
Abstract
Background
The incidence of malaria in Thailand has dramatically declined over the past two decades, and the goal is to eliminate malaria by 2025. Despite significant progress, one of the key challenges to malaria elimination are undetected gametocyte carriers. Human migration adds complexity to the malaria situation, as it not only sustains local transmission but also poses the risk of spreading drug-resistant parasites. Currently, no study has assessed the prevalence of gametocytes across multiple years in Plasmodium falciparum malaria patients in Thailand, and the risk factors for gametocyte carriage have not been fully explored.
Methods
Medical records of all P. falciparum malaria patients admitted from January 1, 2001 to December 31, 2020 at the Hospital for Tropical Diseases, Thailand, were retrospectively examined and a total of 1962 records were included for analysis. Both P. falciparum parasites and gametocytes were diagnosed by microscopy. A regression model was used to evaluate predictors of gametocyte carriage.
Results
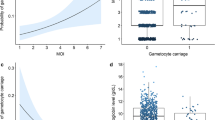
The study demonstrated gametocyte prevalence in low malaria transmission areas. Nine risk factors for gametocyte carriage were identified: age between 15 and 24 years [adjusted odds ratio (aOR) = 1.96, 95% confidence interval (CI) 1.18−3.26], Karen ethnicity (aOR = 2.59, 95% CI 1.56−4.29), preadmission duration of fever > 7 days (aOR = 5.40, 95% CI 3.92−7.41), fever on admission (> 37.5 °C) (aOR = 0.61, 95% CI 0.48−0.77), haemoglobin ≤ 8 g/dL (aOR = 3.32, 95% CI 2.06−5.33), asexual parasite density > 5000−25,000/µL (aOR = 0.71, 95% CI 0.52−0.98), asexual parasite density > 25,000−100,000/µL (aOR = 0.74, 95% CI 0.53−1.03), asexual parasite density > 100,000/µL (aOR = 0.51, 95% CI 0.36−0.72), platelet count ≤ 100,000/µL (aOR = 0.65, 95% CI 0.50−0.85, clinical features of severe malaria (aOR = 2.33, 95% CI 1.76−3.10) and dry season (aOR = 1.41, 95% CI 1.10−1.80). An increasing incidence of imported transnational malaria cases was observed over the past two decades.
Conclusions
This is the first study to determine the prevalence of gametocytes among patients with symptomatic P. falciparum malaria, identify the risk factors for gametocyte carriage, and potential gametocyte carriers in Thailand. Blocking transmission is one of the key strategies for eliminating malaria in these areas. The results might provide important information for targeting gametocyte carriers and improving the allocation of resources for malaria control in Thailand. This study supports the already nationally recommended use of a single dose of primaquine in symptomatic P. falciparum malaria patients to clear gametocytes.
Graphical Abstract

Similar content being viewed by others


Background
The World Health Organization (WHO) has considered Thailand as one of the countries in the Greater Mekong Subregion (GMS) that can potentially eliminate malaria by the year 2025 [1]. While malaria has been successfully eliminated from most provinces in Thailand, transmission persists in the border regions adjacent to Myanmar and Cambodia [2, 3]. Eliminating malaria in these areas presents a significant challenge due to the complex epidemiology of malaria, such as asymptomatic malaria patients [4], multidrug-resistant parasites, population movement, geographically remote areas and political uncertainty in neighbouring countries [5].
Gametocyte carriage has posed a significant challenge to malaria control in Thailand. A recent study found that the gametocyte rate measured by qRT‒PCR was very high (72%) among asymptomatic patients infected with Plasmodium falciparum in communities in western Thailand [4]. As these individuals usually had no symptoms and did not seek medical treatment, they could contribute to sustained malaria transmission [4]. Cross-border movement [6] and international travel [7] have increased the risk of malaria resurgence or importation of malaria cases to malaria-free countries. Sriwichai et al. demonstrated that P. falciparum was mainly imported among Thai-Myanmar immigrants [8], and several studies have reported a higher prevalence of malaria among migrants coming from Myanmar, thus highlighting the importance of border-crossing as a factor in malaria morbidity and mortality in Thailand [9, 10]. Given that the GMS is considered the centre for drug-resistant parasites, population movement may cause the spread of artemisinin-resistant parasites to other countries [11]. In the past, isolated P. falciparum that was resistant to chloroquine and pyrimethamine migrated from the GMS to Africa [11, 12]. Currently, artemisinin-resistant P. falciparum genotypes have been identified in Africa [13, 14].
Gametocytaemia is essential for the onward transmission of malaria infection to mosquitoes, and it does not cause any clinical symptoms. The development of P. falciparum gametocytes occurs over a long period, unlike other Plasmodium species, typically at 7 to 15 days after the initial wave of asexual parasites exit into bloodstream from the liver [15]. Immature gametocytes (stages I–IV) are sequestered in the spleen and bone marrow [16]. Once the gametocytes mature, stage V gametocytes will reappear in blood with an estimated mean circulation time of 4.6–6.5 days [17]. A study in Kenyan children demonstrated the longest duration of gametocyte carriage to be 188 days [18]. In contrast, a study conducted in Thailand showed that the median gametocyte clearance time for uncomplicated P. falciparum malaria was 163 h (with a range of 12–806 h) following the administration of artemisinin-based combination therapy (ACT) [19].
Several risk factors were found to be associated with gametocyte carriage, including age [20,21,22,23,24,25,26,27], gender [28], blood group, sickle cell mutation (HbS) [29], malnutrition [26], duration of illness [28, 30], absence of fever [26, 28, 31], anaemia [26, 30, 32,33,34], thrombocytopenia [26], parasite density [26, 28], malaria severity [32] and multiplicity of infection [31, 35]. However, it is not yet clear what drives asexual stage parasites to progress into the gametocyte stage [16].
