
Abstract
Background
Angiosarcoma of the gallbladder is a rare diagnostic entity rarely encountered by pathologists and has rarely been reported in literature. This review aimed to examine the clinicopathological features, immunohistochemistry, treatment, and outcomes of gallbladder angiosarcoma.
Methods
A search of the PubMed, Science Direct and Google Scholar was done with the search terms ("angiosarcoma" OR "angiosarcomas") AND ("gallbladder" OR "gallbladders"). Based on inclusion and exclusion criteria, only case reports could be used for this review.
Result
8 case reports were chosen in the end for analysis. The mean age of the patients at presentation was 65 years. It was most frequently observed in males. Abdominal pain and palpable mass were the most commonly reported symptoms. Cholelithiasis and anemia were also reported. On histopathology morphologically epithelioid appearance of angiosarcoma was evident. Cytokeratin (CK) AE1/AE3, Von willebrand factor, Factor VIII antigen, Vimentin, CD31 were positive. Meanwhile, UEA, CD34, CD117, S-100, Keratin, EMA, and CEA showed negative outcome. Surgery was the preferred method of treatment and a mean 10-months follow-up was done.
Conclusion
Despite the unavailability of convincing data, histological and immunohistochemical analyses play a major role in the diagnosis of gallbladder angiosarcoma. Nevertheless, more comprehensive clinical studies are required to provide universal guidelines for the treatment and diagnosis of angiosarcoma of the gallbladder.
Similar content being viewed by others


Introduction
Angiosarcoma is a malignancy, vascular tumors, resembling endothelial differentiation in terms of morphology or immunophenotype. It has invasive nature with high likely hood of distal metastasis and poor survival. (1) Roughly, 2–3% of all soft tissue sarcomas in adults are angiosarcomas. (2) Majority of times, etiology is unknown, however, radiation, chronic lymphedema (Stewart-Treves syndrome), exposure to vinyl chloride, arsenic and thorium dioxide (Thorotrast), and surgically implanted foreign materials are some of the risk factors. Moreover, some angiosarcomas are associated with some syndromes such as neurofibromatosis, Maffucci syndrome, and nerve sheath tumors) [1, 3,4,5].
Majority of angiosarcoma cases stem from head and neck and breast region [6]. On the other hand, angiosarcoma of the gastrointestinal tissue is rare [7, 8]. Furthermore, angiosarcoma of the gallbladder is so rare which all related data is mentioned in the case reports to the best of our knowledge [8,9,10,11]. Therefore, in the following article, we have reviewed comprehensively gallbladder angiosarcoma reported cases in regards to demographics characteristics, clinical features, gross findings, histopathology, immunohistochemistry, treatment, and follow-up.
Materials and methods
Search strategy
A literature review was performed according to the preferred reporting items for systematic reviews and meta‐analyses statement. A search of the PubMed, Science Direct and Google Scholar was done with the search terms ("angiosarcoma" OR "angiosarcomas") AND ("gallbladder" OR "gallbladders"). The search was completed on October 2023. The results were limited to human‐subject and English‐language articles. All abstracts were analyzed, and full‐ text articles which were open access were obtained when inclusion criteria were fulfilled. Studies and publications with insufficient data or incomplete information were excluded. Additionally, manual search was also performed from the subsequent full‐text articles reviewed to identify additional relevant articles.
Selection criteria
Our initial intention was to find studies with large sample size. Nonetheless, upon a comprehensive search, we decided to include all case reports due to scarcity of larger studies of angiosarcoma of gallbladder with high sample size. Exclusion criteria were non‐English language, animal, nonobtainable full‐text studies, and studies with insufficient data. A quality assessment tool, the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Case Reports, was used. The quantitative analysis was performed by combining data in their original metric.
Data extraction
Variables included author, year of publication, patient demographics, clinical findings, medical history, lab data, radiological and pathological findings, ultra-structural findings, immunohistochemistry, metastasis, treatment, follow-ups and survival data. Data analyses were performed with Microsoft Excel 2018 (Microsoft Corp., Redmond, WA, USA).
Results
Primary search of PubMed, ScienceDirect and Google Scholar search was performed with 890 articles. (Fig. 1) In the end, 8 case reports were included for quantitative synthesis. (Table 1) The results are as follows:
-
1.
Sex

PRISMA flow chart of the extracted articles regarding gallbladder angiosarcoma
Data was available for 8 patients, of whom 37.5% (n = 3) were females and 62.5% (n = 5) were males.
-
2.
Age
The average was 65 years, with a range from 54 to 81 years. The mean age for females was 73.6 years and for males 59.8 years.
-
3.
