
Abstract
Background
Plasmodium vivax malaria is considered a major threat to malaria eradication. The radical cure for P. vivax malaria normally requires a 14-day administration of primaquine (PQ) to clear hypnozoites. However, maintaining adherence to PQ treatment is a significant challenge, particularly in malaria-endemic rural areas. Hence, this study aimed to formulate interventions for promoting patients’ commitment to PQ treatment in a highly malaria-endemic township in Myanmar.
Methods
A qualitative study was conducted in Waingmaw Township in northern Myanmar, where P. vivax malaria is highly endemic. Key stakeholders including public health officers and community members participated in focus group discussions (FGDs) and in-depth interviews (IDIs) in September 2022. Data were collected using validated guidelines, translated into English, and visualized through thematic analysis.
Results
Responsible individuals from different levels of the Myanmar National Malaria Control Programme participated in the IDIs. Most of them reported being aware of the markedly increasing trend of P. vivax and the possibility of relapse cases, especially among migrants who are lost to follow-up. Workload was a key concern surrounding intervention implementation. The respondents discussed possible interventions, such as implementing directly observed treatment (DOT) by family members, piloting a shorter PQ regimen, expanding the community’s malaria volunteer network, and strengthening health education activities using local languages to promote reasonable drug adherence. FGDs among community members revealed that although people were knowledgeable about malaria symptoms, places to seek treatment, and the use of bed nets to prevent mosquito bites, most of them still preferred to be treated by quack doctors and rarely used insecticide-treated nets at worksites. Many often stopped taking the prescribed drugs once the symptoms disappeared. Nevertheless, some respondents requested more bed nets to be distributed and health promotion activities to be conducted.
Conclusion
In rural areas where human resources are limited, interventions such as implementing family member DOT or shortening PQ regimens should be introduced to enhance the radical cure for the P. vivax infection. Disseminating information about the importance of taking the entire treatment course and emphasizing the burden of relapse is also essential.
Similar content being viewed by others


Background
Despite a significant reduction in reported annual malaria cases, statistics from 2021 showed that Myanmar accounted for 88% of the total malaria cases reported in the Greater Mekong Subregion (GMS) [1]. That year, 81.4% of the 79,001 confirmed malaria cases from the country’s 330 townships were caused by Plasmodium vivax infection [1]. Malaria incidence in Myanmar decreased because access to diagnosis and treatment services expanded through basic health staff (BHS) and village health volunteers (VHVs), especially in rural and highly malaria-endemic areas [2, 3]. Currently, P. vivax has become the predominant cause of Plasmodium infection in the country. The radical cure for P. vivax malaria requires a 14-day primaquine (PQ) treatment to eliminate hypnozoites in the human liver [4]. However, patients’ compliance with such a regimen is a major challenge [5, 6]. According to a recent report, approximately 20% of malaria cases presented recurrent or relapse episodes, most of which occurring within 1 year after the initial infection [7]. Because relapse infections can help sustain the infectious parasite reservoir in the community, they are an important impediment to the eradication of malaria [8].
In 2011, the Myanmar National Malaria Control Programme (NMCP) introduced PQ to the National Antimalaria Treatment Policy, which recommended that a 3-day chloroquine together with a 14-day PQ (0.25 mg/kg/day) be given to patients with P. vivax malaria by BHS without glucose 6 phosphate dehydrogenase (G6PD) testing. In areas where health facilities are limited in handling severe hemolysis, another PQ regimen (0.75 mg/kg/week for 8 weeks) should be prescribed by VHVs [9]. In July 2018, to promote treatment adherence, the guidelines were modified to allow VHVs to administer the 14-day PQ (0.25 mg/kg/day) to patients with P. vivax instead of the weekly regimen. Still, the practice of administering the G6PD test to every patient is not yet recommended in Myanmar. Patients undergoing the 14-day PQ treatment are instructed to check their urine color as a sign of haemolysis; if their urine turns black or red, they must stop PQ medication and seek further haemolysis management at the nearest health centre [9].
Because P. vivax transmission is a major threat to malaria eradication in the country, enhancing activities focusing on the radical cure for P. vivax is a top priority under the Myanmar National Strategic Plan for Malaria Elimination (2021–2025) [10]. Under the current intervention program, adherence to the 14-day PQ regimen is estimated to be low. A study conducted in late 2015 found that only 46% of patients treated by VHVs complied with PQ treatment [11]. This highlights a need for new approaches to improve adherence; however, to be considered effective, new interventions require several considerations, including financial and human resources, community acceptance and participation, and social and local beliefs. Effective interventions must obtain inputs from frontline health workers as well as the community, and the challenges that prevent patients from strictly following treatment instructions must be explored and addressed. One study in Myanmar recommended that qualitative studies be conducted on factors that drive patient adherence to PQ [11].