Several studies demonstrated that a single or low dose of primaquine effectively reduces malaria transmission by shortening gametocyte circulation time or reducing infectivity of gametocytes to mosquitoes [36,37,38,39,40]. Artemisinin derivatives act on the asexual stage and immature gametocytes, but limited effect against mature gametocytes [41]. On the other hand, primaquine is active against mature gametocytes [42]. Therefore, the WHO now recommends a single low dose of primaquine (0.25 mg/kg) to be added with ACT drugs in cases of acute P. falciparum infection to reduce transmission in low-intensity malaria areas such as in GMS [42]. Likewise, the Thai National Guideline Treatment for Malaria recommends a single dose of primaquine (0.5 mg/kg) or a dosage of 30 mg for individuals weighing more than 50 kg, in order to effectively clear gametocytes [43, 44].
To successfully implement a transmission-blocking strategy, it is necessary to determine the gametocyte burden in Thailand and identify the factors that predict gametocyte carriage. No previous studies have assessed the trend of gametocyte prevalence in this area; in addition, there are a limited number of research studies on gametocyte carriage risk factors. Due to the potential severity and life threatening nature of P, falciparum malaria, the objective of this study was to investigate the gametocyte prevalence among patients with P. falciparum mono-infection in Thailand. The study sought to identify risk factors and describe the epidemiology of gametocyte carriages in this population.
Methods
Study setting and population
The Hospital for Tropical Diseases is a university and tertiary referral hospital located in Bangkok, Thailand. Medical records of P. falciparum patients admitted from January 1, 2001, to December 31, 2020, were retrospectively studied. The study population included adult patients aged 15 years or older who were infected with P. falciparum malaria mono-infection confirmed by microscopy. All patients in the study were symptomatic, which was defined as a history of fever prior to admission. The history of fever was not limited by any specific timeframe. The duration of fever was defined as the duration of pre-admission fever. The definitions remained consistent throughout the study period. The exclusion criteria was a history of anti-malarial medication before admission for the current episode, except for malaria chemoprophylaxis. In addition, medical records with important missing data, such as malaria count charts, were excluded. Demographic data, travel details, and clinical and laboratory data were collected. The authors retrospectively reviewed medical charts and diagnosed severe malaria in accordance with the WHO criteria [45].
Quantification of malaria parasitaemia
Giemsa-stained thick and thin films were prepared from finger-prick blood samples. Thick blood films were examined under a microscope at 100 × magnification, with 10–15 white blood cells per microscopic field considered an indicator of satisfactory thickness. The parasites were counted per 200 white blood cells in the thick film. A minimum of 200 high-power fields had to be examined before declaring the absence of malaria parasites. The number of asexual parasites and gametocytes in 1000 red blood cells was counted in the thin film, and all malaria species and stages were recorded. The parasite and gametocyte density were calculated using actual red blood cell and white blood cell counts from the automated complete blood count result. The asexual parasites and gametocytes were counted every 12 h by WHO-certified microscopists until asexual parasites were absent for three consecutive counts. These quantification methods remained unchanged throughout the study period.
Regarding treatment, severe P. falciparum malaria cases were prescribed parenteral artesunate followed by oral ACTs for three days. Uncomplicated P. falciparum malaria cases received oral ACTs or atovaquone/proguanil. Patients enrolled in drug trials received medications according to the specific trial protocol. However, since this study focuses on analysing asexual parasites and gametocytes on admission prior to the initiation of anti-malarial drugs, the treatment administered will not affect the results. In general, patients were discharged after three consecutive negative tests for asexual parasites and a demonstrated clinical improvement. Patients enrolled in drug trials were hospitalised for 28 days prior to discharge.
Statistical analysis
Gametocyte prevalence was calculated as the proportion of patients with positive gametocytes detected by brightfield microscopy on admission. Border malaria was defined as malaria transmission that took place along land borders, whereas transnational malaria was defined as malaria acquired from a country across an international border and did not involve the border per se [46]. Continuous data were presented as means with standard deviations for normal distribution or medians with interquartile range (IQRs) for non-normal distribution. Asexual parasite and gametocyte densities underwent log10 transformation and were presented as geometric means per µL blood. Categorical data were presented as numbers and percentages. Crude odds ratios (ORs) or Chi-square tests were used to compare proportions as appropriate, while t-tests were used for continuous data. Binary logistic regression was used to evaluate the risk factors associated with gametocyte carriage on admission. Pearson’s correlation coefficient (r) was used to assess the linear correlation between two continuous variables. Data were analysed using SPSS version 23 (IBM Corp. in Armonk, NY). Statistical significance was set at 0.05.
Results
A total of 2341 P. falciparum malaria cases were admitted to the Hospital for Tropical Diseases between 2001 and 2020. Of these, 379 records were excluded due to mixed infection, age less than 15 years old, missing laboratory data or a history of treatment with anti-malaria drugs. Thus, 1962 medical records were included for analysis.
Demographic characteristics
Approximately 80% of patients were male and the median age was 24 years (IQR 20–31) (Table 1). The ethnicity of patients represented a very heterogeneous population that was classified into six groups: Burmese (42.9%), followed by Karen (23.4%), Mon (18.6%), Thai (11.8%), African (1.0%) and others (2.3%). Regarding occupations, 58.8%, 17.3%, 11.0%, 7.6% and 2.6% were manual labourers, unemployed, farmers, employees, and merchants, respectively. No prior history of malaria infection was reported by 50.0% of patients, while 23.5% and 19.5% of patients reported being infected with malaria either once or twice or more, respectively (Table 1). None of the patients had taken malaria chemoprophylaxis.
Characteristics of P. falciparum malaria infection
Of 1962 patients analysed, 1352 (68.9%) had documented fever on admission. The majority of patients (1635/1962, 83.3%) had a fever duration of less than seven days, with a median duration of four days (Table 2) preadmission. There were 632 patients (32.2%) who harboured gametocytes on admission, and 173 (8.8%) showed gametocytes during treatment, which resulted in a total of 805 (41.0%) patients with gametocytes on or during admission. The median number of days to gametocyte emergence was two days (IQR 2–4). The geometric mean asexual parasite density and geometric mean gametocyte density on admission were 19,293/µL and 102/µL, respectively.
