
Abstract
Background
To guide decision-making on immunisation programmes for ageing adults in Europe, one of the aims of the Vaccines and InfecTious diseases in the Ageing popuLation (IMI2-VITAL) project is to assess the burden of disease (BoD) of (potentially) vaccine-preventable diseases ((P)VPD). We aimed to identify the available data sources to calculate the BoD of (P)VPD in participating VITAL countries and to pinpoint data gaps. Based on epidemiological criteria and vaccine availability, we prioritized (P) VPD caused by Extra-intestinal pathogenic Escherichia coli (ExPEC), norovirus, respiratory syncytial virus, Staphylococcus aureus, and pneumococcal pneumonia.
Methods
We conducted a survey on available data (e.g. incidence, mortality, disability-adjusted life years (DALY), quality-adjusted life years (QALY), sequelae, antimicrobial resistance (AMR), etc.) among national experts from European countries, and carried out five pathogen-specific literature reviews by searching MEDLINE for peer-reviewed publications published between 2009 and 2019.
Results
Morbidity and mortality data were generally available for all five diseases, while summary BoD estimates were mostly lacking. Available data were not always stratified by age and risk group, which is especially important when calculating BoD for ageing adults. AMR data were available in several countries for S. aureus and ExPEC.
Conclusion
This study provides an exhaustive overview of the available data sources and data gaps for the estimation of BoD of five (P) VPD in ageing adults in the EU/EAA, which is useful to guide pathogen-specific BoD studies and contribute to calculation of (P)VPDs BoD.
Similar content being viewed by others


Background
In 2019, ageing adults (≥50 years) represented about 40% of the population in the European Union (EU), and this proportion is expected to reach 50% by 2025 [1,2,3,4,5]. This rising demographic trend is expected to lead to a growing demand for healthcare as infectious diseases in ageing adults, especially those affecting the elderly (≥65 years), already place a significant health and economic burden on individuals and societies [1, 6, 7]. Ageing adults experience a natural decline in their immune response, also called immuno-senescence [5, 6], increasing their risk of contracting infectious diseases, as well as their risk of a severe disease course. Ageing patients often present with atypical symptoms, thereby complicating the clinical diagnosis [8,9,10]. Moreover, for persons living in elderly care institutions, close living arrangements can further increase the risk of infection.
Prevention strategies, and more specifically vaccination, are often a cost-effective way to decrease the incidence of infectious diseases, thereby contributing to healthy ageing [11,12,13]. Although effective vaccines are already available to prevent some major infectious diseases in ageing adults, such as influenza and pneumococcal disease [1, 14], their vaccination coverage rates remain relatively low in Europe [6]. This is likely due to limited awareness of the adverse impacts on health arising from infectious diseases, and existing gaps in the promotion of adult vaccinations by public health authorities [1, 6]. To guide decision-making about potential prevention strategies for this age-group, it is essential to understand the burden of disease (BoD) and to identify existing data gaps.
In this context, the second Innovative Medicine Initiative (IMI2) supported the Vaccines and InfecTious Diseases in the Ageing PopuLation (IMI2-VITAL) project [15], which aims to address the current challenges of (potentially) vaccine-preventable diseases ((P)VPD) in ageing adults in the EU/EEA. The project will provide evidence-based knowledge on possible specific vaccination strategies to enhance healthy ageing.
We present here a comprehensive review of currently available data sources in the EU/EEA for 2009–2019 to calculate the BoD of (P)VPD in ageing adults and describe the data gaps.
Methods
Disease selection
We identified (P)VPD based on WHO summary information [16] and input from project members. We subsequently selected diseases to review based on their relevance for EU/EEA and the ageing adult population, and the availability of a vaccine in at least phase 2 of clinical development. This resulted in a list of seven infectious diseases: influenza, varicella/herpes zoster, herpes simplex virus, norovirus, respiratory syncytial virus (RSV), Staphylococcus aureus (S. aureus), extra-intestinal pathogenic Escherichia coli (ExPEC), and pneumococcal pneumonia (PnPn). This list was further narrowed down to diseases with a high BoD and/or lack of BoD data. The ranking resulted in five (P)VPD to be assessed on data sources for this review: norovirus, S. aureus, ExPEC, PnPn, and RSV.
