
Abstract
Background
Herein, we analyzed the efficacy of main antibiotic therapy regimens in the treatment of healthcare-associated meningitis (HCAM).
Materials/methods
This retrospective cohort study was conducted in 18 tertiary-care academic hospitals Turkey, India, Egypt and Romania. We extracted data and outcomes of all patients with post-neurosurgical meningitis cases fulfilling the study inclusion criteria and treated with empirical therapy between December 2006-September 2018.
Results
Twenty patients in the cefepime + vancomycin-(CV) group, 31 patients in the ceftazidime + vancomycin-(CFV) group, and 119 patients in the meropenem + vancomycin-(MV) group met the inclusion criteria. The MV subgroup had a significantly higher mean Glasgow Coma Score, a higher rate of admission to the intensive care unit within the previous month, and a higher rate of antibiot herapy within the previous month before the meningitis episode (p < 0.05). Microbiological success on Day 3–5, end of treatment (EOT) clinical success (80% vs. 54.8%% vs 57.9%), and overall success (EOT success followed by one-month survival without relapse or reinfection 65% vs. 51.6% vs. 45.3%), EOT all cause mortality (ACM) and day 30 ACM (15% vs. 22.6% vs. 26%) did not differ significantly (p > 0.05) among the three cohorts. No regimen was effective against carbapenem-resistant bacteria, and vancomycin resulted in an EOT clinical success rate of 60.6% in the methicillin-resistant staphylococci or ampicillin-resistant enterococci subgroup (n = 34).
Conclusions
Our study showed no significant difference in terms of clinical success and mortality among the three treatment options. All regimens were ineffective against carbapenem-resistant bacteria. Vancomycin was unsuccessful in approximately 40% of cases involving methicillin-resistant staphylococci or ampicillin-resistant enterococci.
Similar content being viewed by others


Introduction
Despite advances in medicine, neurosurgery, antimicrobial therapy, and critical care, meningitis, specifically nosocomial or healthcare-associated meningitis (HCAM), still poses a significant risk of mortality and morbidity [1,2,3]. Prompt and appropriate treatment is essential in managing HCAM, as inappropriate treatment may lead to undesirable outcomes. In contrast to community-acquired meningitis (CAM), which is mainly caused by pneumococci and meningococci [4], healthcare-associated meningitis (HCAM) is typically caused by Gram-negative bacilli, such as Pseudomonas aeruginosa, Acinetobacter spp., or Enterobacteriaceae, and Gram-positive cocci, such as staphylococci or enterococci [1,2,3, 5,6,7,8,9]. This difference also results in a discrepancy in empirical antibiotic therapy. While the third-generation cephalosporin ± ampicillin and vancomycin or rifampin is recommended for empirical CAM therapy, HCAM empirical treatment is recommended to be a combination of vancomycin with ceftazidime or cefepime or meropenem [1, 2, 5, 7]. However, to our knowledge, there are no published clinical data comparing these empirical treatment regimens in terms of efficacy in HCAM. In this multicenter multinational retrospective cohort study, our main objective was to compare the microbiological and clinical efficacy of the main empirical antibiotic regimens used for HCAM.
Methods
This study was conducted in 15 tertiary-care educational hospitals across nine cities in Turkey, including Izmir, Ankara, İstanbul, Adana, Denizli, Antalya, Diyarbakir, Trabzon, and Mersin, as well as three centers in India, Egypt, and Romania. We extracted data and outcomes from all adult patients (aged 18 or older) with post-neurosurgical meningitis who met the inclusion criteria and were treated with one of the three empirical therapy options. The study period was between December 2006 and September 2018. Demographic, clinical, and laboratory findings (white blood cells, CRP and other findings were on the day empirical antibiotic was started), predisposing factors, as well as information on treatment response and outcomes were obtained retrospectively.
Inclusion criteria were as follows [9, 10]
-
a)
Age ≥ 18–year-old
-
b)
Presence of at least three of the following four clinical/laboratory criteria as meningitis findings:
-
i)
Cerebrospinal fluid (CSF) finding: ≥ 250 leucocytes/mm3
-
ii)
CSF culture positivity (in case of coagulase-negative staphylococci meningitis or culture negative meningitis ≥ 250/mm3 leucocytes was a necessity)
-
iii)
Body temperature > 38° C
-
iv)
At least one of the following clinical findings:; disturbances in consciousness, neck stiffness, nausea or vomiting.
