
Abstract
Background
Significant lower genital tract (LGT) dysbiosis and an associated lower rate of clinical pregnancy after in vitro fertilization–frozen embryo transfer (IVF-FET) among polycystic ovary syndrome (PCOS) patients have been previously reported by our group. We aimed to assess whether transvaginal Lactobacillus supplementation can reverse LGT dysbiosis and further improve perinatal outcomes in PCOS patients after IVF-FET.
Methods/design
This is a protocol for a multicenter, open-label, randomized controlled trial in China. Women diagnosed with PCOS who are undergoing IVF-FET treatment will be recruited. Allocation to the intervention/control arms at a ratio of 1:1 will be executed by an electronic randomization system. Participants in the intervention arm will receive the live Lactobacillus capsule vaginally for 10 consecutive days before embryo transfer, while those in the control arm will receive standard individualized care. The primary outcomes will be the clinical pregnancy rate, implantation rate, and live birth rate. 16S rRNA sequencing and liquid chromatography–mass spectrometry will be conducted to evaluate the LGT microbiome and systemic metabonomics before and after the intervention. A sample of 260 participants will provide 95% power to detect a 20% increase in the rate of clinical pregnancy (α = 0.025, one-tailed test, 15% dropout rate). A total of 300 participants will be recruited.
Discussion
This is the first large and multicenter randomized controlled trial aimed at assessing the efficacy of transvaginal Lactobacillus supplementation on restoring the LGT microbiome and improving perinatal outcomes in PCOS patients after IVF-FET. This pragmatic trial is promising for increasing the rates of clinical pregnancy and live birth in PCOS patients after IVF-FET.
Ethics and dissemination
Ethical review approval was obtained from the Medical Research Ethics Committees of the International Peace Maternity and Child Health Hospital of Shanghai Jiao Tong University (15 October 2020, GKLW 2020-29). To maximize dissemination, these findings will be reported in open access publications in journals with high impact, and oral and poster conference presentations will be performed.
Trial registration
ChiCTR ChiCTR2000036460. Registered on 13 September 2020, https://www.chictr.org.cn/showproj.html?proj=59549.
Similar content being viewed by others


Background
Polycystic ovarian syndrome (PCOS) is one of the most common endocrinopathies among women of reproductive age, affecting approximately 10–15% of women worldwide, and is one of the most common causes of female infertility [1, 2]. According to the Rotterdam criteria, two of the following three criteria must be fulfilled for a PCOS diagnosis: hyperandrogenism, oligo-ovulation or anovulation, and polycystic ovarian morphology defined by the presence of ≥ 12 follicles with a maximum diameter of 2–9 mm in either ovary [3, 4]. Women with PCOS are at a high risk of infertility due to anovulation. In vitro fertilization–frozen embryo transfer (IVF-FET) provides a valuable choice for PCOS patients who desire to become pregnant. However, once pregnant, women with PCOS are more susceptible to recurrent miscarriage, gestational diabetes mellitus (GDM), hypertension disorders in pregnancy, etc. [5, 6].
Our previous study showed that the bacterial genus diversity was higher in the lower genital tract (LGT), including the vagina and cervical canal, in PCOS patients. Additionally, the abundance of Lactobacillus spp. was significantly reduced in the LGT of PCOS patients. Pathway enrichment analysis showed that the top pathways were beneficial to the growth of pathogenic species, including Gardnerella [7]. Importantly, we found that in PCOS patients undergoing IVF-FET, those with Lactobacillus deficiency in the LGT had significantly lower rates of embryo implantation and clinical pregnancy (unpublished data), suggesting a potential role of reversing LGT dysbiosis in improving perinatal outcomes in PCOS patients after IVF-FET. However, large-scale and multicenter randomized clinical trials (RCTs) examining the effect of a vaginal Lactobacillus intervention on improving pregnancy outcomes in PCOS patients with LGT flora dysbiosis are unavailable.
The use of probiotics mainly containing Lactobacillus spp. was previously reported to have benefits in the treatment of vaginal diseases. A recent meta-analysis (n = 2321) showed that probiotic therapy resulted in a beneficial outcome in the treatment of bacterial vaginosis [8]. Compared with antibiotic therapy for bacterial vaginosis, which has high failure and recurrence rates, probiotics are recognized as valuable alternative strategies for their significant role in reestablishing the physiological vaginal environment and improving the local immune response with fewer adverse effects, further relieving clinical symptoms [9]. Moreover, a meta-analysis systematically reviewed the beneficial outcomes of probiotic treatment for women with GDM, including maternal and infant health and well-being [10].