Characteristics of P. falciparum malaria infection in cases with gametocytes versus no gametocytes on admission
The patients were divided into two groups upon admission: with gametocytes and without gametocytes. Independent t-test was used to calculate the differences in parasite characteristics between the two groups. Although the continuous data showed non-normal distribution, the sample size was sufficiently large enough for equal variances to be assumed. Two-tailed p values of less than 0.05 were considered statistically significant.
Regarding malaria characteristics between these two groups, three parameters were significantly different (Table 3). Patients with gametocytes on admission had a significantly longer duration of fever (p < 0.001), were more likely to be afebrile on admission (p < 0.001) and had a lower maximum geometric mean asexual parasite density during admission (p = 0.045).
Number of P. falciparum malaria cases and gametocyte prevalence
There was a marked decline in the number of P. falciparum malaria cases admitted in the hospital. From 2001 to 2012, the gametocyte prevalence recorded at the Hospital for Tropical Diseases, Thailand, ranged from 32 to 52%. Between 2013 and 2020, there was a decreasing trend in gametocyte prevalence (Fig. 1). However, it is important to interpret these numbers with caution due to the small sample size.

Gametocyte prevalence of Plasmodium falciparum malaria admitted to the Hospital for Tropical Diseases, Thailand, between 2001 and 2020
Between 2001 and 2012, the main study population was composed of Burmese, Karen, and Mon patients, whereas after 2012, there were more African patients. Thai patients were presented across the study period (Additional file 1). In the past decade, there was an increasing proportion of imported transnational malaria from Africa admitted to the hospital, from 7% (1/15) in 2013 to 92% (11/12) in 2019 (Additional file 2).
Gametocyte carriage risk factors
To determine risk factors for gametocyte carriage, univariate and multivariable analyses were performed based on the proportion of gametocyte carriage in each analytic group (Table 4). The cut-off p value for univariate analysis was 0.1. The forest plots of univariate and multivariable analyses are shown in Additional files 3 and 4.
Demographic risk factors
Univariate analysis revealed five demographic risk factors for gametocytaemia on admission: age, occupation, ethnicity, body mass index (BMI) and population group. The younger age group of 15–24 years (OR = 2.39, 95% confidence interval (CI) 1.57–3.64, p < 0.001) had higher odds of gametocytaemia compared with the older age groups. Regarding occupation, those who were unemployed had the highest risk of carrying gametocytes compared to other occupations (OR = 1.93, 95% CI 1.27–2.95, p < 0.001). Karen, Mon and Burmese ethnicities demonstrated two to three times higher the odds of gametocytaemia than Thai citizens. Underweight individuals (BMI < 18.5 kg/m2) (OR = 1.24, 95% CI 0.99–1.54, p = 0.06) and immigrants were risk factors for gametocyte carriage on admission.
Although not statistically significant, African ethnicities (OR = 0.25, 95% CI 0.03–1.93), overweight individuals (BMI > 25 kg/m2) (OR = 0.75, 95% CI 0.47−1.10) and travellers (OR = 0.62, 95% CI 0.18−2.18 were associated with a low risk of gametocyte carriage on admission. No significant association was observed between gametocyte carriage and gender.
Clinical, parasitological, and haematological risk factors
Gametocyte carriage was significantly associated with a fever duration > 3 days (OR = 3.06, 95% CI 2.49 − 3.76, p < 0.001), haemoglobin ≤ 8 g/dL (OR = 7.87, 95% CI 5.20−11.92, p < 0.001) and severe malaria (OR = 2.45, 95% CI 1.99−3.01, p < 0.001). However, the correlation between fever duration and gametocyte density was weak, despite a statistically significant p value (Pearson’s correlation coefficient = 0.113, p < 0.004, Additional file 5). In contrast, gametocyte carriage decreased with a history of malaria infection (OR = 0.79, 95% CI 0.62−1.01, p = 0.08), fever on admission (axillary temperature (> 37.5 °C) (OR = 0.67, 95% CI 0.55−0.82, p < 0.001), asexual parasite density > 5000−25,000/µL (OR = 0.79, 95% CI 0.61−1.04), asexual parasite density > 25,000−100,000/µL (OR = 0.74, 95% CI 0.54−0.93), asexual parasite density > 100,000/µL (OR = 0.67, 95% CI 0.51−0.87), and thrombocytopenia (≤ 100,000/µL) (OR = 0.76, 95% CI 0.63−0.93, p = 0.007). There was no significant correlation between gametocyte density and asexual parasite density among different ethnicities (Additional file 6).
Seasonality and cases of imported P. falciparum malaria
In Thailand, the rainy season is between May and October, and the dry season is between September and April [47]. A higher number of P. falciparum malaria cases were observed during the rainy season (Additional file 7). The proportion of patients with positive gametocytes on admission ranged from 25% (33/130 in October) to 41% (49/119 in January and 30/74 in February). Individuals were more likely to develop gametocytes during the dry season (OR = 1.24, 95% CI 1.02−1.52, p = 0.032). The risk of gametocyte carriage was approximately 1.5 times higher in cases of border malaria than cases of indigenous malaria (OR = 1.5, 95% CI 1.24−1.82, p < 0.001) whereas transnational malaria showed a low risk of gametocyte carriage (OR = 0.34, 95% CI 0.13−0.87, p < 0.001).