-
i)
-
c)
In case of a neurosurgical operation (except shunt operations) onset of the meningitis findings after at least 72 h of hospitalization and/or meningitis episode during the 30-day period after the neurosurgery and/or meningitis episode during the 90-day period after the shunt operations
Exclusion criteria were as follows
-
a)
Age < 18-year-old
-
b)
In case the patient had > 1 meningitis episodes, only the first episode was included in the study.
-
c)
Meningitis episodes not fulfilling the above criteria.
Cefepime, ceftazidime, and meropenem were administered at a dosage of 2 g every 8 h, while vancomycin was given at a dosage of 500 mg every 6 h.
Cerebrospinal fluid (CSF) samples were obtained via lumbar puncture, percutaneous aspiration of the shunt reservoir, or puncture of the extra ventricular drainage tubing. The samples were routinely centrifuged, and the pellet was Gram-stained. Identification and determination of antimicrobial susceptibility were performed using the VITEK 2 automated system (BioMerieux Inc, Mercy L’etoil, France) or conventional methods. Antibacterial susceptibility tests were evaluated according to the Clinical Laboratory Standards Institute (CLSI) criteria until 2014 and the European Committee on Antimicrobial Susceptibility Testing (EUCAST) after 2015 [11, 12].
Clinical and microbiological success criteria were as follows
Day 3–5 clinical response
Defervescence of fever and improvement of other clinical signs on days 3–5.
Day 3–5 microbiological response
Negative CSF culture with a decrease in leukocyte count on days 3–5.
End of treatment (EOT) clinical success
Absence of any need for modification of empirical treatment, along with concomitant clinical (i.e., defervescence of fever and improvement of other clinical signs) and Tmicrobiological response at the end of the empirical therapy regimen. Discontinuation of one of the combined antibiotics after receiving culture results was not considered a modification, but rather an indication of successful treatment.
All cause mortality (ACM)
This referred to death occurring during the meningitis episode, regardless of the cause.
Day 30 all cause mortality
ACM after 30-days after the start of the empirical meningitis treatment.
Infection related mortality
Mortality due to documented or clinically diagnosed infection/meningitis according to the oonsulting physician.
Overall clinical success
This referred to survival at the EOT with clinical and microbiological success, and no relapse or recurrence during the 30-day follow-up period.
Statistical analysis
The aim of this study was to compare the clinical success, mortality, and overall clinical success rates for cohorts that received the three empirical regimens. We used SPSS version 25.0 (Chicago, IL, USA) for all analyses. We evaluated the difference between groups using the χ2 test and one-way ANOVA test, as indicated. The significance level was set at p < 0.05.
Results
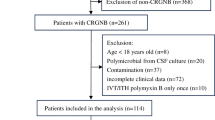
A total of 170 postneurological meningitis cases were included in the study, with 20 patients in the cefepime + vancomycin (CV) group, 31 in the ceftazidime + vancomycin (CFV) group, and 119 in the meropenem + vancomycin (MV) group. Of these patients, 28 (16.5%) had shunt infections, 20 (11.8%) were on lumbar drainage, and 36 (21.2%) were on external ventricular drainage at the time of diagnosis of nosocomial meningitis. Table 1 shows the underlying diseases, age, and other characteristics of the cases. There were no significant differences between the three therapy cohorts in terms of underlying diseases, shunt, lumbar or extraventricular drainage, treatment duration, gender, and age. However, admission to the intensive care unit (ICU) and any antibiotic therapy during the one-month prior to the meningitis episode were significantly more common in the MV subgroup.
Clinical presentation and diagnosis
Out of the total of 170 cases, 113 cases (66.5%) presented with fever, 92 cases (54.1%) exhibited disturbances in consciousness, 61 (36%) had neck stiffness, and 39 cases (22.9%) had all three symptoms, known as the classical triad. Additionally, 20 (11.8%) cases had convulsions and 55 (32.4%) had nausea and vomiting (Table 2).
The mean levels for white blood cells and CRP were 15,089 ± 8106/mm3 and 15.20 ± 15.93 mg/dl, respectively. Out of 170 patients, 128 (75%) had leukocytosis (> 10,000/mm3). Additionally, 32 cases did not have leukocytosis but showed polymorphonuclear leukocyte predominance (> 64%) (Table 2).