Myanmar is composed of 14 states and regions and 1 union territory. Each locality is different in terms of geographical features, displacement patterns of people, movement of migrants, and malaria situation including vector bionomics. Consequently, disparities in malaria prevalence can be observed across regions. For instance, in 2021, the states of Kachin, Kayin, and Rakhine reported the highest malaria cases in the country. Formulating the most effective intervention to reduce the number of patients in a particular area involves tailoring the intervention to the nature of its location, demographics, and predominant malaria species [12]. Therefore, optimal interventions for each setting must include inputs from frontline health workers and the community. This study aims to examine the various factors that influence P. vivax malaria patients’ compliance with PQ treatment in a township in northern Myanmar. Ultimately, this study’s goal is to create a novel intervention package that can improve adherence among these patients.
Methods
Study design
This qualitative study includes in-depth interviews (IDIs) with healthcare providers from all administrative levels of the NMCP (central, state, township, and village) and focus group discussions (FGDs) with community members to collect their perspectives, views, and inputs regarding P. vivax malaria treatment and treatment adherence.
Study site
This study was conducted in Kachin State in northern Myanmar, which has a population of 1.7 million. Kachin State accounted for 36% of the nationwide reported P. vivax cases in 2020. Of the total malaria cases reported in this state, more than 90% were caused by P. vivax. Malaria infection is present throughout the year but peaks in May–August.
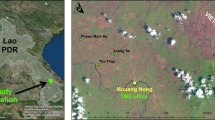
Waingmaw Township, located near the China–Myanmar border (Fig. 1), was purposively selected as the study site for having the highest incidence of P. vivax among the 18 townships of Kachin State. In 2020, Waingmaw Township had a total of 197 trained VHVs serving a population of approximately 100,000 across its 213 malaria-endemic villages [13]. One-third of the township is covered by forest vegetation with an average annual rainfall of 98 cm. Its annual parasite incidence was 30 per 1000 population in 2021, of which 99.4% is attributed to P. vivax (Fig. 2). The township reported 5242 and 7953 P. vivax cases in 2020 and 2021, respectively. In addition, three villages were purposively selected for the FGDs based on their high P. vivax burden and accessibility (security reasons).

Map of the study township in northern Myanmar

Malaria species composition in Waingmaw Township (2015–2021)
Study population and samples
The study population included malaria programme staff from all levels of administration, residents from ethnic majority and minority groups in selected villages, mobile and migrant populations working as seasonal agricultural labourers, and forest-related workers.
To explore the perceptions of different stakeholders regarding the challenges to malaria treatment and its adherence, 10 IDIs were held at the central, state, township, and village levels (Fig. 3). Eligible participants included males or females aged more than 18 years, with more than 1 year of experience in malaria prevention and control activities in their current positions.

Myanmar’s malaria control programme lineup from the village to the central levels
Also, four FGDs were conducted among community members to explore their overall malaria knowledge, perceptions, preventive practices, and suggestions for further activities in the malaria programme. One FGD was held in each village except for one large village that required two FGDs. A total of six community members were invited to participate in each FGD. These community members included males and females in different occupations to capture different views, but the FGDs prioritized community members who have resided in the selected villages for at least 2 years and have contracted malaria at least once in the last 2 years. Village administrative personnel, religious leaders, or older villagers who could lead the discussion and whose voice may overpower others were excluded.
Data collection
Guidelines for both IDIs and FGDs were developed in English based on the literature [14] and other relevant studies [11, 15]. These guidelines were translated into Burmese with the help of two malaria experts from the NMCP through backtranslation. Two guidelines were written separately for healthcare providers and community members. For the IDIs, semi-structured interviews were conducted to explore healthcare providers’ operational challenges, barriers, and difficulties in implementing the National Malaria Treatment Guidelines. Meanwhile, the FGDs explored the community members’ knowledge of malaria, their perception of its susceptibility and severity, the benefits of and barriers to PQ treatment, and access to information on anti-malarial medications and treatment adherence.