Clinical features
Epigastric pain and abdominal mass were the most common symptoms. Moreover, nausea, vomiting, dizziness, melena and rectal bleeding were reported. The mean duration of symptoms were 6.3 weeks with a range of 2 to 12 weeks in general. Cholelithiasis was the most common finding in the past medical history. Anemia was reported in 3 cases.
-
4.
Radiological findings
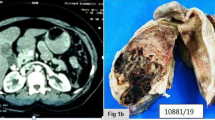
Computed tomography (CT scan) of abdomen showed distended and edematous gallbladder with a large hematoma in the lumen (n = 1), gross dilation of the gallbladder (n = 1), and free intraperitoneal blood and a mass at gallbladder fossa (n= 1). In addition, ultrasound revealed gross echogenic formations and areas of hyperechogenic (n = 1), sonolucent area at the inferior aspect of the right lobe of the liver (n = 1), and an echo productive area adjacent to the posterior wall of the gallbladder (n = 1).
-
5.
Pathological findings
Macroscopically, gallbladders of two patients showed polypoid masses with gangrenous walls and perforated thick-walled gallbladder surrounded by omental adhesions and abscesses. Transmural infiltration by tumors cells in 2 cases, morphologically epithelioid appearance of angiosarcoma in 3 cases, and mitotic figures in 2 patients were detected. In one of the patients, the neoplastic cells tended to form vascular lacunae containing erythrocytes, with interposition of amyloid-like stroma. Also, mucosa of gallbladder showed extensive ulceration and necrosis. Furthermore, large round to oval vesicular nucleus, a single prominent basophilic nucleolus, intracytoplasmic vacuoles containing erythrocytes, and abundant pale eosinophilic cytoplasm was evident. Regarding findings of another patient, nuclear pleomorphism and hyperchromatism was prominent, particularly in tumor cells lining cleft-like or anastomosing vascular channels angiosarcoma.
-
6.
Immunohistochemistry
Among immunohistochemical stains, Cytokeratin (CK) AE1/AE3 was positive in one case. von Willebrand factor antibodies and Factor VIII antigen were reported positive in one case. CD 31 resembled positive findings in 2 cases. Vimentin was positive in 2 cases. Moreover, UEA, CD34, CD117, S-100, Keratin, EMA, and CEA demonstrated negative result in one of the patients.
-
7.
Metastasis
Out of the data of 8 patients, metastasis was reported in 5 cases. Metastatic sites were peritoneum, abdominal lymph nodes, pancreas, spleen, stomach, intestines, lungs, adrenals, bone, liver, and ovaries.
-
8.
Treatment
Surgical intervention, cholecystectomy, was performed for 7 patients. One patient refused treatment. In one of the cases, pre-operational ultrasound-guided percutaneous gallbladder drainage and resection of hepatic segment IV along with cholecystectomy were performed.
-
9.
Follow-up
The mean follow‐up for patients was found in 8 cases with a mean of 10 months. At the time of the follow-up, 3 patients were alive and 5 were dead. However, prognosis could not be defined.
Discussion
Definition
Angiosarcoma is defined as the rapid and extensive infiltrative overgrowth of vascular endothelial cells. It resembles local invasion with high possibility of involvement of lymph nodes and metastasis. High expression of vascular specific receptor tyrosine kinases including TIE1, KDR, TEK, FLT, and VEGF leads to endothelial cell expansion, angiogenesis, and vascular leaks [2, 6, 10, 12, 13].
Demographic and clinical features
Angiosarcomas of the gastrointestinal tract are such rare neoplasms that their exact incidence is still not known [11, 14]. Angiosarcomas of the gallbladder, according to our knowledge, have been described in 8 case reports [6, 9, 15, 16]. Men were more involved in such cases and the mean age of patients was 65. Association between histological grade and clinical outcomes has been investigated and angiosarcoma is not routinely graded [13, 16,17,18]. Possibly, cholelithiasis has been advocated for the etiology of gallbladder tumors in general, because of its frequent coexistence with them. Vaittinen et al reported cholelithiasis to be present in 79% of sarcomas of the gallbladder [7,8,9,10,11, 14, 16, 19,20,21]. Though the underlying casus requires deeper establishment, it is said that the irritation due to stones and accompanying inflammation can trigger the development of gallbladder tumors, and hence, angiosarcomas. [22] Clinical symptoms of angiosarcomas of the gallbladder apparently are the same as gallbladder carcinomas. Nevertheless, the diagnosis took shorter period of time as a result of speedy tumoral progression [21].