The mean CSF leukocyte count was 1365 ± 2668/mm3 (range 10–20350/mm3), while the mean CSF protein and the mean CSF glucose levels were 215.15 ± 195.26 mg/dl (range 2–917 mg/dl) and 43.04 ± 30.21 mg/dl (range 0–144 mg/dl), respectively.
A total of 42 patients (24.7%) tested positive for Gram-stain, while 107 cases (62.9%) tested positive for CSF culture. No bacteriological agent was found in 63 cases (37.1%). Of the 66 bacteria isolated in CSF culture positive cases, 61.7% were Gram-negative while 46.7% were Gram-positive. The most common etiologic agent was A. baumannii, followed by coagulase-negative staphylococci and S. aureus (Table 2). Nine cases (5.3%) were found to have mixed infections. Twenty-two (91.7%) of the A. baumannii strains were resistant to carbapenem, and none were intermediately-resistant. Of all the Gram-negative bacteria, 9.2%, 64.6%, 52.3%, and 38.4% were ESBL producers, resistant to ceftazidime, cefepime, and carbapenem, respectively.
Although the rate of methicillin resistance among CNS strain was 71.4%, it was 63.1.% among S. aureus strains. Fortunately, there were no cases of fungal meningitis. However, one (0.6%) of the causative agents was vancomycin-resistant E. faecium.
Magnetic resonance imaging (MRI) was conducted on 77% of the overall cohort (132 patients). Out of the 132 patients, 10 cases (7.57%) showed normal MRI results. The most common MRI findings were postoperative changes (46.9%), hydrocephalus (28%), intracranial hemorrhage (9%), and abscess (6.1%). Besides, the MRI detected ventriculitis in two cases (1.5%).
According to Table 2, there was no significant difference among the three treatment groups in relation to symptoms, blood WBC, CRP, CSF bacterial etiology, CSF findings, MRI performed cases, cases with normal MRI and ventriculitis in MRI. However, the MV cohort had a significantly lower mean GCS score, and the CV cohort had a greater number of CSF culture-negative cases.
Clinical efficacy
The clinical response on day 3–5 ranged between 45–54.8%. However, there was no significant difference between the three groups (p = 0.472, Table 3). A total of 56 cases that had positive CSF culture (32.9%) did not have a repeated CSF culture on day 3–5 or died before that time point. Nonetheless, there was no significant difference in day 3–5 microbiological responses between the three groups (p = 0.736, Table 3).
The clinical success rate at the EOT was 80%, 54.8%, and 57.9% for the CV, CFV, and MV cohorts, respectively (p = 0.143, Table 3). There was no significant difference in EOT clinical success rates among the CSF culture-negative subgroups. Overall, vancomycin demonstrated an EOT clinical success rate of 60.6% (20/34) in the subgroup of methicillin-resistant staphylococci + ampicillin-resistant enterococci. Treatment failure occurred in two patients with vancomycin MIC > 1mg/l, but EOT success was achieved in 9 out of 10 patients with vancomycin MIC ≤ 1mg/l (p = 0.007). Nevertheless, as expected, the EOT clinical success rate was 0% in the carbapenem-resistant HCAM subgroup in the overall cohort (0/23).
Finally, there was no significant difference in terms of overall clinical success rate between the treatment groups (p = 0.252), as well as for both microbiologically confirmed (p = 0.874) and microbiologically unconfirmed meningitis subgroups (p = 0.337) (Table 3).
Sequalae
The overall rate of sequela was 19.4%. Interestingly, no sequela was reported in the CV or CFV groups, while all sequelae were in the MV group, any sequalae was significantly higher than CF or CFV groups (p = 0.0015). However, there was no significant difference in terms of any sequela subgroup between the CV, CFV, and MV cohorts (see Table 3).
Mortality
Overall ACM on day 30 of HCAM empirical treatment was 24.1% and did not differ significantly between the three groups as well as in möicrobioogically confirmed or unconfirmed subgroups (Table 3). At EOT (CV-CFV-MV), the overall mortality rate was 18.8%. The lowest mortality rate was observed in the CV cohort (10%), while the highest was observed in the CFV cohort (22.5%) (p = 0.489). The infection-related mortality rate during meningitis treatment (CV-CFV-MV) was 13.5%, with no significant difference among the three cohorts (p = 0.821). Thirteen cases died during the 30-day follow-up period for those with successful EOT (p = 0.101). Table 3 provides a summary of the mortality data.