Three data collection assistants from NMCP were voluntarily recruited. One day before data collection, the lead researcher conducted orientation sessions on data collection procedures, ethical standards, and the recording of responses. An IDI lasted 20 min while a FGD took 1 h. Audio recordings and handwritten notes were taken during the interviews. The IDIs and FGDs were held in secure locations, such as offices or private rooms. Informed consent was obtained before the interviews.
Data analysis
Qualitative data from both IDIs and FGDs were independently translated into English by KMW and PLA and simultaneously transcribed in verbatim. The translations were cross-checked for accuracy by SL and ZR. The findings underwent deductive and inductive thematic analysis, and the constructed themes were shared with all authors and amended accordingly. All authors agreed on the finalized themes. Qualitative data analysis was performed with the help of NVivo version 12.
Ethical consideration
The study protocol was reviewed and approved by the institutional review boards of the University of Public Health, Yangon, Myanmar (UPH-IRB: 2022/Research/6), and the Ethics Committee for Human Research Study, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand (MUTM 2022-064-01). The respondents were informed about the study and signed informed consent forms before participating in the interviews or discussions.
Results
Participant demographics
The IDIs were conducted with 10 focal persons (3 females and 7 males) representing the different levels of the malaria programme. This respondent group had a mean age of 46.7 years (SD 8.7 years). Their working experience in malaria programme ranged from 5 to 20 years. Two designated NMCP focal persons from the central level were responsible for various aspects, including programme management, monitoring and evaluation, logistic management, and supervision. Two respondents from the Vector-Borne Disease Control Unit, representing the State Public Health Department, were accountable for the prevention and control of all vector-borne diseases in their state. Six public health officers at the township and village levels served as key management personnel responsible for overseeing all diseases in their respective areas.
Additionally, 4 FGDs were conducted with 24 community members (8 females, 16 males) from 3 malaria-endemic villages in Waingmaw Township. These respondents had a mean age of 34 years (SD 9.8 years). More than half of the respondents (63%) were engaged in forest-related work, such as in banana plantations; 16% were employed in their villages; and 20% were dependents or housewives.
Qualitative findings
Three themes emerged reflecting the importance of the malaria burden and the challenges faced by the current anti-malarial treatment as well as recommendations to improve the malaria control programme.
Theme I: The overall malaria situation
Both health care providers and community members agreed on malaria burden in their area, moreover health care providers expressed the increasing trend of P. vivax. In FGDs, the community members shared their experiences with malaria, with the majority having a history of malaria themselves or in their families within the past two years. They were aware that malaria is caused by mosquito bites and that its cardinal symptom is fever with chill and rigors. However, some respondents chose quick relief by consulting illegal practitioners such as quack doctors. Most community members regularly used bed nets at night except in hot weather and during travel. In recent years, the distributed nets had become large and unusable in the forest. Many people also use the old nets while preserving the newly distributed ones for guests.
We could not use a net when we traveled as the recently distributed nets were family size which takes too much space. Therefore, we could not use a net if it’s unavailable. (29-year-old male)
In IDIs, all participants from different levels of the malaria programme acknowledged a significant decline in malaria prevalence throughout the country due to the expanded implementation of intensive malaria prevention and control activities by various funding agencies. Central level healthcare officials emphasized the emerging trend of malaria cases reported in specific townships, which may be influenced by both the influx of the population due to the ongoing economic crisis and changes in environmental factors favouring vector proliferation. While malaria cases had predominantly involved migrant workers, in 2021, Kachin State reported a substantial number of locally transmitted cases, particularly affecting younger age groups. While migrant populations have been traditionally associated with malaria cases in the study area, the township has seen a recent emergence of indigenous malaria cases.
Implementing partners such as NGO and INGO are working with state VBDC [vector-borne disease control] for malaria prevention and control activities. (Malaria focal person, State Health Department)
Myanmar has witnessed a notable shift in the distribution of Plasmodium species causing malaria. In Kachin State, Plasmodium falciparum was historically the dominant species responsible for malaria infections. Recently, however, there has been a steady prevalence of P. vivax malaria cases, and at present, nearly all malaria cases in the region are caused by P. vivax infections.
In this area, P. vivax cases are increasing beginning from 2019 as reported by rural health centers, subcenters, and volunteers. Many patients with P. vivax came back from the banana plantation field. Still, we found malaria among local people and children too. (Malaria focal person, township public health department)
Theme II: Issues and challenges encountered during anti-malaria treatment
Four sub-themes related to the treatment adherence issues emerged from FGDs among community members and IDIs among health care providers.