Diagnosis of angiosarcoma relies on histopathologic examination, since CT scans, ultrasound, or X-rays, can reveals a general suspicion of a tumoral mass. Because of the very limited experience, no definite guideline for treatment exists. As far, surgical intervention remains as the first conventional and reliable treatment. To elaborate more, cholecystectomy with or without wedge resection or extended right hepatic resection, and regional lymph node dissection are performed in majority of cases [22]. Moreover, there is dilemma in including chemotherapy and/or radiotherapy adjacent to surgery in the treatment approach [21]. In one study, age more than 50, tumor larger than 5 cm, and mode of treatment (multimodal versus other) were independent negative prognostic variables [5, 12, 13, 15, 16, 23].
Pathology
Since a well-differentiated tumor may mimic a hemangioma or hematoma on histology, diagnosis of angiosarcoma cause challenges for clinicians. Detection of endothelial cells with nuclear atypia, abundant mitotic figures, and necrosis could indicate presence of a malignant vascular tumor. The sole histologic variable appearing to have a prognostic implication was mitotic activity. In fact, cases with greater than ten mitoses in high power fields were uniformly fatal within a mean of two years of diagnosis.
On performing immunohistochemistry for ruling out differential diagnosis, vascular markers CD31, CD34 and Factor VIII are specific in differentiating between carcinomas and vascular neoplasms. However, there may be additional difficulties encountered in attempting to differentiate between other neoplasms that stain with vascular markers. Positive immunohistochemical staining for vascular markers may be helpful in differentiating an epithelioid vascular neoplasm from an epithelial neoplasm. Epithelioid angiosarcoma tends to grow in diffuse sheets with larger more pleomorphic cells which contains prominent nucleoli and subtle cleft indicative of vascular differentiation. It is necessary to distinguish Epithelioid hemangioendothelioma (EHE), a vascular neoplasm resembling aggressive behavior and multifocal involvement, from epithelioid angiosarcoma [24]. Moreover, the differential diagnosis of a deep-seated epithelioid neoplasm also consists of malignant melanoma (primary or metastatic), proximal-type epithelioid sarcoma, and epithelioid malignant peripheral nerve sheath tumor. Although such tumors lack true vascular differentiation on histology, immunohistochemistry can play a role in differentiating them. S-100 can be used to ruling out melanoma and epithelioid malignant peripheral nerve sheath tumor [7]. Additionally, CD31 and von Willebrand factor antibodies are helpful in cases of epithelioid angiosarcoma, since it can mimic a poorly differentiated carcinoma on histological investigations. In about one-third of the patients, expression of cytokeratin was positive in epithelioid angiosarcoma. Despite the fact that Weibel Palade bodies presence were negative in angiosarcoma of gallbladder, it played a major diagnostic role in diagnosis of epithelioid angiosarcoma [1, 2, 4,5,6, 12, 13, 16, 17, 22, 25].
Follow-up
Based on the findings the included case reports, 3 cases survived the surgery and resembled no recurrence in their follow-ups [2, 9, 14]. On the other hand, one of the patients refused the surgical intervention and died of hepatorenal failure [8]. In 3 of the case reports, patients did not survive due to sepsis, metastasis, hemorrhagic shock in months after their surgeries [10, 11, 21]. Moreover, one of the patients underlying cause of death is unknown [20].
Conclusions
Our study reviewed all cases of gallbladder angiosarcoma in the literature and summarized their main features. Angiosarcoma of the gallbladder is a rare condition. The relationship of cholelithiasis and gallbladder angiosarcoma requires further clinical investigation. However, mitotic activity was associated with poor prognosis. Despite the scarcity of available data, histological and immunohistochemical analyses appear to play a major role in the diagnosis of angiosarcoma of the gallbladder. Nonetheless, further clinical studies are required to organize a comprehensive universal guideline for the treatment and diagnosis of angiosarcoma of the gallbladder.
Availability of data and materials
Not applicable.
References
Espat NJ, Lewis JJ, Woodruff JM, Antonescu C, Xia J, Leung D, et al. Confirmed angiosarcoma: prognostic factors and outcome in 50 prospectively followed patients. Sarcoma. 2000;4(4):173–7.
Cao J, Wang J, He C, Fang M. Angiosarcoma: a review of diagnosis and current treatment. Am J Cancer Res. 2019;9(11):2303–13.
Mentzel T, Katenkamp D. Intraneural angiosarcoma and angiosarcoma arising in benign and malignant peripheral nerve sheath tumours: clinicopathological and immunohistochemical analysis of four cases. Histopathology. 1999;35(2):114–20.
Jennings TA, Peterson L, Axiotis CA, Friedlaender GE, Cooke RA, Rosai J. Angiosarcoma associated with foreign body material: a report of three cases. Cancer. 1988;62(11):2436–44.
Webster P, Wujanto L, Fisher C, Walker M, Ramakrishnan R, Naresh K, et al. Malignancies confined to disused arteriovenous fistulae in renal transplant patients: an important differential diagnosis. Am J Nephrol. 2011;34(1):42–8.