Adverse events
One participant in the CV cohort experienced an adverse event (AE) of abdominal pain. In the CFV cohort, four participants developed AEs, with two complaining of diarrhea, one reporting abdominal distention, and one requiring a drug switch due to an abnormal liver function test. Finally, six participants in the MV cohort experienced AEs, with three reporting nephrotoxicity, two experiencing a local reaction at the IV entrance site, and one requiring a drug switch due to an allergic reaction. The number of participants who experienced AEs that necessitated a change in therapy was similar across the three cohorts (p > 0.05, see Table 3).
Discussion
HCAM is a very serious type of healthcare-associated infection that poses significant patient risks. The HCAM guidelines recommend ceftazidime, cefepime, or meropenem + vancomycin as empirical therapy options [5]. Although these combinations are the most commonly suggested regimens [1, 2, 4, 5], there has been no controlled or uncontrolled comparative analysis to determine the efficacy of these options. Cefepime has an advantage over ceftazidime in that it is resistant to inducible Ampc type beta-lactamases, while ceftazidime and cefepime both have the disadvantage of being susceptible to most ESBLs compared to meropenem. However, all three options are sensitive to carbapenemases [13, 14]. Using only one option for continuous antibiotic pressure may contribute to resistance; therefore, increasing the number of available empirical therapy options could increase the effective consumption periods of the available antibiotic options [13]. This study was conducted to determine whether these three options may be alternative to each other.
HCAM is a relatively rare nosocomial infection. However, in centers with overloaded neurosurgery clinics, it may comprise a more significant part of overall nosocomial infections. While HCAM is rare, it can lead to a mortality rate of 16–40.8% [15,16,17,18,19,20,21] and significant morbidity. In our cohort, overall mortality at EOT (CV-CFV-MV) was 18,8%. The lowest mortality was observed in CV cohort (10%) and highest in CFV cohort (22.5%) (p = 0.489) all of which are compatible with the results published in the literature [15,16,17,18,19,20,21]. It is worth noting that some patients experienced a relapse or developed other nosocomial infections, leading to additional mortality during the follow-up period. Hence, in our study, after 18.8% EOT mortality an additional 13 (7.6%) patients died until day 30 follow up. However, there was no significant difference in terms of mortality analysis between the three treatment groups.
As our study was a retrospective cohort study, it was not possible to balance the cohorts in all parameters including patient numbers or culture-negative cases in the three cohorts. MV combination was used more commonly than CV or CFV combination in the study centers, which created an imbalance in disfavor of CV and CFV cohorts. Additionally, the GCS at the start of empirical antibiotic therapy, the number of patients managed in the ICU, and the number of cases that received antibiotics in the previous month of the HCAM episode were significantly disfavored in the MV arm. It is possible that all these disadvantages, which are risk factors for ESBL, might have caused selection of meropenem rather than cefepime or ceftazidime. Furthermore, sequalae were more common in the MV arm, which may be due to the significantly lower GCS score and significantly higher ICU need in that cohort [1, 4]. However, the EOT clinical success, day-30 mortality, and overall clinical success at the end of the one-month follow-up did not differ significantly between the three cohorts.
Nosocomial Acinetobacter infections, including meningitis, are becoming increasingly common in ICUs. According to a recent systematic review of HCAM in Turkey [3], Acinetobacter spp. caused 30.7% of 899 CSF culture positive nosocomial meningitis episodes. The pooled carbapenem-resistance rate was 37.5%. In addition, carbapenem-resistant Enterobacteriales are increasingly being reported as a cause of HCAM [22, 23]. However, carbapenems, ceftazidime, and cefepime have the disadvantage of not covering carbapenem-resistant strains. As a result, all three treatment arms evaluated in our cohorts failed in the carbapenem-resistant subgroup.
Herein, we detected the overall clinical success rate with vancomycin as 60.6% in the ampicillin-resistant enterococci and methicillin-resistant staphylococci subgroup. As glycopeptides are relatively large molecules, their ability to penetrate the central nervous system is limited. Strains with a low MIC (< 1mg/l) are expected to have a higher likelihood of clinical success. Hence, we found that clinical success at EOT was lower in patients with a vancomycin MIC > 1mg/l compared to those with a MIC ≤ 1mg/l (p = 0.001) [9, 24, 25].