Challenges to patient adherence and compliance
Poor treatment adherence among patients with P. vivax malaria was another issue to be prioritized. Typically, healthcare providers would administer the complete drug regimen all at once to every malaria patient. However, they were unsure of the patients’ full treatment compliance, especially for a 14-day PQ course. Some might forget to take the drugs or lose them during the treatment course, especially when their symptoms (e.g., fever) disappear after two to three days of CQ treatment. Other patients had a history of malaria and incomplete treatment two to three months before the current infection.
We observed that some old patients contracted malaria again after two to three months after the first-time treatment. They have always reported not completing the full drug course in the last treatment. As the area constituted many migrants, a few patients disappeared after the treatment and never reappeared. (VHV)
The community members discussed the historical and current symptoms of malaria, highlighting a shift from severe to mild in FGD. They shared experiences of caring for family members with the disease and noted recurring episodes despite completely taking the drugs prescribed by healthcare professionals. Some participants stopped treatment once their symptoms improved, while others experienced worse symptoms and required hospital referral after oral treatment. One case involved a pregnant woman who had an abortion after taking malaria medication, which led some individuals to become reluctant in taking anti-malarial drugs because of concerns about side effects and prolonged usage.
We have to take the drugs for many days to overcome malaria infection. However, as I am afraid of drug side effects, most of the time, I took paracetamol to relieve fever. It worked for me well. (40-year-old male)
Insufficient health literacy initiatives
One health care provider emphasized the importance of updated treatment guidelines among all health providers in effectively managing malaria infections and ensuring radical cure. Following current guidelines is deemed crucial for the treatment of every malaria patient. Additionally, the health care provider respondents highlighted the limitations faced by those who conduct malaria control activities during the COVID-19 pandemic. Onsite activities including state-level coordination meetings with implementation partners, malaria volunteer trainings, refresher courses, and health education sessions were prohibited because of social distancing measures.
We do not implement regular follow-up schemes for patients with malaria. During COVID-19 pandemic era, we could not organize any malaria health education activity either one by one or in a group because we are all busy with urgent activities like COVID-19 vaccination. Still, we regularly distributed the LLINs [long-lasting insecticide-treated nets] to every malaria-confirmed patient. (Female BHS, rural health centre)
Inadequate supply chain management
Most health care provider respondents highlighted the need for an effective supply chain for the distribution of malaria commodities, particularly rapid diagnostic kits and anti-malarial medicines, in response to the increasing number of malaria cases in recent years. They noted that they could not distinguish relapse cases using the current diagnostic tools.
Human resource shortages and constraints
Township-level healthcare officers stated that they usually prescribed complete drugs on a one-time basis without comprehensively communicating the importance of treatment adherence because of time limitations amid workloads. They would usually perform microscopy examinations on hospital-admitted patients and outpatients. Although the township hospital has a malaria microscopy facility, its technician could not cross-check every patient who has undergone a rapid diagnostic test unless a healthcare officer was specially requested. Moreover, because of resource constraints, conducting long-term follow-ups for all malaria cases to identify potential new infections or relapses is not feasible.
There is no regular follow-up system and detection of relapse in the current malaria surveillance system. Due to political insecurity, supervision of patients can’t be done either. (Malaria focal person, State Public Health Department)
Theme III: Suggestions to improve anti-malarial drug adherence among patients with P. vivax
Four sub-themes related to the suggestion to improve anti-malarial drug adherence emerged from FGD among community members and IDI among health care providers.
Behavioural change communication
Community members participated in FGD reported having limited health knowledge, having attained only primary education. Therefore, they preferred to engage in more health education sessions along with the distribution of other malaria-preventive materials such as long-lasting insecticide treated nets. Several respondents also stated that because malaria control activities primarily relied on healthcare professionals and malaria projects, community members planned to simply follow the instructions accordingly. Overall, they are ambivalent about offering suggestions for the programme but remain willing to help healthcare working groups as required.
I had a chance to attend only Grade-5 class, and I do not exactly know malaria-related facts on how to prevent or treat the disease. Therefore, I will be grateful if healthcare providers come to our villages and organize frequent health education sessions. (46-year-old male)
Village-level healthcare providers concluded that increasing the community’s health awareness of taking a complete treatment course is critical to improving treatment compliance. When prescribing anti-malarial medicines, delivering health education using the local language might be effective. The participants proposed an intervention in which health messages are disseminated through sessions organized at religious buildings such as churches or monasteries. They also stated that many villagers preferred receiving health messages through posters and pamphlets including simple facts and fancy pictures or cartoons. If possible, these materials should include contents in the local language.