Fury MG, Antonescu CR, Van Zee KJ, Brennan MF, Maki RG. A 14-year retrospective review of angiosarcoma: clinical characteristics, prognostic factors, and treatment outcomes with surgery and chemotherapy. Cancer J. 2005;11(3):241–7.
Allison KH, Yoder BJ, Bronner MP, Goldblum JR, Rubin BP. Angiosarcoma involving the gastrointestinal tract: a series of primary and metastatic cases. Am J Surg Pathol. 2004;28(3):298–307.
Rosansky SJ, Mullens CC. The hepatorenal syndrome associated with metastatic angiosarcoma of the gallbladder. Ann Intern Med. 1982;96(2):191–2.
Costantini R, Di Bartolomeo N, Francomano F, Angelucci D, Innocenti P. Epithelioid angiosarcoma of the gallbladder: case report. J Gastrointest Surg. 2005;9(6):822–5.
Odashiro AN, Pereira PR, Odashiro Miiji LN, Nguyen GK. Angiosarcoma of the gallbladder: case report and review of the literature. Can J Gastroenterol. 2005;19(4):257–9.
White J, Chan YF. Epithelioid angiosarcoma of the gallbladder. Histopathology. 1994;24(3):269–71.
Rossi S, Fletcher CD. Angiosarcoma arising in hemangioma/vascular malformation: report of four cases and review of the literature. Am J Surg Pathol. 2002;26(10):1319–29.
Lahat G, Dhuka AR, Hallevi H, Xiao L, Zou C, Smith KD, et al. Angiosarcoma: clinical and molecular insights. Ann Surg. 2010;251(6):1098–106.
Kumar A, Singh MK, Kapur BM. Synchronous double malignant tumors of the gall bladder: a case-report of squamous cell carcinoma with an angiosarcoma. Eur J Surg Oncol. 1994;20(1):63–7.
Park G, Park WS, Lee SK, Kim JO. A rare collision tumor comprising intracystic papillary neoplasm associated with adenocarcinoma and angiosarcoma in the gallbladder. Korean J Intern Med. 2020;35(3):732–3.
Vorburger SA, Xing Y, Hunt KK, Lakin GE, Benjamin RS, Feig BW, et al. Angiosarcoma of the breast. Cancer. 2005;104(12):2682–8.
Torres KE, Ravi V, Kin K, Yi M, Guadagnolo BA, May CD, et al. Long-term outcomes in patients with radiation-associated angiosarcomas of the breast following surgery and radiotherapy for breast cancer. Ann Surg Oncol. 2013;20(4):1267–74.
Naka N, Ohsawa M, Tomita Y, Kanno H, Uchida A, Myoui A, et al. Prognostic factors in angiosarcoma: a multivariate analysis of 55 cases J. Surg Oncol. 1996;61(3):170–6.
Vaittinen E. Sarcoma of the gallbladder. Ann Chir Gynecol Fenn. 1972;61:185–9.
Kawai T, Hirose Y, Ainota T, Miyazaki Y, Yamamoto Y, Ikeda M, et al. A case of hemangiosarcoma of the gallbladder. Nihon Shokakibyo Gakkai Zasshi. 1989;86(11):2611–6.
Kumar A, Lal BK, Singh MK, Kapur BM. Angiosarcoma of the gallbladder. Am J Gastroenterol. 1989;84(11):1431–3.
Glenn F, Hays DM. The scope of radical surgery in the treatment of malignant tumors of the extrahepatic biliary tract. Surg Gynecol Obstet. 1954;99(5):529–41.
Meis-Kindblom JM, Kindblom LG. Angiosarcoma of soft tissue: a study of 80 cases. Am J Surg Pathol. 1998;22(6):683–97.
Weiss SW, Ishak KG, Dail DH, Sweet DE, Enzinger FM. Epithelioid hemangioendothelioma and related lesions. Semin Diagn Pathol. 1986;3(4):259–87.
Hasegawa T, Matsuno Y, Shimoda T, Umeda T, Yokoyama R, Hirohashi S. Proximal-type epithelioid sarcoma: a clinicopathologic study of 20 cases. Mod Pathol. 2001;14(7):655–63.
Acknowledgements
Not applicable.
Funding
This study received no funding or financial support.
Author information
Authors and Affiliations
Contributions
MS and SR provided the main idea of this study. MS, HRJ, and SR wrote the manuscript and did the final revision. SD and HRJ gathered data and analyzed it. MS submitted the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal
Competing interests
There is no competing of interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Salehi, M., Rehman, S., Davis, S. et al. Angiosarcoma of gallbladder, a literature review. J Med Case Reports 18, 62 (2024). https://doi.org/10.1186/s13256-023-04323-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13256-023-04323-z