The reported penetration rates of the included antimicrobial agents into inflamed CSF are as follows: 20–40% for ceftazidime [26], 10.3% for cefepime [27], 39% for meropenem [27], and 30% for vancomycin [27]. However, the drug levels were not measured in any of the study centers.
Our study has several limitations i) its retrospective design ii) with a relatively small number of cases in the ceftazidime and cefepime groups, it was underpowered to demonstrate the efficacy of the three empirical treatment regimens in well-balanced cohorts and also unable to show the outcome differences in methicillin-resistant versus sensitive cases, as well as 3rd generation and carbapenem resistant bacterial strains iii)the absence of antibiotic levels, pharmacokinetic and pharmacodynamic data including vancomycin, which were not measured in any of the cases iv) repeated lumbar puncture was not repeated In all cases vi) we did not analyse the neutrophil rates of CSF samples v) all the included cases fulfilled the inclusion criteria but we did not further examine the excluded cases) vi) Though we could include the meningitis episodes developping after 90 days we wanted to stay within the 90 days period in implant cases [28]. Herein, our primary objective was to compare the efficacies of empirical therapy and assess EOT clinical success and EOT mortality as the most critical outcomes. However, due to the fact that EOT not having a fixed time point, we conducted further analysis of day-30 ACM, which could have been impacted by revisions to intravenous/intrathecal antibiotic therapy after the etiology was elucidated. Nevertheless, needing such modifications was considered an unsuccessful outcome, and analysis of these modifications was kept outside the scope of this study. Additionally, infection related mortality was considered as per the treating physician. Due to the inability to perform autopsies, definitive reasons for mortality could not be determined. Our analysis indicated considerable mortality, relapse, and reinfection after the EOT, suggesting potential problems in infection control or reaching the best available therapy (especially in carbapenem-resistant Gram-negative cohort) at the study centers. Despite these limitations, to our knowledge, this is the first and the largest dataset evaluating the microbiological and clinical efficacy of empirical therapy regimens in HCAM, providing valuable insights into this area of study.
In conclusion this retrospective cohort study revealed no significant difference in EOT clinical success, EOT mortality, overall clinical success, and day-30 ACM among the three treatment arms. Our study was the first to compare three empirical therapy regimens in HCAM. While all three options had basicdisadvantages against carbapenem-resistant strains, vancomycin was found to have average efficacy against methicillin-resistant staphylococci. We suggest a randomized controlled trial to further analyze these three regimens. In addition, we suggest evaluating empirical therapy regimens that may be effective against carbapenem-resistant Gram-negative bacteria. We strongly recommend developing speedy diagnostic systems for HCAM, similar to those used in community-acquired meningitis or other infections [29, 30]. Finally the medical community should seek more effective measures for infection control in HCAM.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author (Dr Deniz Akyol) upon reasonable request.
References
Bardak-Ozcem S, Sipahi OR. An updated approach to healthcare-associated meningitis. Expert Rev Anti Infect Ther. 2014;12(3):333–42.
Ippolito M, Giarratano A, Cortegiani A. Healthcare-associated central nervous system infections. Curr Opin Anaesthesiol. 2022;35(5):549–54.
Sipahi OR, Nazli Zeka A, Taşbakan M, Pullukçu H, Arda B, Yamazhan T, Sipahi H, Ulusoy S. Pooled analysis of 899 nosocomial meningitis episodes from Turkey. Turk J Med Sci. 2017;47(1):29–33.
Van de Beek D, Cabellos C, Dzupova O, Esposito S, Klein M, Kloek AT, Leib SL, Mourvillier B, Ostergaard C, Pagliano P, Pfister HW, Read RC, Sipahi OR, Brouwer MC, ESCMID Study Group for Infections of the Brain (ESGIB). ESCMID guideline: diagnosis and treatment of acute bacterial meningitis. Clin Microbiol Infect. 2016;22(Suppl 3):37–62.
Tunkel AR, Hasbun R, Bhimraj A, Byers K, Kaplan SL, Scheld WM, van de Beek D, Bleck TP, Garton HJL, Zunt JR. 2017 Infectious Diseases Society of America’s Clinical Practice Guidelines for Healthcare-Associated Ventriculitis and Meningitis. Clin Infect Dis. 2017;64(6):e34–65.