PCOS patients were reported to have metabolic disorders, mainly hyperandrogenism, insulin resistance, dyslipidemia, and derangements in carbohydrate and hormonal metabolism [4, 11,12,13,14,15]. Moreover, studies reported that metabolic profiling and the vaginal microbiome were associated with adverse perinatal outcomes such as preterm birth [16]. However, the changes in metabonomics in the LGT and their interactions with systemic metabolic status in PCOS patients remain unknown, as do their effects on IVF–FET and maternal and infant health outcomes. Given the adverse perinatal effects of LGT dysbacteriosis on PCOS patients and the promising benefits of reversing LGT dysbacteriosis on improving the perinatal outcomes of PCOS patients, we designed this multicenter, open-label RCT to provide an accessible and effective therapy to better improve the perinatal outcomes and health of PCOS patients with LGT dysbiosis who are undergoing IVF–FET.
Methods/design
Objectives
We plan to conduct the present trial to evaluate the effects of supplementation with live Lactobacillus capsules for vaginal use on reversing LGT dysbiosis and improving perinatal outcomes in PCOS patients undergoing IVF-FET.
Study design and setting
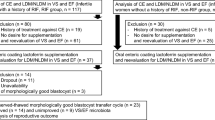
This proposed study is a prospective, multicenter, open-label RCT. A total of 300 eligible participants will be recruited from 4 different tertiary hospitals, including ± 100 participants from the International Peace Maternity and Child Health Hospital, ± 50 participants from Ruijin Hospital, ± 50 participants from Zhongshan Hospital, and ± 100 participants from ShangHai JIAI Genetics and IVF Institute. A flowchart of participant enrollment and screening, randomization, and follow-up and sample collection is shown in Fig. 1.

Flowchart for recruitment, screening, allocation, intervention, and follow-up of study participants. PCOS, polycystic ovary syndrome; qPCR, quantitative polymerase chain reaction; FET, frozen embryo transfer; HCG, human chorionic gonadotropin
Participants
Inclusion criteria
A total of 20- to 35-year-old women who have been diagnosed with PCOS according to the Rotterdam Criteria and plan to undergo IVF–FET will be recruited. Quick screening of the abundance of Lactobacillus spp. will be performed by real-time quantitative polymerase chain reaction (RT–qPCR), which will be specified later. Women with PCOS with Lactobacillus spp. accounting for less than 80% of the vaginal microbiome who volunteer to participate will be eligible for this study.
Exclusion criteria
We will exclude individuals if they have been diagnosed with the following disorders: Cushing’s syndrome, congenital adrenal hyperplasia, thyroid disorder, hyperprolactinemia, androgen-secreting tumors, congenital malformations of the reproductive tract, systemic lupus erythematosus or any other autoimmune disease, HIV, endometriosis, uterine fibroids or colpitis. The subjects should not receive hormones, antibiotics, or vaginal medication within 7 days or cervical treatment or flushing within 5 days of the start of the study. Moreover, sexual activities should not be carried out within 48 hours. Women who undergo preimplantation genetic testing will also be excluded.
Withdrawal of participants
Participants will be clearly informed by investigators at enrollment that they may withdraw from this RCT at any period for any reason without penalty. A withdrawal statement will be provided and signed. Written consent forms will be obtained if the individual agrees to receive continued follow-up for associated clinical outcomes after withdrawal.
Procedure
The study procedure is described by following the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) checklist (Additional file 1).