National disease expert surveys
An online survey on BoD data was developed for each of the selected (P)VPD and sent to disease experts from IMI2-VITAL participating countries (Belgium, Denmark, Hungary, Italy, The Netherlands, Norway and Spain). The experts were identified by the IMI2-VITAL partners who aimed to adhere to the European Centre for Disease Prevention and Control (ECDC) national focal points. The parameters of interest included summary measures (disability-adjusted life year (DALY), quality-adjusted life year (QALY)), utility/disability, morbidity, mortality, antimicrobial resistance (AMR), other pathogen-associated and patient registry data.
The surveys, developed in Google Forms, were based on case definitions described in Table 1 with a supplementary example available in Additional file 1. The survey responses were summarised by listing the available data for each BoD indicator by country.
Literature reviews
A literature review was conducted by searching the MEDLINE database (via PubMed) for peer-reviewed publications with data relevant to BoD calculations. A search strategy was developed for each disease, consisting of a common part across all diseases and a disease-specific part (Additional file 2). The former contained search terms on BoD parameters, age group and the period of interest, while the latter contained the name of the pathogen, clinical syndromes and related synonyms. The BoD parameters included summary measures (DALY, QALY, years of life lost (YLL), years lived with disability (YLD) and Quality of Life (QoL)), disability/utility, morbidity mortality and AMR data. The period of interest was restricted to the last 10 years (01/01/2009–23/05/2019), except for PnPn, where only publications since 01/01/2012 were included. The rationale was to exclude data reported before large-scale paediatric use of more-valent pneumococcal conjugate vaccines (PCV10/PCV13), as this has impacted the BoD in the ageing population due to indirect effects [17, 18].
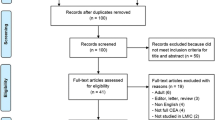
The literature selection process and the number of excluded publications by reason were documented and presented in PRISMA flow-diagrams (Additional file 3). Titles and abstracts of identified records were screened by one reviewer to identify studies that fulfilled the selection criteria. Studies were excluded if there was 1) No English abstract and an irrelevant title, 2) No human subjects, 3) No relation to the disease of interest, 4) No new evidence described (editorials, letters, case reports/series), 5) No relevant data (this criterion was further specified in each disease area according to the characteristics of the disease in question, see definitions on the PRISMA flowcharts), 6) Only children, or 7) If the study was conducted outside of Europe. A sample of 100 abstracts per disease was double-screened, and discrepancies were discussed among reviewers. Data from the selected publications were then extracted using a uniform Excel table for all diseases. Based on the available literature, summary tables were created to list the countries for which BoD parameters were available.
Results
Extra-intestinal pathogenic Escherichia coli
Survey
The Netherlands, Denmark and Norway use the proposed case definition in their surveillance (Table 1). In Italy, only a subset of laboratories within the European AMR surveillance network (EARS-net) use this case definition. Hungary uses a non-agent specific definition for Hospital-Associated Bloodstream Infections (HA-BSI) [19], Belgium and Spain do not collect ExPEC-specific data. None of the countries reported summary BoD measures (Table 2). Stratification by age-group and risk factors was reported as possible in the six countries for which morbidity data are available (Hungary, Denmark, Norway, Italy, and The Netherlands). ExPEC-mortality and sequelae data were rarely available. The latter could only be retrieved in The Netherlands. All countries collected AMR data.