Multivariable analysis
All factors except gender and population group were included in the multivariable analysis. The reason was that gender showed a non-significant result (p > 0.1) and the population group had collinearity with ethnicity. Multivariable analysis revealed nine factors that had significantly higher risks of carrying gametocytes: (1) age between 15 and 24 years old, (2) being Burmese, Karen or Mon, (3) fever duration > 3 days, (4) afebrile on admission (≤ 37.5 °C), (5) haemoglobin ≤ 8 g/dL, (6) asexual parasite density ≤ 5000/µL (7) platelet count > 100,000/µL (8) clinical features of severe malaria and (9) dry season. There was no statistically significant difference in gametocyte carriage among occupations, BMI, a history of malaria and imported malaria (Table 4).
Discussion
This study aimed to demonstrate the gametocyte prevalence of P. falciparum in Thailand from a 20-year retrospective study and thus identify potential risk factors that enable target malaria carriers. This is the longest retrospective study that demonstrated gametocyte prevalence in Thailand, which is a low-intensity malaria transmission area. The study demonstrated a gametocyte prevalence of 32−52% between 2001 and 2012. A relatively higher gametocyte prevalence was observed in comparison to a study at the Thai-Myanmar border during 2001−2010 (24−40% vs. 3−12%) [48]. Likewise, other earlier studies conducted in Thailand also showed a lower gametocyte prevalence [19, 30, 48]. The observed differences might be due to a longer duration of fever or more severe cases in this study population, as the study site was a malaria referral hospital. Moreover, the study identified a slightly higher gametocyte density compared to Nigerian paediatric patients [49], possibly attributed to the higher malaria endemicity in sub-Saharan Africa. The presence of acquired immunity to malaria [50] might contribute to a decrease in gametocyte density. In contrast, Thailand’s border area is recognized for its unstable and low malaria transmission [51]. Additionally, African patients might be more accustomed to malaria and tend to seek care earlier when they are ill.
Nine independent factors were identified, showing a statistically significant association with gametocytaemia on admission. A younger age group (15–24 years) was an important predictor of gametocyte carriage in the study population. Many studies have associated young age with a higher risk of gametocytaemia [21, 23,24,25,26]. A recent meta-analysis of clinical trials conducted in Asia, Africa and South America involving nearly 50,000 patients, revealed interesting findings regarding the prevalence of gametocytaemia [26]. In Africa, the prevalence of gametocytaemia decreased with age, whereas in Asia, it showed an increasing trend until approximately 20 years of age, followed by a gradual decline thereafter [26]. The lower prevalence of gametocytaemia in adults compared to children can be partly attributed to the consequences of increasing immunity against asexual parasite, as well as the possibility that the immune response directly influence gametocytogenesis [15]. A recent study identified antibodies targeting P. falciparum gametocytes, namely Pfs48/45 and Pfs230 [52]. However, there are limited data available regarding the age-related increase in sexual stage immunity. In contrast, some studies have reported no significant association between age and gametocyte carriage [31, 53]. The differences may be attributed to variations in population profiles and methods used for parasite detection.
Burmese migrants [8, 9] or Karen ethnicity [54] were reported as more likely to be infected with P. falciparum malaria than Thai citizens. This is the first study to demonstrate the association between ethnicity and gametocyte carriage. The odds of gametocytaemia in Karen, Mon, and Burmese individuals were two to three times higher than in Thai citizens. Ethnicity may not be directly associated with gametocyte development but rather related to the ecology and socio-economic structure of these populations. Difficulty in accessing healthcare system, including low-risk perception, language barriers, geographical remoteness, poor logistics and limited health coverage may lead to delayed treatment, placing this subpopulation at risk for developing gametocytes. Thus, to reduce transmission and help contain the spread of artemisinin-resistant P. falciparum malaria, it is imperative to administer a single dose of primaquine as a gametocytocidal drug, particularly to migrants who were identified with higher gametocyte prevalence.
Unemployed status was shown to be a risk factor for gametocytaemia in the univariate analysis but not in the multivariable analysis. Political and economic crises might have driven these individuals to migrate cross-border in search for work [8]. It has been demonstrated that recent migrants were almost four times more likely to be infected with P. falciparum malaria compared with Thai patients, suggesting that most P. falciparum cases were imported [8]. Therefore, border screening, regional collaboration, early case detection and treatment in this mobile group are crucial to prevent imported malaria [55]. Interestingly, forest-related occupations were unexpectedly not identified as a risk factor, but this could be due to the small sample size. Nevertheless, multivariable analysis did not show occupation as a risk factor for gametocyte carriage.
There were discrepancies in outcomes between studies as to whether gender [23, 28, 31], absence of fever [26, 28, 31], and parasite density [26, 28, 32] were risk factors of gametocyte carriage. Consistent with previous findings, this study demonstrated that patients who were afebrile (≤ 37.5 °C) [26, 28], had a long duration of fever > 3 days, had anaemia (haemoglobin ≤ 8 g/dL) and had asexual parasite densities ≤ 5000/μL were predictive of gametocyte carriage [28]. A longer duration of fever was found to be associated with a higher risk of gametocytaemia and an increase in gametocyte density. Therefore, in settings with limited health care facilities, a history of a long duration of fever should prompt timely diagnosis and treatment. It has also been reported that anaemia may reflect a prolonged infection and erythrocyte destruction, as evidence by the red blood cell lysis, dyserythropoiesis and reticulocytosis may trigger gametocytogenesis [56, 57]. A direct correlation between asexual parasite density and gametocyte density has also been demonstrated [31]. However, the finding could not be replicated, and this may be attributed to differences in duration of fever before admission or variations in patients’ clinical severity. Despite this, the study revealed low asexual parasite density (≤ 5000/μL) as a predictive factor of gametocytaemia, which is consistent with the literature [28]. According to Farid et al., gametocytogenesis occurred at a very low parasite density, specifically < 100 parasites per mL [58]. Cases with lower asexual parasite densities were reported as more likely to have gametocytes, suggesting that excessive multiplication compensated for reduced gametocytogenesis [59]. Another explanation may be that patients with low parasitaemia are often asymptomatic or subclinical, leading to a delay in seeking care and the subsequent gametocyte development. The study found that gametocyte carriage was more common in severe cases than in uncomplicated malaria. It is possible that the stressful environment in the host triggers gametocytogenesis, with more asexual forms committed to the sexual stage to increase the chance of parasite survival and onward transmission. Thus, further studies on gametocyte biology are necessary to determine the cause of this finding.