Recruitment and randomization
The clinical research coordinators (CRCs) will verbally inform PCOS patients that the hospital is currently conducting a multicenter clinical trial to better improve the outcomes of IVF–FET in PCOS patients with vaginal microbiota dysbiosis. If they fully understand and are willing to take part in the study, they will meet a CRC in person at the hospital, sign an informed consent form, and officially join the study on the first day of the current IVF–FET cycle. The CRCs will later inform patients of whether they have vaginal microbiota dysbiosis. Basic information, including sociodemographic characteristics and clinical history, will be collected by the CRCs using standardized questionnaires and recorded into an online and password-protected electronic data collection system (Clinical Research Integrated Platform [CRIP], https://crip-ec.shdc.org.cn, supported by Shanghai Hospital Development Center, Shanghai, China), which will automatically generate a sequential code and randomly allocate participants to the intervention group or the control group at a ratio of 1:1 based on the whole study population. The research doctors will manage the study group allocation. Given the nature of vaginal use of live Lactobacillus capsules before FET, the investigators and participants will be informed of the assignment. To ensure the reality of this study, independent statisticians will be recruited, and they will be blinded to the group allocation.
Sample collection
Two vaginal swabs, 2 cervical canal swabs, and 3 ml of peripheral blood will be collected on the day of the first clinic visit and the day of embryo transfer (ET). Vaginal swabs will be collected directly, while cervical canal swabs will be collected carefully through a vaginal dilator device to avoid contamination from contact with the vagina. Vaginal and cervical canal swabs will be immediately collected in a clean 2-ml DNA LoBind tube and immediately placed on ice and transferred to a − 80 °C freezer within 2 h, followed by DNA extraction. Peripheral venous blood will be collected in coagulation-enhancing disposable vacuum blood collection tubes. Blood will be centrifuged at 2000 rpm for 20 min at 4 °C (Eppendorf, Germany). Serum will be isolated and divided into 2 tubes and immediately frozen at − 80 °C until use.
DNA extraction and quick screening by quantitative PCR
DNA extraction from a vaginal swab will be performed using the DNeasy Power Soil kit (12888, QIAGEN) according to the manufacturer’s instructions. The quantity and quality of DNA will be assessed by a NanoDrop 2000 (Thermo Fisher Scientific, USA). Quick screening for the relative abundance of Lactobacillus spp. in the vaginal microbiome will be performed by qPCR. The relative abundance of Gardnerella vaginalis and subtypes of Lactobacillus spp., including Lactobacillus jensenii, Lactobacillus crispatus, and Lactobacillus ineris, will also be evaluated. The sequences of primers used in qPCR are presented in Table 1. DNA will be amplified with TB Green® Premix Ex Taq™ (Tli RNaseH Plus) (RR420, Takara) using an ABI QuantStudio™ 7 Flex Real-Time PCR System. The abundance of Lactobacillus spp. will be calculated relative to that of total bacteria.
Intervention
For the intervention group, a live Lactobacillus capsule (> 1 × 106 CFU/g, National Medicine Approval Number: S20030005, Inner Mongolia Shuangqi Pharmaceutical Co., Ltd., PRC) will be administered vaginally.
The live Lactobacillus capsule has been reported to be effective for bacterial vaginosis treatment with fewer adverse effects than antibiotics, and probiotic treatment for women with GDM has been reported to improve maternal and infant health outcomes [10, 17,18,19]. In the intervention group, 1 live Lactobacillus capsule per day will be applied transvaginally for 10 consecutive days starting on the initiation day of the FET cycle. Medical gloves will be included in the pill box, and the pills will be stored at 2–8 °C until use. The usage will be explained to the participants by the CRCs. A well-designed medication diary will be prepared to help remind patients and assist them in recording the process of medication administration (Table 2). Regular follow-up will be performed on day 5 and day 10 in both groups by phone call. Any adverse response will be recorded and reported at any time.
Standard care
All participants in both groups will receive optimally personalized endometrial preparation regimens. The medication regimens will be recorded in detail, including the dose, frequency, and duration of use of the medication.