Tunkel AR, Hartman BJ, Kaplan SL, Kaufman BA, Roos KL, Scheld WM, Whitley RJ. Practice guidelines for the management of bacterial meningitis. Clin Infect Dis. 2004;39(9):1267–84.
Van de Beek D, Drake JM, Tunkel AR. Nosocomial bacterial meningitis. N Engl J Med. 2010;362:146–54.
Karvouniaris M, Brotis A, Tsiakos K, Palli E, Koulenti D. Current Perspectives on the Diagnosis and Management of Healthcare-Associated Ventriculitis and Meningitis. Infect Drug Resist. 2022;28(15):697–721.
Sipahi OR, Bardak S, Turhan T, Arda B, Pullukcu H, Ruksen M, Aydemir S, Dalbasti T, Yurtseven T, Zileli M, Ulusoy S. Linezolid in the treatment of methicillin-resistant staphylococcal post-neurosurgical meningitis: a series of 17 cases. Scand J Infect Dis. 2011;43(10):757–64.
Garner JS, Jarvis WR, Emori TG, Horon TC, Hughes JM. CDC definitions for nosocomial infections. In: Olmsted RN, editor. APIC infection control and applied epidemiology: Principles and practice. St. Louis, USA: Mosby; 1996. p. A1–20.
Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Twenty-third Informational Supplement M100–S23. Wayne, PA, USA: CLSI; 2013.
European Committee on Antimicrobial Susceptibility Testing Breakpoint tables for interpretation of MICs and zone diameters. Version 6.0, valid from 2016–01–01. Available from http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_6.0_Breakpoint_table.pdf. Accessed 12 Mar 2023.
Sipahi OR. Economics of antibiotic resistance. Expert Rev Anti Infect Ther. 2008;6(4):523–39.
Rodríguez-Baño J, Gutiérrez-Gutiérrez B, Machuca I, Pascual A. Treatment of Infections Caused by Extended-Spectrum-Beta-Lactamase-, AmpC-, and Carbapenemase-Producing Enterobacteriaceae. Clin Microbiol Rev. 2018;31(2):e00079-e117.
Durand ML, Calderwood SB, Weber DJ, et al. Acute bacterial meningitis in adults. A review of 493 episodes. N Engl J Med. 1993;328:21–8.
Weisfelt M, Van de Beek D, Spanjaard L, de Gans J. Nosocomial bacterial meningitis in adults. A prospective series of 50 cases. J Hosp Infect. 2007;66(1):71–8.
Wang KW, Chang WN, Huang CR, et al. Post-neurosurgical nosocomial bacterial meningitis in adults: microbiology, clinical features, and outcomes. J Clin Neurosci. 2005;12(6):647–50.
Reichert MC, Medeiros EA, Ferraz FA. Hospital-acquired meningitis in patients undergoing craniotomy: incidence, evolution, and risk factors. Am J Infect Control. 2002;30(3):158–64.
Dizbay M, Güzel Tunccan O, Arman D, et al. Factors associated with mortality in nosocomial central nervous system infections. ANKEM Derg. 2011;25(1):6–11.
Erdem I, Hakan T, Metin F, et al. Clinical features, laboratory data management and the risk factors that affect the mortality in patients with postoperative meningitis. Neurol India. 2008;56(4):433–7.
Van de Beek D, Brouwer MC, Thwaites GE, Tunkel AR. Advances in treatment of bacterial meningitis. Lancet. 2012;380(9854):1693–702.
Tuon FF, Rocha JL, Arend LN, Wallbach K, Zanin HA, Pilonetto M. Treatment and outcome of nine cases of KPC-producing Klebsiella pneumoniae meningitis. J Infect. 2013;67:161–4.
Guanghui Z, Jing L, Guojun Z, Hong L. Epidemiology and risk factors of neurosurgical bacterial meningitis/encephalitis induced by carbapenem resistant Enterobacteriaceae. J Infect Chemother. 2020;26:101–6.
Matsubara H, Makimoto A, Higa T, et al. Successful treatment of meningoencephalitis caused by methicillin-resistant Staphylococcus aureus with intrathecal vancomycin in an allogeneic peripheral blood stem cell transplant recipient. Bone Marrow Transplant. 2003;31:65–7.