A higher rate of gametocyte carriers in the dry season was demonstrated in this study. Unlike previous findings, there was no association between gametocyte prevalence and seasonality [23, 31, 53]. From an evolutionary perspective, a parasite would not benefit from investing resources in gametocyte development if there were no mosquitoes for onward transmission. However, it has been speculated that parasites might increase their gametocyte conversion rate at the beginning of the transmission season [60]. In Thailand, there was little seasonal variation from year to year between 2001 and 2011 [48]. However, after 2011, marked fluctuations in rainfalls and droughts occurred due to the effects of El Niño and La Niña [61]. Since these factors may have an impact on gametocyte prevalence, further investigation is warranted.
The use of primaquine holds great potential for reducing transmission of P. falciparum malaria in low-transmission settings [42]. Available data suggest that a single low dose of primaquine is safe in glucose-6-phosphate dehydrogenase (G6PD) deficient patients in Southeast Asia [62, 63]. However, the current practice of administering a single dose of primaquine to block transmission in symptomatic P. falciparum cases, as recommended in the Thai malaria treatment guideline, does not address the asymptomatic carriers with gametocytes who do not seek medical care. These carriers, often submicroscopic, pose a hidden threat to malaria elimination. Several studies confirmed the presence of asymptomatic and submicroscopic malaria infections in Thailand [4, 64, 65]. But limited data are available regarding the gametocytes in these individuals and their infectivity to mosquitoes in low-transmission settings [66,67,68]. Further research on gametocytes and malaria transmission, encompassing both symptomatic and asymptomatic cases, is necessary to develop effective strategies for mitigating malaria in this low-endemicity area.
Interestingly, an increasing proportion of imported malaria cases transnationally, mainly from the African region was found. Similar situations have occurred in China, Sri Lanka and Kyrgyzstan, where imported malaria threatened malaria resurgence and reintroduction as these countries approached the elimination phase [69]. Since Thailand is approaching the pre-elimination phase, understanding the epidemiology and situation of gametocyte carriage is crucial. Border malaria is complex and requires integrated intervention with multiple parties at local and national levels between adjacent countries. Moreover, awareness of transnational malaria, especially gametocyte carriers, will be useful in preventing onward transmission and the risk of artemisinin-resistant spread.
Limitations
There were some limitations in the current study. First, the number of P. falciparum malaria cases admitted during the past several years was small due to the majority of cases being treated at the border area and the recent travel restriction from the COVID-19 pandemic. However, the decrease in the number of malaria cases reflected the real-life situation. Second, submicroscopic and asymptomatic malaria cases were not included in the study; thus, the gametocyte prevalence might be underestimated. Nevertheless, microscopy remains the standard diagnostic tool and can be applied in the field studies. Third, detailed data on the timing of past malaria infections could not be obtained due to the nature of retrospective study, so the gametocytes detected on admission could also result from recent infection. Furthermore, the precise geolocation may be obscured from the constant movement of human population. As a result, considering the history of malaria and border malaria as a risk factor for gametocytaemia should be interpreted with caution. Despite these limitations, the advantages of this study include a large sample size with comprehensive data on gametocyte carriage over multiple years.
Conclusion
This study is the first to demonstrate gametocyte prevalence of P. falciparum cases and gametocyte risk factors in Thailand. The results revealed that younger age groups, non-Thai citizens (Burmese, Karen and Mon), afebrile on admission, individuals with a longer duration of fever and those with severe clinical features had at a higher risk of gametocyte carriage. Implementing targeted transmission-blocking interventions in this population might facilitate malaria elimination efforts in Thailand. Additionally, raising awareness of transnational malaria, particularly regarding gametocyte carriers, would be useful in preventing onward transmission and the risk of artemisinin-resistant spread. These findings highlight the need for the bidirectional efforts in malaria control.
Availability of data and materials
Data are available from the corresponding author to all interested researchers upon reasonable request.
Abbreviations
- aOR:
-
Adjusted odds ratio
- CI:
-
Confidence interval
- WHO:
-
World Health Organization
- GMS:
-
Greater Mekong Subregion
- ACT:
-
Artemisinin-based combination therapy
- IQR:
-
Interquartile range
- OR:
-
Odds ratio
- BMI:
-
Body mass index
- G6PD:
-
Glucose-6-phosphate dehydrogenase
References
WHO. Strategy for malaria elimination in the Greater Mekong Subregion : 2015–2030. Regional Office for the Western Pacific; World Health Organization; 2015.
Nguitragool W, Karl S, White M, Koepfli C, Felger I, Singhasivanon P, et al. Highly heterogeneous residual malaria risk in western Thailand. Int J Parasitol. 2019;49:455–62.
Kaewpitoon N, Loyd RA, Kaewpitoon SJ, Rujirakul R. Malaria risk areas in Thailand border. J Med Assoc Thai. 2015;98(Suppl 4):S17-21.
Nguitragool W, Mueller I, Kumpitak C, Saeseu T, Bantuchai S, Yorsaeng R, et al. Very high carriage of gametocytes in asymptomatic low-density Plasmodium falciparum and P. vivax infections in western Thailand. Parasit Vectors. 2017;10:512.
WHO. Approaches for mobile and migrant populations in the context of malaria multi-drug resistance and malaria elimination in the Greater Mekong Subregion. Regional Office for South-East Asia; World Health Organization; 2016). https://apps.who.int/iris/handle/10665/204351. Accessed 27 June 2023.
Wangdi K, Gatton ML, Kelly GC, Clements ACA. Cross-border malaria: a major obstacle for malaria elimination. Adv Parasitol. 2015;89:79–107.