Participant timeline
The time schedule of enrollment, intervention, follow-up and outcome assessments is shown in Table 3. After undergoing ovulation, egg retrieval, IVF, and advanced embryo freezing, PCOS patients will move on to the next step of endometrial preparation for FET. The duration of endometrial preparation will continue for approximately 14 days. At the 1st clinical visit on the first day of the current FET cycle, written informed consent, baseline information, 2 vaginal swabs, 2 cervical canal swabs, and 3 ml peripheral blood will be obtained at enrollment. After quick screening for the relative abundance of Lactobacillus spp. in vaginal flora, the participants will be informed of whether they have LGT dysbiosis and the results of randomization. At the 2nd visit after enrollment, in the control group, participants with LGT dysbiosis will confirm the next contact, while the intervention group will administer live Lactobacillus capsules vaginally and will be provided a medication diary. All participants will be followed up 5 times in the clinic or by phone call. The 3rd visit after 5 days of drug administration will mainly be about whether any adverse response occurs. At the 4th visit after 10 days of drug administration, the medication diary will be checked and reviewed, and any adverse response will be recorded and reported. At the 5th visit on the day of ET, 2 vaginal swabs, 2 cervical canal swabs, and 3 ml peripheral blood will be obtained from participants in both groups. At the 1st follow-up after 14 days of ET, human chorionic gonadotropin (HCG) and progesterone (P) levels will be determined as standard clinical procedures. If the HCG test is positive, the 2nd follow-up will occur approximately 5 weeks after ET, and clinical pregnancy will be confirmed by ultrasound and recorded in the CRIP system. At the 3rd follow-up, the fetal developmental situation and maternal obstetric complications at approximately 24-28 gestational weeks, if any, will be carefully recorded. The endpoint of follow-up is live birth, and maternal and neonatal information will be obtained.
16S rRNA amplicon sequencing
For the analysis of bacterial diversity, V3-V4 variable regions of 16S rRNA genes will be amplified with universal primer pairs 343F (5′-TACGGRAGGCAGCAG-3′) and 798R (5′-AGGGTATCTAATCCT-3′) [20]. 16S rRNA sequencing will be performed on an Illumina NovaSeq 6000 with 250 bp paired-end reads (Illumina Inc., San Diego, CA; OE Biotech Company; Shanghai, China).
Liquid chromatography–mass spectrometry (LC–MS) for metabonomic analysis
An ACQUITY UPLC I-Class system (Waters Corporation, Milford, USA) coupled with a VION IMS QTOF mass spectrometer (Waters Corporation, Milford, USA) will be used to analyze the metabolic profile in both ESI positive and ESI negative ion modes.
Proposed outcome measurement
Primary outcome
The clinical pregnancy rate will be the primary outcome. The clinical pregnancy rate is defined as the ratio of the clinical pregnancy (one or more observed gestational sacs with a fetal heartbeat in the uterus under ultrasonography 28 days after embryo transfer) to the number of transplant cycles.
Secondary outcomes
Maternal outcomes
The implantation rate is defined as the number of gestational sacs in the uterus divided by the number of embryos transferred. The live birth rate is defined as the delivery of any viable infant at 25 weeks of gestation or more after initial embryo transfer to the number of transplant cycles. The biochemical pregnancy rate is defined as the ratio of biochemical pregnancies (serum hCG level >5 mIU/L 14 days after embryo transfer) to the number of transplant cycles. The spontaneous abortion rate is defined as the ratio of spontaneous abortions (spontaneous pregnancy loss before 20 weeks of gestation) to the number of transplant cycles. The ongoing pregnancy rate is defined as the ratio of ongoing pregnancies (intrauterine live fetus under ultrasonography after 20 weeks of gestation) to the number of transplant cycles. The preterm birth rate is defined as the ratio of preterm births (delivery at ≥ 28 and < 37 weeks of gestation) to the number of transplant cycles. Pregnancy complications, including GDM, hypertensive disorders of pregnancy, including gestational hypertension and preeclampsia, placental abruption, preterm/prelabor/rupture of membranes, birth mode (vaginal delivery/operational vaginal delivery/selective or emergency cesarean section), blood loss during birth, and postpartum hemorrhage, adherence to the intervention and maternal mortality, will be followed up and assessed. A GDM diagnosis will be made according to the diagnostic criteria of the American Diabetes Association based on the results of the 75-g oral glucose tolerance test (OGTT) at 24–28 gestational weeks (fasting venous glucose level ≥ 5.1 mmol/L, 1-h value ≥ 10.0 mmol/L, 2-h value ≥ 8.5 mmol/L) [21]. Gestational hypertension is defined as de novo hypertension (≥ 140/90 mmHg) after 20 gestational weeks without proteinuria. Preeclampsia will be diagnosed when gestational hypertension is comorbid with any of the following manifestations: proteinuria (≥ 0.3 g/24 h), renal insufficiency, thrombocytopenia (platelets ≤ 100,000 × 109/L), impaired liver function or pulmonary edema [22].