We should strengthen the community’s knowledge of malaria treatment so that they would strictly follow our instructions. It would be good if we could conduct health education sessions at churches using pamphlets and posters. (Male VHV)
Supervised treatment
Most health care provider respondents expressed concern regarding malaria patients’ suboptimal treatment adherence, particularly in cases where long-duration treatment regimens were prescribed. To address this issue, they suggested DOT as a potential solution to improve patient compliance. However, resource constraints such as staffing shortages, budget limitations, and logistical challenges, particularly in rural areas with a high malaria burden, affect the feasibility of intensive DOT implementation by healthcare personnel. Consequently, the respondents proposed a reliable and cost-effective alternative in which DOT is administered by the family members of malaria patients. They emphasized the importance of locally adapting such interventions to individual needs. Furthermore, considering the limited accessibility of mobile phone networks in certain areas, relying solely on follow-up calls for medication reminders was deemed impractical.
The immediate treatment by a family member may be viable as we applied for organizing mass drug administration activities in the filariasis program. (Malaria focal person, NMCP)
We can do some activities such as family member’s DOT and telephone reminder calls or text messages to improve treatment adherence. (Malaria focal person, township public health department)
Shortening of treatment
Although patients with P. vivax usually present minor symptoms, the health care providers felt that eradicating liver-stage parasites is complicated and requires close supervision. Thus, shortening the current 14-day treatment for P. vivax malaria would be a good alternative. The safety concerns related to the shorter treatment options did not emerge as a prominent issue.
Shortening the days of primaquine treatment and giving more health education for strengthening the radical cure of P. vivax should be implemented. Moreover, volunteer training should be organized to improve their perception of treatment adherence. (Female, State Health Department, Kachin State)
Refresher trainings for volunteers
Because of malaria volunteers’ insufficient provision of detailed information on the importance of drug adherence, their understanding of the potential detrimental consequences of incomplete treatment must be strengthened. Refreshing their knowledge is crucial as it would help them effectively disseminate their acquired knowledge to the wider community and malaria patients.
Trainings to volunteers should be organized to improve their perception toward treatment adherence. (Malaria focal person, State Health Department)
Discussion
This study was conducted in a township that is currently a long way from achieving the malaria elimination indicator. The majority of malaria infections were due to P. vivax. Relapse and the reactivation of latent hypnozoites have been recognized as the main contributors to the persistence of P. vivax transmission [16]. The radical cure of P. vivax requires a 14-day PQ treatment. Several interventions have been proposed to improve treatment compliance [17,18,19,20]. However, each intervention can vary in effectiveness across areas because of the baseline culture, beliefs, and logistical limitations. Specific interventions should be tailored to increase the chance of successful implementation. This study presented stakeholders’ opinions toward the P. vivax malaria burden, challenges and limitations of treatment intervention, and alternative measures to increase adherence to the 14-day PQ treatment.
In this relatively high-malaria-endemic area, the respondents were aware of the disease but still chose to consult illegal medical practitioners such as quack doctors as their first choice because of their perceptions of mild symptoms or familiarity with the disease. This aligns with findings from a study in Lao PDR, where people in highly malarious areas had low perceptions of malaria [21]. In certain areas of Myanmar with no government health centers, quack doctors remain popular and continue to provide healthcare services [22]. Once symptoms such as fever subside, patients with malaria frequently discontinue their prescribed medications. This finding is consistent with a study conducted in Sri Lanka, where a majority of malaria patients were hesitant to continue medication once they felt better [23]. The FGDs revealed that the respondents preferred to receive health education from healthcare providers. In addition, the community promptly participated in health activities led by healthcare providers. Therefore, healthcare providers or malaria volunteers should routinely provide patients infected with P. vivax with detailed prescriptions of medicines and health messages regarding the importance of completing their treatment courses.
Ensuring standardized and timely treatment for every confirmed malaria patient is essential for speedy recovery and to prevent complications [24]. However, low literacy surrounding P. vivax treatment was the main concern among the healthcare providers participating in this study. Some studies in Myanmar have raised a similar concern about the performance of VHVs [25,26,27]. Malaria treatment providers, including BHS and VHVs, should be well-prepared to deliver high-quality treatment according to the National Malaria Treatment Guidelines [3]. Therefore, regular refresher sessions on malaria diagnosis and case management, along with field site monitoring visits, are necessary. Adequate stocks of malaria commodities should be maintained through strategic procurement planning.