Franco-Paredes C, Santos-Preciado JI. Problem pathogens: prevention of malaria in travellers. Lancet Infect Dis. 2006;6:139–49.
Sriwichai P, Karl S, Samung Y, Kiattibutr K, Sirichaisinthop J, Mueller I, et al. Imported Plasmodium falciparum and locally transmitted Plasmodium vivax: cross-border malaria transmission scenario in northwestern Thailand. Malar J. 2017;16:258.
Kritsiriwuthinan K, Ngrenngarmlert W. Asymptomatic malaria infections among foreign migrant workers in Thailand. Asian Pac J Trop Med. 2011;4:560–3.
Kritsiriwuthinan K, Ngrenngarmlert W. Molecular screening of Plasmodium infections among migrant workers in Thailand. J Vector Borne Dis. 2011;48:214–8.
Mita T, Tanabe K. Evolution of Plasmodium falciparum drug resistance: implications for the development and containment of artemisinin resistance. Jpn J Infect Dis. 2012;65:465–75.
Ecker A, Lehane AM, Clain J, Fidock DA. PfCRT and its role in antimalarial drug resistance. Trends Parasitol. 2012;28:504–14.
Balikagala B, Fukuda N, Ikeda M, Katuro OT, Tachibana S-I, Yamauchi M, et al. Evidence of artemisinin-resistant malaria in Africa. N Engl J Med. 2021;385:1163–71.
Uwimana A, Umulisa N, Venkatesan M, Svigel SS, Zhou Z, Munyaneza T, et al. Association of Plasmodium falciparum kelch13 R561H genotypes with delayed parasite clearance in Rwanda: an open-label, single-arm, multicentre, therapeutic efficacy study. Lancet Infect Dis. 2021;21:1120–8.
Bousema T, Drakeley C. Epidemiology and infectivity of Plasmodium falciparum and Plasmodium vivax gametocytes in relation to malaria control and elimination. Clin Microbiol Rev. 2011;24:377–410.
Usui M, Williamson KC. Stressed out about Plasmodium falciparum gametocytogenesis. Front Cell Infect Microbiol. 2021;11:790067.
Bousema T, Okell L, Shekalaghe S, Griffin JT, Omar S, Sawa P, et al. Revisiting the circulation time of Plasmodium falciparum gametocytes: molecular detection methods to estimate the duration of gametocyte carriage and the effect of gametocytocidal drugs. Malar J. 2010;9:136.
Andagalu B, Mativo J, Kamau E, Ogutu B. Longitudinal study on Plasmodium falciparum gametocyte carriage following artemether-lumefantrine administration in a cohort of children aged 12–47 months living in Western Kenya, a high transmission area. Malar J. 2014;13:265.
Piyaphanee W, Krudsood S, Tangpukdee N, Thanachartwet W, Silachamroon U, Phophak N, et al. Emergence and clearance of gametocytes in uncomplicated Plasmodium falciparum malaria. Am J Trop Med Hyg. 2006;74:432–5.
Coleman RE, Kumpitak C, Ponlawat A, Maneechai N, Phunkitchar V, Rachapaew N, et al. Infectivity of asymptomatic Plasmodium -infected human populations to Anopheles dirus mosquitoes in Western Thailand. J Med Entomol. 2004;41:201–8.
Grange L, Loucoubar C, Telle O, Tall A, Faye J, Sokhna C, et al. Risk Factors for Plasmodium falciparum gametocyte positivity in a longitudinal cohort. PLoS ONE. 2015;10:e0123102.
Muthui MK, Mogeni P, Mwai K, Nyundo C, Macharia A, Williams TN, et al. Gametocyte carriage in an era of changing malaria epidemiology: a 19-year analysis of a malaria longitudinal cohort. Wellcome Open Res. 2019;4:66.
Adomako-Ankomah Y, Chenoweth MS, Tocker AM, Doumbia S, Konate D, Doumbouya M, et al. Host age and Plasmodium falciparum multiclonality are associated with gametocyte prevalence: a 1-year prospective cohort study. Malar J. 2017;16:473.
Koepfli C, Robinson LJ, Rarau P, Salib M, Sambale N, Wampfler R, et al. Blood-stage parasitaemia and age determine Plasmodium falciparum and P. vivax gametocytaemia in Papua New Guinea. PLoS ONE. 2015;10:e0126747.
Akim NI, Kingo T, Drakeley C, Senkoro K, Sauerwein RW, Simon B. Dynamics of P. falciparum gametocytemia in symptomatic patients in an area of intense perennial transmission in Tanzania. Am J Trop Med Hyg. 2000;63:199–203.
WWARN Gametocyte Study Group. Gametocyte carriage in uncomplicated Plasmodium falciparum malaria following treatment with artemisinin combination therapy: a systematic review and meta-analysis of individual patient data. BMC Med. 2016;14:79.
Ouédraogo AL, Bousema T, de Vlas SJ, Cuzin-Ouattara N, Verhave J-P, Drakeley C, et al. The plasticity of Plasmodium falciparum gametocytaemia in relation to age in Burkina Faso. Malar J. 2010;9:281.
Sowunmi A, Fateye BA, Adedeji AA, Fehintola FA, Happi TC. Risk factors for gametocyte carriage in uncomplicated falciparum malaria in children. Parasitol. 2004;129:255–62.
Lawaly YR, Sakuntabhai A, Marrama L, Konate L, Phimpraphi W, Sokhna C, et al. Heritability of the human infectious reservoir of malaria parasites. PLoS ONE. 2010;5:e11358.
White NJ, Chongsuphajaisiddhi T, Nosten F, van Vugt M, Price R, ter Kuile F, et al. Risk factors for gametocyte carriage in uncomplicated falciparum malaria. Am J Trop Med Hyg. 1999;60:1019–23.
Sondo P, Bihoun B, Tahita MC, Derra K, Rouamba T, Nakanabo Diallo S, et al. Plasmodium falciparum gametocyte carriage in symptomatic patients shows significant association with genetically diverse infections, anaemia, and asexual stage density. Malar J. 2021;20:31.