Neonatal outcomes
The birth defect rate is defined as the ratio of birth defects (fetal body structure, functional or metabolic congenital abnormalities) to the number of transplant cycles. Birth weight, infant sex, gestational age at birth, Apgar score, congenital anomalies, shoulder dystocia, bone fracture, neonatal hypoglycemia, bronchial plexus injury, neonatal respiratory distress, neonatal pathological jaundice, neonatal intensive care unit admission, stillbirth (≥ 20 weeks), and neonatal death (within the first 28 days after delivery) will be followed-up and assessed.
Microbiome and metabolism
Alpha and beta diversity analysis will be conducted by QIIME2 software [23]. The taxonomy abundance spectrum will be described and compared between groups using the linear discriminant analysis effect size (LEfSe) method. Metabolic profiles will be analyzed using the Progenesis QI v3.0 software.
Data collection
At the time of enrollment, information about the history of PCOS diagnosis, menstrual cycle demographic characteristics, socioeconomic status, alcohol consumption, smoking habit, self-reported morbidity, obstetric history, first-degree family history of hypertension, diabetes, stroke, hyperlipidemia, and obesity will be obtained using a baseline questionnaire. Clinical information on the maternal and neonatal outcomes mentioned above will be collected from outpatient and inpatient electronic records in four centers and will be confirmed by the investigators.
Statistical methods
Sample size calculation
A recent meta-analysis reported an estimated clinical pregnancy rate of 26% in PCOS patients undergoing IVF [24]. Our team has revealed that approximately 30% of PCOS patients have Lactobacillus deficiency (PCOS-LD), which presents as lower levels of Lactobacillus (< 50%) in the vagina [7]. Our unpublished data suggested a clinical pregnancy rate of 17.65% in patients with PCOS-LD, while a clinical pregnancy rate of 41.82% was reported in PCOS patients without Lactobacillus deficiency (PCOS-non-LD). Moreover, our team previously reported a clinical pregnancy rate of 49.69% in patients who underwent IVF due to tubal blockage [25]. To improve the clinical pregnancy rate among infertile PCOS-LD patients to the level of that among PCOS-non-LD patients, or even to the clinical pregnancy rate among patients with tubal blockage, we hypothesized a 20% increase in the clinical pregnancy rate in our RCT. Assuming a clinically important 20% increase in the rate of clinical pregnancy in the intervention arm and allowing for a 15% dropout rate, the calculated sample size of 260 subjects (130 per group) will provide 95% power with a one-tailed alpha error of 0.025. Thus, we aim to recruit 300 women in total (150 per group).
Statistical analysis
Categorical variables will be presented as counts with percentages, e.g., n (%). Normally distributed data will be shown as the means with standard deviations, e.g., means ± SDs, while nonnormally distributed data will be expressed as medians with interquartile ranges, e.g., medians (IQRs). Student’s t test for continuous variables with normal distributions and the nonparametric
Kruskal–Wallis test for nonnormally distributed data will be applied for comparisons of significant differences between the 2 groups. The Pearson chi-square test will be used for categorical data. For binary observational endpoints, risk ratios with 95% confidence intervals will be calculated by binomial regression with and without adjustment for potentially confounding baseline values. In this study, the main analyses will be conducted using an intention-to-treat (ITT) model, in which all participants will be included based on random assignment regardless of study completion. For outcomes collected at different time points, a repeated measurements design using a generalized estimating equation (GEE) model will be used to fit outcomes that are measured at each time point so that all the participants might be included in the analyses, even if there are missing data for some of the follow-up points. A multiple imputation model will be used to process the missing data. Additionally, statistical analyses of the baseline characteristics of participants who remain in the study and those who are lost to follow-up will also be performed to explore whether there is differential dropout. All statistical analyses will be conducted using the SPSS software (version 25.0) and R software (version 4.0.2). A two-sided p value < 0.05 will be considered significant.
Data management and confidentiality
All paper materials will be stored and locked in a designated cabinet, and electronic data will be saved in the password-secured CRIP system. Data input will be executed by a full-time CRC and a supervisor. Incorrectly inputted data will be checked and corrected by the supervisor after confirmation with participants or by checking their clinical records. Any amendment of the original data will be tracked in detail. The personal information of the participants will remain anonymous and be stored securely throughout the study. Any unauthorized access to the CRIP system or disclosure of the database will not be allowed at any trial center. All staff members in this study are responsible for strict confidentiality of information at all times. There are no plans for additional studies using the data that are collected as part of this trial.