Arda B, Yamazhan T, Sipahi OR, İşlekel S, Büke Ç, Ulusoy S. Meningitis due to methicillin-resistant Staphylococcus aureus (MRSA): review of 10 cases. Int J Antimicrob Agents. 2005;25(5):414–8.
The Sanford Guide to Antimicrobial Therapy. Dallas. TX: Antimicrobial Therapy Inc; 2021.
Nau R, Sörgel F, Eiffert H. Penetration of drugs through the blood-cerebrospinal fluid/blood-brain barrier for treatment of central nervous system infections. Clin Microbiol Rev . 2010;23(4):858-83.
Sikora A, Zahra F. Nosocomial Infections. [Updated 2023 Apr 27]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559312/. Accessed 12 Mar 2023.
Kahraman H, Tünger A, Şenol Ş, Gazi H, Avcı M, Örmen B, Türker N, Atalay S, Köse Ş, Ulusoy S, Işıkgöz Taşbakan M, Sipahi OR, Yamazhan T, Gülay Z, Alp Çavuş S, Pullukçu H. Investigation of bacterial and viral etiology in community acquired central nervous system infections with molecular methods. Mikrobiyol Bul. 2017;51(3):277–85.
Bastug A. Rational use of syndromic approach. Mediterr J Infect Microb Antimicrob. 2022;11(Supp 1):4.
Acknowledgements
Authors thank European Study Group for Infections of Brain (Esgib) and Infectious Diseases International Research Initiative (ID-IRI). A part of this study has been presented as a poster presentation in European Conference for Clinical Microbiology and Infectious Diseases in 2021 (p 1435) and as an oral presentation in Annual Congress of Infectious Diseases and Clinical Microbiology Specialty Society of Türkiye (Türkiye-Ekmud) in 2019.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
Conceptualization: Oğuz Reşat Sipahi, Deniz Akyol, Sercan Ulusoy; Methodology: Oğuz Reşat Sipahi, Meltem Taşbakan, Hüsnü Pullukçu, Tansu Yamazhan, Bilgin Arda; Data collection: Bahar Örmen, Gönül Çiçek-Şentürk, Sinan Mermer, Uğur Önal, Fatma Amer, Maysaa Abdallah Saed, Kevser Özdemir, Elif Tükenmez-Tigen, Nefise Öztoprak, Ummugülsüm Altın, Behice Kurtaran, Corneliu Petru Popescu, Mustafa Sakçı, Bedia Mutay Suntur, Vikas Gautam, Megha Sharma, Şafak Kaya, Eren Fatma Akçıl, Selçuk Kaya, Tuba Turunc, Pınar Ergen, Özlem Kandemir, Salih Cesur, Selin Bardak Ozcem, Erkin Özgiray, Taşkın Yurtseven, Hüseyin Aytaç Erdem, Hilal Sipahi, Bilgin Arda, Hüsnü Pullukçu, Meltem Taşbakan, Tansu Yamazhan, Sohret Aydemir; Formal analysis and investigation: Hilal Sipahi; Writing—original draft preparation: Deniz Akyol, Uğur Önal; Writing—review and editing: Oğuz Reşat Sipahi, Deniz Akyol, Bilgin Arda, Sercan Ulusoy.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of Ege University Instituonal Review Board (16–3.2–54) and was conducted following the legal requirements and tenets of the Declaration of Helsinki and its subsequent amendments. The need to obtain written informed consent was waived by the Ethics Committee of Ege University Hospital due to the retrospective nature of the study.
We confirm that all methods were carried out in accordance with relevant guidelines and regulations. Ethical approval was granted from Ege University Institutional Review Board (16–3.2–54). Informed consent was obtained from all subjects and/or their legal guardian(s).
Consent for publication
Not applicable.
Competing interests
Oguz Resat Sipahi, Sercan Ulusoy, Bilgin Arda, Meltem Taşbakan, Hüsnü Pullukçu and Tansu Yamazhan received speaker’s honorarium from Pfizer. Others have none to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Sipahi, O.R., Akyol, D., Ormen, B. et al. Empirical cefepime+vancomycin versus ceftazidime+vancomycin versus meropenem+vancomycin in the treatment of healthcare-associated meningitis: results of the multicenter Ephesus study. BMC Infect Dis 23, 639 (2023). https://doi.org/10.1186/s12879-023-08596-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-023-08596-z