Research has shown that DOT is an effective intervention to ensure treatment compliance in many diseases including malaria [17]. Considering the relatively high number of reported P. vivax cases in the study township, it would be impossible for healthcare providers or VHVs to deliver DOT because of increased workloads and limited human resources. The existing local malaria workforce has highlighted that the DOT strategy is infeasible for malaria treatment unless the incidence of the disease is reduced [28]. A study has shown that sending reminder text messages directly to patients could be an efficient alternative to DOT [29]. However, the limited access to a reliable telecommunication infrastructure, particularly in remote villages with active malaria transmission, poses a challenge for malaria healthcare providers in implementing this approach.
In the study township, the respondents reported an influx of workers migrating to and from worksites including banana plantation fields. Therefore, an alternative measure would involve allocating more malaria volunteers to these worksites to perform follow-up checks with patients who completely take the prescribed drugs. However, its success depends on the number of confirmed patients with malaria and population displacements that result in loss to follow-up [15]. The performance of health volunteers is sometimes associated with the incentive they receive for surviving [3]. An attractive incentive scheme should be based on the magnitude of workloads.
Many patients with P. vivax came from worksites with poor road conditions. Delivering health education to patients and their companions to ensure regular and thorough drug intake has been proven to effectively improve adherence, as demonstrated in the Thailand–Myanmar border area [28]. However, Myanmar consists of numerous ethnic groups and minorities, with Burmese being the major language spoken across the country. Because of language barriers, delivering health messages solely in Burmese may not reach all individuals. As suggested by most respondents, it is important to produce information, education, and communication materials in dual-language formats and involve locals who can communicate health facts in regional dialects during health education sessions. One study recommended using local languages to ensure the effective and efficient dissemination of health-related messages [30].
The current respondents also suggested shortening the course of radical treatment. A multicenter study documented the acceptable efficacy of implementing a seven-day PQ treatment compared with a two-week regimen in reducing P. vivax malaria relapse [18]. The adoption of a shortened treatment regimen depends on the availability of reliable G6PD testing before treatment can be administered. However, G6PD testing is not currently being practiced in Myanmar [31]. NMCP may consider piloting this in the study township based on further feasibility assessment of the area and technical support from other organizations, such as the World Health Organization. The participants did not express significant worries or reservations regarding safety. This observation aligns with similar findings reported in the literature, where shorter treatment regimens have been associated with a favourable safety profile in patients with normal G6PD [32].
This study has several strengths and limitations. Because it is the first comprehensive qualitative study that involves malaria stakeholders from all levels of the malaria control programme in Myanmar, its findings are valuable and representative. The selected township represents the socio-behavioural conditions of areas where P. vivax malaria elimination is challenging. The present findings can be applied to other areas with similar conditions. FGDs were conducted to identify challenges and community needs regarding drug treatment compliance. These results can serve as a reference for new interventions in the National Malaria Strategic Plan. However, this study was conducted in areas where political conflict situations have less impact. The suggested interventions in this study should therefore be adjusted when they are implemented in other high-endemic areas. In this study, some healthcare providers discussed the feasibility of a shorter PQ regimen as a means to enhance drug compliance. The primary aim of the present study was to propose potential interventions. Consequently, to facilitate the practical implementation of these suggested interventions in real-world settings, it is imperative to further verify the safety of the treatment, assess technical and operational feasibility, prior to embarking on comprehensive implementation.
Conclusions
Given the emerging trend of P. vivax incidence in Myanmar, facilitating patients’ compliance with PQ treatment may facilitate the country’s path toward malaria elimination by 2030. This study provided insights into the challenges to treatment adherence and recommendations for improving it. Interventions include delivering DOT by family members, piloting a shorter PQ regimen, recruiting worksite malaria volunteers in refugee camps or plantation sites, and increasing health education activities specifically to disseminate information on the issue of incomplete or partial treatment among migrants. When possible, health promotion activities must be delivered in local dialects and standardized pamphlets to strengthen the use of long-lasting insecticide-treated nets and drug adherence. Meanwhile, to reduce the malaria caseloads in this township, maintaining a decent surveillance system is essential to promptly detect malaria cases. In addition, each malaria case must receive standard treatment provided by skilled health workers including VHVs. A constant procurement and supply chain system for distributing malaria commodities should also be in place.
Availability of data and materials
All the data analyzed in this study are already included in the article.