Data monitoring and auditing
The trial steering committee is composed of LL, SYL, AJZ, HFH, and JL, who will be responsible for study supervision and overall conduct. A data monitoring committee (DMC) will be set up for on-site audits and quality control. The DMC will be independent from the sponsor with no conflicts of interest. Two audits will be executed: at the midpoint and at the end of the RCT. Emphasis will be placed on whether enrollment, sampling, data collection, intervention, and follow-ups are executed and recorded in a timely manner according to the research protocol. The accuracy of the original data will be verified by randomly selected participants. A formal report will be generated, which will provide valuable instructions for problem-solving in due time and for future statistical analyses. Regarding adverse events (AEs), vaginal use of live Lactobacillus capsules for the treatment of mycosis fungoides and bacterial vaginosis in pregnant women has been reported, and no adverse effects were observed in a small-scale clinical study in China [17,18,19]. However, for the safety of the treatment, during the whole treatment and follow-up procedure, any discomfort or worsening of existing discomfort in patients will be recorded, regardless of whether it is related to the study intervention. Symptoms such as abdominal pain, bloating, chest tightness, and bleeding, physical signs such as positive shifting dullness, adnexa mass, and infection and abnormal medical auxiliary examination results will be recorded. Any unexpected effects might be collected by regular follow-up, participant self-reports, systematic physical examinations performed by doctors, and laboratory results. Any harms will be classified using the Common Terminology Criteria for Adverse Events (CTCAE) Version 5, published on November 27, 2017, by the Department of Health and Human Services, National Institutes of Health, National Cancer Institute, USA. Any unintended appearances of AEs will be reported in a timely manner to the TSC and recorded in detail. All the related AEs will be recorded in case report form and reported in the future published manuscript.
Ethics approval and consent to participate
Ethical review approvals were obtained from four centers: the International Peace Maternity and Child Health Hospital (15 October 2020, GKLW 2020-29), Ruijin Hospital, Shanghai Jiao Tong University, School of Medicine, Shanghai, China (3 December 2020), Zhongshan Hospital, Fudan University, Shanghai, China (20 October 2020, SK2020-169), and the ShangHai JIAI Genetics and IVF Institute (10 October 2020, JIAI E2020-017). All study designs will comply with the principles of the Declaration of Helsinki. All individuals will sign written informed consent forms before participating in the RCT.
Dissemination
Regular meetings will be held for quality control and progress promotion. The completion of this trial and publication of the results will be attributed to all collaborators. The ultimate results of this trial will be reported back to each participant through open access publications. To maximize dissemination, these findings will be reported in open access publications in journals with high impact, and oral and poster presentations concerning the fertility needs of PCOS patients will be performed domestically and internationally.
Discussion
PCOS is one of the most common causes of female infertility. Once pregnant, women with PCOS face an increased risk of adverse perinatal outcomes [5]. Moreover, we previously found significant LGT dysbiosis and an associated lower rate of clinical pregnancy among PCOS patients after IVF-FET (unpublished). Our trial aims to evaluate the effects of transvaginal Lactobacillus supplementation on the health of the LGT microbiome and perinatal outcomes in PCOS patients after IVF-FET, which will be the first large and cross-centered RCT in this territory. If successful, the findings of this study can be applied to clinical practice to better improve the health of PCOS patients and maternal and infant health after IVF-FET.
Nonetheless, several limitations of this trial should be recognized. First, investigators and participants will not be blinded to group allocation, which might introduce bias. Another limitation is that the control arm will still have access to the administration of Lactobacillus, although medical records will be obtained to confirm the group situation.
Trial status
Recruitment began on January 12, 2021. Data collection aims to be completed in July 2024. Date and version identifier: 2020.08.15-version 1.0.
Availability of data and materials
Not applicable.