Literature review
A total of 940 publications were identified in the literature review, of which 41 were included for data extraction covering eleven countries (Additional files 3 and 4). Most publications came from the United Kingdom (UK) (n = 9), Denmark (n = 6) and Spain (n = 4) (Table 3). Additionally, seven publications included multiple countries for data extraction. Respectively, twelve and three publications focused on E.coli bacteraemia and urosepsis. Sixteen studies provided general Bloodstream Infection (BSI) morbidity data. Only eight studies presented E.coli bacteraemia incidence. Seven publications concerned BSI caused by AMR E.coli strains. Several countries presented data on E.coli BSI mortality (Denmark, Finland, Norway, Sweden and the UK) or AMR E.coli-related BSI mortality (Germany and Spain). A large European study reporting ICU-specific mortality data was also identified. Many publications focusing on AMR E.coli BSI were found. Two large AMR-focused surveillance systems were identified (SENTRY and EARS-Net) [20, 21]. Only one study reported DALYs for AMR E.coli, and no study reported disability/utility weights, disease duration, or the need for hospitalisation due to ExPEC (hospitalisation needs).
Norovirus
Survey
Belgium, Italy and Spain use both the norovirus and syndromic (acute gastroenteritis) case definitions in their surveillance (Table 1). Denmark uses only the norovirus case definition. The Netherlands collects aggregated laboratory surveillance data on norovirus. Hungary and Norway collect data on norovirus outbreaks. The survey results indicated that the majority of countries collected norovirus morbidity data (6 out of 7), mortality data (4 out of 7), and hospitalisation data (4 out of 7) (Table 2). In addition, Belgium, Denmark and the Netherlands estimated DALYs specifically for norovirus.. However, only a few countries assessed the level of under-reporting or under-ascertainment (i.e. completeness) of morbidity data, and morbidity and mortality data were rarely stratified by age or risk factors. No country collected sequelae data.
Literature review
The literature review yielded 371 publications, of which 24 were selected for data extraction (Additional files 3 and 4). Data from eight countries were retrieved, mostly from the Netherlands (n = 6), the UK (n = 6) and Germany (n = 5) (Table 2). Four studies (from the UK and the Netherlands) estimated DALYs based on incidence data obtained via the population-based studies Sensor [22] and IID2 (Infectious Intestinal Disease in the community study) [23, 24]. Morbidity data were retrieved in 24 publications, half of them describing pathogen-specific data, in most cases stratified by age. Sequelae data were identified in three syndromic data studies. Norovirus and syndromic disease mortality data were identified in eight and three studies, respectively.
Pneumococcal pneumonia
Survey
Spain and Italy use the non-bacteraemia PnPn case definition in their surveillance, whereas the other countries use only the all-cause pneumonia case definition (Table 1). Overall, PnPn-specific BoD data is lacking, as no country collected summary BoD data, and only Spain and Italy reported PnPn-morbidity and mortality data (Table 2). On the other hand, more data was available for all-cause pneumonia; Belgium and the Netherlands reported that DALY and/or QALYs have already been calculated or could be calculated for all-cause pneumonia. All-cause pneumonia incidence and hospitalisation data are available in most countries, and mortality data are available in the Netherlands, Belgium and Hungary.
Literature review
A total of 784 publications were identified, of which 40 were included for data extraction (Additional files 3 and 4). Most studies were conducted in Spain (n = 9), the Netherlands (n = 8), the UK (n = 7) and Italy (n = 5) (Table 2). Only two studies reported QALYs; both were based on the CAPITA study from the Netherlands on all-cause pneumonia [25, 26]. Two studies from France and Switzerland determined the QoL for all-cause pneumonia [27, 28]. For most studies, the incidence was based on hospital discharge data, either for all-cause pneumonia or PnPn. Incidence data on outpatients with all-cause pneumonia were only reported for France, the Netherlands and Belgium. Serotype-specific PnPn incidence data were available in three studies. Several studies reported the attributable fraction for pneumococci using hospital discharge data. Most studies reported age stratification data and half of them reported data for risk groups. Several studies reported mortality after PnPn or after all-cause pneumonia.