Nacher M, Singhasivanon P, Silachamroon U, Treeprasertsuk S, Tosukhowong T, Vannaphan S, et al. Decreased hemoglobin concentrations, hyperparasitemia, and severe malaria are associated with increased Plasmodium falciparum gametocyte carriage. J Parasitol. 2002;88:97–101.
Essangui E, Eboumbou Moukoko CE, Nguedia N, Tchokwansi M, Banlanjo U, Maloba F, et al. Demographical, hematological and serological risk factors for Plasmodium falciparum gametocyte carriage in a high stable transmission zone in Cameroon. PLoS ONE. 2019;14:e0216133.
Gbotosho GO, Sowunmi A, Okuboyejo TM, Happi CT, Michael OS, Folarin OA, et al. Plasmodium falciparum gametocyte carriage, emergence, clearance and population sex ratios in anaemic and non-anaemic malarious children. Mem Inst Oswaldo Cruz. 2011;106:562–9.
Touray AO, Mobegi VA, Wamunyokoli F, Butungi H, Herren JK. Prevalence of asymptomatic P. falciparum gametocyte carriage among school children in Mbita, Western Kenya and assessment of the association between gametocyte density, multiplicity of infection and mosquito infection prevalence. Wellcome Open Res. 2021;5:259.
Okebe J, Bousema T, Affara M, Di Tanna GL, Dabira E, Gaye A, et al. The gametocytocidal efficacy of different single doses of primaquine with dihydroartemisinin-piperaquine in asymptomatic parasite carriers in The Gambia: a randomized controlled trial. EBioMedicine. 2016;13:348–55.
Gonçalves BP, Tiono AB, Ouédraogo A, Guelbéogo WM, Bradley J, Nebie I, et al. Single low dose primaquine to reduce gametocyte carriage and Plasmodium falciparum transmission after artemether-lumefantrine in children with asymptomatic infection: a randomised, double-blind, placebo-controlled trial. BMC Med. 2016;14:40.
Lin JT, Lon C, Spring MD, Sok S, Chann S, Ittiverakul M, et al. Single dose primaquine to reduce gametocyte carriage and Plasmodium falciparum transmission in Cambodia: an open-label randomized trial. PLoS ONE. 2017;12:e0168702.
Dicko A, Roh ME, Diawara H, Mahamar A, Soumare HM, Lanke K, et al. Efficacy and safety of primaquine and methylene blue for prevention of Plasmodium falciparum transmission in Mali: a phase 2, single-blind, randomised controlled trial. Lancet Infect Dis. 2018;18:627–39.
Mwaiswelo RO, Ngasala B, Msolo D, Kweka E, Mmbando BP, Mårtensson A. A single low dose of primaquine is safe and sufficient to reduce transmission of Plasmodium falciparum gametocytes regardless of cytochrome P450 2D6 enzyme activity in Bagamoyo district, Tanzania. Malar J. 2022;21:84.
White NJ. The role of anti-malarial drugs in eliminating malaria. Malar J. 2008;7:S8.
Policy brief on single-dose primaquine as a gametocytocide in Plasmodium falciparum malaria. https://cdn.who.int/media/docs/default-source/documents/publications/gmp/policy-brief-on-single-dose-primaquine-as-a-gametocytocide-in-plasmodium-falciparum-malaria.pdf?sfvrsn=cab14722_2&download=true. Accessed 27 June 2023.
WHO. Programmatic review of the national malaria programme in Thailand. Regional Office for South-East Asia, World Health Organization, 2016. https://apps.who.int/iris/bitstream/handle/10665/253958/9789290225133-eng.pdf. Accessed 27 June 2023.
Thai National Treatment Guideline. 2021. https://malaria.ddc.moph.go.th/downloadfiles/Malaria_Manual/Guideline_Malaria_Treatment_2564_NTG.pdf. Accessed 27 June 2023.
Global malaria programme, guidelines review committee. WHO Guidelines for malaria. 2023. https://apps.who.int/iris/handle/10665/366432. Accessed 8 August 2023.
WHO. Meeting report of the evidence review group on border malaria. Geneva: World Health Organization; 2018.
Mercado CEG, Lawpoolsri S, Sudathip P, Kaewkungwal J, Khamsiriwatchara A, Pan-ngum W, et al. Spatiotemporal epidemiology, environmental correlates, and demography of malaria in Tak Province, Thailand (2012–2015). Malar J. 2019;18:240.
Carrara VI, Lwin KM, Phyo AP, Ashley E, Wiladphaingern J, Sriprawat K, et al. Malaria burden and artemisinin resistance in the mobile and migrant population on the Thai-Myanmar border, 1999–2011: an observational study. PLoS Med. 2013;10:e1001398.
Oyibo W, Latham V, Oladipo O, Ntadom G, Uhomoibhi P, Ogbulafor N, et al. Malaria parasite density and detailed qualitative microscopy enhances large-scale profiling of infection endemicity in Nigeria. Sci Rep. 2023;13:1599.
Doolan DL, Dobaño C, Baird JK. Acquired immunity to malaria. Clin Microbiol Rev. 2009;22:13–36.
Parker DM, Landier J, Von Seidlein L, Dondorp A, White L, Hanboonkunupakarn B, et al. Limitations of malaria reactive case detection in an area of low and unstable transmission on the Myanmar–Thailand border. Malar J. 2016;15:571.
O’Flaherty K, Chan J-A, Cutts JC, Zaloumis SG, Ashley EA, Phyo AP, et al. Anti-gametocyte antigen humoral immunity and gametocytemia during treatment of uncomplicated falciparum multi-national study. Front Cell Infect Microbiol. 2022;12:804470.