Abbreviations
- BHS:
-
Basic health staff
- DOT:
-
Directly observed treatment
- FGD:
-
Focus group discussion
- G6PD:
-
Glucose 6 phosphate dehydrogenase
- GMS:
-
Greater Mekong Subregion
- IDI:
-
In-depth interview
- PQ:
-
Primaquine
- VBDC:
-
Vector-borne disease control
- VHV:
-
Village health volunteer
References
WHO. World Malaria Report 2022. Geneva: World Health Organization; 2022.
Landier J, Parker DM, Thu AM, Lwin KM, Delmas G, Nosten FH, et al. Effect of generalised access to early diagnosis and treatment and targeted mass drug administration on Plasmodium falciparum malaria in Eastern Myanmar: an observational study of a regional elimination programme. Lancet. 2018;391:1916–26.
Linn NYY, Kathirvel S, Das M, Thapa B, Rahman MM, Maung TM, et al. Are village health volunteers as good as basic health staffs in providing malaria care? A country wide analysis from Myanmar, 2015. Malar J. 2018;17:242.
Popovici J, Tebben K, Witkowski B, Serre D. Primaquine for Plasmodium vivax radical cure: what we do not know and why it matters. Int J Parasitol Drugs Drug Resist. 2021;15:36–42.
Khantikul N, Butraporn P, Kim HS, Leemingsawat S, Tempongko MA, Suwonkerd W. Adherence to antimalarial drug therapy among vivax malaria patients in northern Thailand. J Health Popul Nutr. 2009;27:4–13.
Rahmalia A, Poespoprodjo JR, Landuwulang CUR, Ronse M, Kenangalem E, Burdam FH, et al. Adherence to 14-day radical cure for Plasmodium vivax malaria in Papua, Indonesia: a mixed-methods study. Malar J. 2023;22:162.
White NJ. Determinants of relapse periodicity in Plasmodium vivax malaria. Malar J. 2011;10:297.
Roy M, Bouma MJ, Ionides EL, Dhiman RC, Pascual M. The potential elimination of Plasmodium vivax malaria by relapse treatment: insights from a transmission model and surveillance data from NW India. PLoS Negl Trop Dis. 2013;7: e1979.
National Malaria Control Programme. Guidelines for malaria diagnosis and treatment in Myanmar. Department of Public Health, Ministry of Health and Sport, Republic of the Union of Myanmar. 2015
Myanmar National Malaria Control Programme. National Strategic Plan for Malaria Elimination 2021–2025. Nay Pyi Taw: The Republic of the Union of Myanmar; 2020.
Lwin MK, Ya KZ, Mon SY, Lu SSML, Soe WH, Thi A. Adherence to primaquine treatment in six States and Regions in Myanmar. International congress for Tropical medicine and malaria 18–22 September, Australia 2016. p. 1184.
WHO. A Framework for malaria elimination. Geneva: World Health Organization; 2017.
Department of Population. Thematic Report on Population Dynamics. Myanmar Department of Population, Ministry of Labour, Immigration and Population; 2016.
Grietens KP, Soto V, Erhart A, Ribera JM, Toomer E, Tenorio A, et al. Adherence to 7-day primaquine treatment for the radical cure of P. vivax in the Peruvian Amazon. Am J Trop Med Hyg. 2010;82:1017–23.
Win AYN, Maung TM, Wai KT, Oo T, Thi A, Tipmontree R, et al. Understanding malaria treatment-seeking preferences within the public sector amongst mobile/migrant workers in a malaria elimination scenario: a mixed-methods study. Malar J. 2017;16:462.
Chu CS, White NJ. Management of relapsing Plasmodium vivax malaria. Expert Rev Anti Infect Ther. 2016;14:885–900.
Rahi M, Sirohi PR, Sharma A. Supervised administration of primaquine may enhance adherence to radical cure for P. vivax malaria in India. Lancet Reg Health Southeast Asia. 2023;13: 100199.
Taylor WRJ, Thriemer K, von Seidlein L, Yuentrakul P, Assawariyathipat T, Assefa A, et al. Short-course primaquine for the radical cure of Plasmodium vivax malaria: a multicentre, randomised, placebo-controlled non-inferiority trial. Lancet. 2019;394:929–38.
Llanos-Cuentas A, Lacerda MVG, Hien TT, Velez ID, Namaik-Larp C, Chu CS, et al. Tafenoquine versus primaquine to prevent relapse of Plasmodium vivax mMalaria. N Engl J Med. 2019;380:229–41.
