank all the treatment clients and staff who have supported the development and delivery of the Breaking Free from Substance Abuse program over the past decade.
Funding
Not applicable – no funding was obtained for this study.
Author information
Authors and Affiliations
Contributions
SED led on study conception and design, obtained ethical approval, analysed data, and drafted the manuscript; JN reviewed the data analysis and provided reviewed and revised the manuscript; AJ reviewed the data analysis and provided reviewed and revised the manuscript; GD reviewed and revised the manuscript; JW reviewed and revised the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Approval to analyze data provided by participants was granted by the ODRC Human Subjects Research Review Committee on May 3rd 2021 – all participants provided consent for their data to be used for research purposes.
Consent for publication
Not applicable.
Competing interests
SED, GD and JW are all employed by LifeWorks where the Breaking Free Online program has been developed.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Elison-Davies, S., Newsome, J., Jones, A. et al. Associations between psychosocial risk factors, and changes in substance dependence and psychosocial functioning, during engagement with digital cognitive behavioral therapy for methamphetamine use: use of 'Breaking Free from Substance Abuse' by incarcerated people during the COVID-19 pandemic. Health Justice 10, 28 (2022). https://doi.org/10.1186/s40352-022-00190-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40352-022-00190-w