Shekalaghe SA, Teun Bousema J, Kunei KK, Lushino P, Masokoto A, Wolters LR, et al. Submicroscopic Plasmodium falciparum gametocyte carriage is common in an area of low and seasonal transmission in Tanzania: submicroscopic gametocytes at low endemicity. Trop Med Int Health. 2007;12:547–53.
Parker DM, Matthews SA, Yan G, Zhou G, Lee M-C, Sirichaisinthop J, et al. Microgeography and molecular epidemiology of malaria at the Thailand–Myanmar border in the malaria pre-elimination phase. Malar J. 2015;14:198.
Sturrock HJW, Roberts KW, Wegbreit J, Ohrt C, Gosling RD. Tackling imported malaria: an elimination endgame. Am J Trop Med and Hyg. 2015;93:139–44.
Baker DA. Malaria gametocytogenesis. Mol Biochem Parasitol. 2010;172:57–65.
Schneweis S, Maier WA, Seitz HM. Haemolysis of infected erythrocytes ? A trigger for formation of Plasmodium falciparum gametocytes? Parasitol Res. 1991;77:458–60.
Farid R, Dixon MW, Tilley L, McCarthy JS. Initiation of gametocytogenesis at very low parasite density in Plasmodium falciparum infection. J Infect Dis. 2017;215:1167–74.
Nacher M, Silachamroon U, Singhasivanon P, Wilairatana P, Phumratanaprapin W, Fontanet A, et al. Risk factors for Plasmodium vivax gametocyte carriage in Thailand. Am J Trop Med Hyg. 2004;71:693–5.
Babiker HA, Schneider P, Reece SE. Gametocytes: insights gained during a decade of molecular monitoring. Trends Parasitol. 2008;24:525–30.
Thailand Water Situation 2022. https://www.thaiwater.net/uploads/contents/current/YearlyReport2022/rain2.html. Accessed 27 June 2023.
Bancone G, Chowwiwat N, Somsakchaicharoen R, Poodpanya L, Moo PK, Gornsawun G, et al. Single low dose primaquine (0.25 mg/kg) does not cause clinically significant haemolysis in G6PD deficient subjects. PLoS ONE. 2016;11:e0151898.
Dysoley L, Kim S, Lopes S, Khim N, Bjorges S, Top S, et al. The tolerability of single low dose primaquine in glucose-6-phosphate deficient and normal falciparum-infected Cambodians. BMC Infect Dis. 2019;19:250.
Sattabongkot J, Suansomjit C, Nguitragool W, Sirichaisinthop J, Warit S, Tiensuwan M, et al. Prevalence of asymptomatic Plasmodium infections with sub-microscopic parasite densities in the northwestern border of Thailand: a potential threat to malaria elimination. Malar J. 2018;17:329.
Shimizu S, Chotirat S, Dokkulab N, Hongchad I, Khowsroy K, Kiattibutr K, et al. Malaria cross-sectional surveys identified asymptomatic infections of Plasmodium falciparum, Plasmodium vivax and Plasmodium knowlesi in Surat Thani, a southern province of Thailand. J Infect Dis. 2020;96:445–51.
Alemayehu A. Biology and epidemiology of Plasmodium falciparum and Plasmodium vivax gametocyte carriage: implication for malaria control and elimination. Parasite Epidemiol Control. 2023;21:e00295.
Vantaux A, Samreth R, Piv E, Khim N, Kim S, Berne L, et al. Contribution to malaria transmission of symptomatic and asymptomatic parasite carriers in Cambodia. J Infect Dis. 2018;217:1561–8.
Tadesse FG, Slater HC, Chali W, Teelen K, Lanke K, Belachew M, et al. The relative contribution of symptomatic and asymptomatic Plasmodium vivax and Plasmodium falciparum infections to the infectious reservoir in a low-endemic setting in Ethiopia. Clin Infect Dis. 2018;66:1883–91.
Liu Y, Sturrock HJW, Yang H, Gosling RD, Cao J. The challenge of imported malaria to eliminating countries. Lancet Infect Dis. 2017;17:141.
Acknowledgements
The authors thank the staff at the Critical Care Research Unit, Department of Clinical Tropical Medicine, Mahidol University for providing data.
Funding
This work was supported by a grant from the Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand. The funders had no roles in the study design, analysis or writing of the manuscript.
Author information
Authors and Affiliations
Contributions
PL, PW, SK, SL, NT, and WM conceptualised and designed the study. PL collected data. PL, SL and NT analysed the data. PL, PW, and SL interpreted the data. PL drafted the manuscript. PL, PW, SK, SL, NT, WM and WN revised and critically reviewed the manuscript. All authors read and agreed to the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Faculty of Tropical Medicine, Mahidol University, Thailand (MUTM 2022-028-01).
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
: Ethnicity of P. falciparum malaria cases admitted to the Hospital for Tropical Diseases, Thailand, between 2001 and 2020.
Additional file 2
: Malaria contraction sites of P. falciparum malaria cases admitted to the Hospital for Tropical Diseases, Thailand, between 2001 and 2020.
Additional file 3
: Forest plot based on univariate analysis of demographic, clinical, parasitological, haematological, and other risk factors for gametocyte carriage.
Additional file 4
: Forest plot based on multivariable analysis of demographic, clinical, parasitological, haematological, and other risk factors for gametocyte carriage.
Additional file 5
: Scatter plot showing the association between duration of fever and gametocyte density.
Additional file 6
: Scatter plot showing the association between asexual parasite density and gametocyte density stratified by ethnicity.
Additional file 7
: Gametocyte prevalence and total number of P. falciparum malaria cases admitted to the Hospital for Tropical Diseases, Thailand recorded monthly during 2001–2020.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Looareesuwan, P., Krudsood, S., Lawpoolsri, S. et al. Gametocyte prevalence and risk factors of P. falciparum malaria patients admitted at the Hospital for Tropical Diseases, Thailand: a 20-year retrospective study. Malar J 22, 321 (2023). https://doi.org/10.1186/s12936-023-04728-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12936-023-04728-7