Poespoprodjo JR, Burdam FH, Candrawati F, Ley B, Meagher N, Kenangalem E, et al. Supervised versus unsupervised primaquine radical cure for the treatment of falciparum and vivax malaria in Papua, Indonesia: a cluster-randomised, controlled, open-label superiority trial. Lancet Infect Dis. 2022;22:367–76.
Vilay P, Nonaka D, Senamonty P, Lao M, Iwagami M, Kobayashi J, et al. Malaria prevalence, knowledge, perception, preventive and treatment behavior among military in Champasak and Attapeu provinces, Lao PDR: a mixed methods study. Trop Med Health. 2019;47:11.
Aung T, Lwin MM, Sudhinaraset M, Wei C. Rural and urban disparities in health-seeking for fever in Myanmar: findings from a probability-based household survey. Malar J. 2016;15:386.
Reilley B, Abeyasinghe R, Pakianathar MV. Barriers to prompt and effective treatment of malaria in northern Sri Lanka. Trop Med Int Health. 2002;7:744–9.
Chu CS, White NJ. The prevention and treatment of Plasmodium vivax malaria. PLoS Med. 2021;18: e1003561.
Linn NYY, Tripathy JP, Maung TM, Saw KK, Maw LYW, Thapa B, et al. How are the village health volunteers deliver malaria testing and treatment services and what are the challenges they are facing? A mixed methods study in Myanmar. Trop Med Health. 2018;46:28.
Thiha Y, Zin T, Win KM, Soe MT, Aung PL. Performance of malaria volunteers regarding malaria control activities in Southeastern Myanmar: a study in the areas under coverage of an ethnic health organization. J Trop Med. 2021;2021:6642260.
Aung PL, Silawan T, Rawiworrakul T, Min M. Perceived role and its enhancing factors among the village health volunteers regarding malaria control in rural myanmar. Indian J Public Health. 2018;62:10–4.
Takeuchi R, Lawpoolsri S, Imwong M, Kobayashi J, Kaewkungwal J, Pukrittayakamee S, et al. Directly-observed therapy (DOT) for the radical 14-day primaquine treatment of Plasmodium vivax malaria on the Thai-Myanmar border. Malar J. 2010;9:308.
Raifman JR, Lanthorn HE, Rokicki S, Fink G. The impact of text message reminders on adherence to antimalarial treatment in northern Ghana: a randomized trial. PLoS ONE. 2014;9: e109032.
Kayode OS, Ibitoye B, Olanrewaju MK. Roles of local languages on effective public healthcare delivery in the Gambia: implications for psychological assessment. Texila Int J Public Health. 2020;8:1–8.
Krudsood S, Tangpukdee N, Wilairatana P, Phophak N, Baird JK, Brittenham GM, et al. High-dose primaquine regimens against relapse of Plasmodium vivax malaria. Am J Trop Med Hyg. 2008;78:736–40.
Durand S, Cabezas C, Lescano AG, Galvez M, Gutierrez S, Arrospide N, et al. Efficacy of three different regimens of primaquine for the prevention of relapses of Plasmodium vivax malaria in the Amazon Basin of Peru. Am J Trop Med Hyg. 2014;91:18–26.
Acknowledgements
We thank the state and township public health department officials and the VBDC team from Waingmaw Township for their cooperation during the study. We also thank all data collection assistants for their commitment to gathering data.
Funding
This research was funded by the National Institute of Allergy and Infectious Diseases, National Institutes of Health, USA (U19AI089672).
Author information
Authors and Affiliations
Contributions
KMW, JS, and SL conceived the design of this study. KMW, ZR, and NYYL facilitated data collection. KMW, PLA, and SL performed analysis and drafted the manuscript. All authors reviewed and revised the manuscript as well as read and approved its final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The institutional review boards of the University of Public Health, Yangon, Myanmar (UPH-IRB: 2022/Research/6) and the Ethics Committee for Human Research Study, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand (MUTM 2022-064-01), reviewed and approved the study protocol. The respondents were informed about the study and signed consent forms before participating in the interviews or group discussions.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Win, K.M., Aung, P.L., Ring, Z. et al. Interventions for promoting patients’ adherence to 14-day primaquine treatment in a highly malaria-endemic township in Myanmar: a qualitative study among key stakeholders. Malar J 22, 302 (2023). https://doi.org/10.1186/s12936-023-04743-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-023-04743-8