Abbreviations
- PCOS:
-
Polycystic ovary syndrome
- LGT:
-
Lower genital tract
- IVF-FET:
-
In vitro fertilization–frozen embryo transfer
- GDM:
-
Gestational diabetes mellitus
- RCT:
-
Randomized clinical trial
- RT–qPCR:
-
Real-time quantitative polymerase chain reaction
- CRCs:
-
Clinical research coordinators
- CRIP:
-
Clinical Research Integrated Platform
- ET:
-
Embryo transfer
- HCG:
-
Human chorionic gonadotropin
- P:
-
Progesterone
- LC–MS:
-
Liquid chromatography–mass spectrometry
- LEfSe:
-
Linear discriminant analysis effect size
- SDs:
-
Standard deviations
- IQRs:
-
Interquartile ranges
- TSC:
-
Trial steering committee
- DMC:
-
Data monitoring committee
- AEs:
-
Adverse events
References
Norman RJ, Dewailly D, Legro RS, Hickey TE. Polycystic ovary syndrome. Lancet. 2007;370(9588):685–97.
Wang F, Pan J, Liu Y, Meng Q, Lv P, Qu F, et al. Alternative splicing of the androgen receptor in polycystic ovary syndrome. Proc Natl Acad Sci U S A. 2015;112(15):4743–8.
Conway G, Dewailly D, Diamanti-Kandarakis E, Escobar-Morreale HF, Franks S, Gambineri A, et al. The polycystic ovary syndrome: a position statement from the European Society of Endocrinology. Eur J Endocrinol. 2014;171(4):P1–29.
Anagnostis P, Tarlatzis BC, Kauffman RP. Polycystic ovarian syndrome (PCOS): long-term metabolic consequences. Metab Clin Exp. 2018;86:33–43.
Hoeger KM, Dokras A, Piltonen T. Update on PCOS: consequences, challenges, and guiding treatment. J Clin Endocrinol Metab. 2021;106(3):e1071–e83.
Bahri Khomami M, Joham AE. Increased maternal pregnancy complications in polycystic ovary syndrome appear to be independent of obesity-a systematic review, meta-analysis, and meta-regression. Obes Rev. 2019;20(5):659–74.
Tu Y, Zheng G, Ding G, Wu Y, Xi J, Ge Y, et al. Comparative analysis of lower genital tract microbiome between PCOS and healthy women. Front Physiol. 2020;11:1108.
Wang Z, He Y, Zheng Y. Probiotics for the treatment of bacterial vaginosis: a meta-analysis. Int J Environ Res Public Health. 2019;16(20)
Tomas M, Palmeira-de-Oliveira A, Simoes S, Martinez-de-Oliveira J, Palmeira-de-Oliveira R. Bacterial vaginosis: standard treatments and alternative strategies. Int J Pharm. 2020;587:119659.
Okesene-Gafa KA, Moore AE, Jordan V, McCowan L, Crowther CA. Probiotic treatment for women with gestational diabetes to improve maternal and infant health and well-being. The Cochrane database of systematic reviews, CD012970. 2020;6(6)
Szczuko M, Kikut J, Szczuko U, Szydlowska I, Nawrocka-Rutkowska J, Zietek M, et al. Nutrition strategy and life style in polycystic ovary syndrome-narrative review. Nutrients. 2021;13(7)
Yu Y, Tan P, Zhuang Z, Wang Z, Zhu L, Qiu R, et al. Untargeted metabolomic approach to study the serum metabolites in women with polycystic ovary syndrome. BMC Med Genet. 2021;14(1):206.
Feng T, Liu Y. Microorganisms in the reproductive system and probiotic’s regulatory effects on reproductive health. Computational and structural biotechnology journal. 2022;20:1541–53.
Lindheim L, Bashir M, Munzker J, Trummer C, Zachhuber V, Leber B, et al. Alterations in gut microbiome composition and barrier function are associated with reproductive and metabolic defects in women with polycystic ovary syndrome (PCOS): a pilot study. PLoS One. 2017;12(1):e0168390.
Qi X, Yun C, Sun L, Xia J, Wu Q, Wang Y, et al. Gut microbiota-bile acid-interleukin-22 axis orchestrates polycystic ovary syndrome. Nat Med. 2019;25(8):1225–33.
Pruski P, Correia GDS, Lewis HV, Capuccini K, Inglese P. Direct on-swab metabolic profiling of vaginal microbiome host interactions during pregnancy and preterm birth. Nat Commun. 2021;12(1):5967.
Li Zhang LQ. Clinical observation of the live Lactobacillus capsule for vaginal use for bacterial vaginosis during pregnancy. Chinese Journal of Eugenics and Genetics. 2007;09:77–8.
Xiuhong Sun GS, Jin P. The value of the live Lactobacillus capsule for vaginal use in the treatment of recurrent Candida vaginitis in pregnant women. Strait Pharmacy. 2007;1:69.
Xiang C. The efficacy of the live Lactobacillus capsule for vaginal use in treating 80 cases of bacterial vaginosis during pregnancy. Modern Journal of Integrated Chinese and Western Medicine. 2008;07:1067.
Nossa CW, Oberdorf WE, Yang L, Aas JA, Paster BJ, Desantis TZ, et al. Design of 16S rRNA gene primers for 454 pyrosequencing of the human foregut microbiome. World J Gastroenterol. 2010;16(33):4135–44.
Classification and Diagnosis of Diabetes. Standards of Medical Care in Diabetes-2021. Diabetes Care. 2021;44(Suppl 1):S15–s33.
ACOG Practice Bulletin No. 202: Gestational hypertension and preeclampsia. Obstet Gynecol. 2019;133(1):1.
Bolyen E, Rideout JR. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat Biotechnol. 2019;37(8):852–7.
Showell MG, Mackenzie-Proctor R, Jordan V, Hodgson R, Farquhar C. Inositol for subfertile women with polycystic ovary syndrome. The Cochrane database of systematic reviews. 2018;12(12):Cd012378.
Pan JX, Liu Y, Ke ZH, Zhou CL, Meng Q, Ding GL, et al. Successive and cyclic oral contraceptive pill pretreatment improves IVF/ICSI outcomes of PCOS patients and ameliorates hyperandrogenism and antral follicle excess. Gynecological endocrinology: the official journal of the International Society of Gynecological Endocrinology. 2015;31(4):332–6.
Acknowledgements
We would like to express our sincere appreciation and thanks to the clinical colleagues at each participating center for their strong support and enormous effort during the execution of this clinical trial and to the participants enrolled in this study for their voluntary participation and willingness to cooperate.
Funding
This work was supported by the Clinical Research Plan of Shanghai Hospital Development Center (SHDC, No. SHDC2020CE1008A), the National Key R&D Program of China (2021YFC2700603), the National Natural Science Foundation of China (82088102, 82171613, 82171688 and 81801411), the International Cooperation Project of China and Canada NSFC (No. 81661128010), the Chinese Academy of Medical Sciences Research Unit (No. 2019RU056), and the Collaborative Innovation Program of Shanghai Municipal Health Commission (2020CXJQ01).
None of the funders took part in the study design, management of data, or decision on publication.
Author information
Authors and Affiliations
Contributions
HH, LJ, and YW conceived the study idea and supervised trial processing in each study center. YT, HC, and CZ participated in the study design and data analysis. HC drafted the manuscript, and YT, CZ, YW, LJ, and HH revised the manuscript. SY, AZ, LL, LW, JL, and HH supervised the recruitment and diagnosis in each center, and HC, LH, YL, YS, XC, and JX were in charge of the participant recruitment and data collection. CZ, YT, and HC will perform the data analysis. HC, TW, and JL oversee the laboratory screening. All authors critically reviewed the text and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Ethical review approvals were obtained from four centers: Medical Research Ethics Committees of the International Peace Maternity and Child Health Hospital (15 October 2020, GKLW 2020-29); Ruijin Hospital, Shanghai Jiao Tong University, School of Medicine, Shanghai, China (3 December 2020); Zhongshan Hospital, Fudan University, Shanghai, China (20 October 2020, SK2020-169); and ShangHai JIAI Genetics and IVF Institute (10 October 2020, JIAI E2020-017). All study designs will comply with the principles of the Declaration of Helsinki. All individuals will sign written informed consent forms before participating in the RCT.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
SPIRIT 2013 Checklist: Recommended items to address in a clinical trial protocol and related document.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, H., Tu, Y., Zhang, C. et al. Effect of transvaginal Lactobacillus supplementation on reversing lower genital tract dysbiosis and improving perinatal outcomes in PCOS patients after IVF-FET: a study protocol for a multicenter randomized controlled trial. Trials 24, 821 (2023). https://doi.org/10.1186/s13063-023-07825-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s13063-023-07825-9