Respiratory syncytial virus
Survey
Case definitions and methods to ascertain RSV cases differ widely by country (Table 1). In Belgium and Spain, laboratory testing is usually conducted only in a selection of hospitalized cases. In the Netherlands, while a subset of ARI cases undergoes laboratory testing for RSV and real-time SARI surveillance is being piloted, no official laboratory confirmation is needed for applying ICD-10 codes in hospitalized cases. Many hospitals in Norway conduct influenza like illness (ILI) surveillance with RSV and influenza panel testing, which results in RSV-positivity among ILI cases. Under-ascertainment and underreporting may bias the official frequency estimates as the completeness of reported frequency data are not assessed in any of the countries (Table 2). The only exception might be the Netherlands, where efforts have been made to assess data completeness for RSV cases identified in primary care. RSV sequelae data are available from Denmark, and are also currently being studied in the Netherlands, in the context of the RESCEU (Respiratory Syncytial virus Consortium in Europe) project [27]. Spain has reported that hospital records could be used as a possible source of sequelae data. As several countries use SARI case definitions for RSV (Belgium, Spain, the Netherlands, Denmark), there are available data on hospitalisations and RSV-specific mortality. In Belgium, sentinel hospitals report case-fatality and RSV-SARI mortality data, which can be stratified by age and risk groups. There are also case-fatality data in Spain, but only for younger age-groups and for a subset of cases which undergo laboratory testing.
Literature review
The literature search yielded a total of 711 publications, of which 46 were included in the data extraction (Additional files 3 and 4). The majority of studies originated from the UK (n = 12), followed by Sweden (n = 4), France (n = 3), Poland (n = 3), Spain (n = 3), Germany (n = 2), Greece (n = 2), the Netherlands (n = 2), Switzerland (n = 2), and Belgium (n = 1) (Table 2). In the literature review, the most widely used case definitions for sampling are based on ILI or ARI cases, or both. Although one article reported age-specific DALYs due to hospitalised lower or upper respiratory tract infections (LRTIs and URTIs) caused by RSV, no study described country-specific summary BoD estimates. In a study by Shi et al. [28], simple BoD data (RSV incidence, hospital admission rates, RSV positivity among hospitalised ARI cases and hospital case fatality ratios for RSV) were estimated for industrialised vs developing countries, but no European-level data were described. Age stratification and risk factor data (co-morbidities, such as cardiopulmonary and cardiovascular diseases), immunocompromised health status, and seasonality were widely reported in publications. Publications analysing RSV surveillance data in the Netherlands and the UK contained robust data on RSV-attributable mortality. Case fatality rates were estimated in literature reviews performed in French and Swedish hospitals [28, 29].
Staphylococcus aureus
Belgium, Denmark, Italy, the Netherlands, Norway and Spain reported using the abovementioned S.aureus case definition in their surveillance (Table 1). Hungary uses the official non-specific ECDC case definition of HAI, including the one for BSI [19]. Only Belgium reported that DALYs could be calculated, although only for general nosocomial infections but not for those which are pathogen-specific (Table 2). None of the surveyed countries collect disability/utility weights. All countries, except for Norway, have S.aureus incidence data available or data which is easily retrievable and can be stratified by risk factors. Several countries stated that they collect sequelae and hospitalisation data. Very few countries collect mortality data, while all countries collect AMR data. Additionally, some countries collect non-BSI data, such as S.aureus pneumonia and surgical site infection cases.
Literature review
The literature search yielded 185 publications, of which 101 publications remained for data extraction after full-text review (Additional files 3 and 4). Most publications came from Denmark (n = 14), followed by Spain (n = 13), Germany (n = 9), England (n = 8), France (n = 7), and Finland (n = 6). Two large European surveillance systems were identified: the EARS-Net [20], and the Central Asian and Eastern European Surveillance of Antimicrobial Resistance (CAESAR) [29]. Both collect data on blood cultures and AMR, which can be used to calculate the incidence of S.aureus bacteraemia. EARS-Net also allows age and gender stratification (Table 2). None of the publications reported summary BoD measures. Incidence data could be extracted from 51 publications. In most cases, data were stratified by age. Sequelae and hospitalisation data were often retrievable. Disease duration was only reported in three studies. In total, 75 studies reported on S.aureus-specific or all-cause mortality. Many publications included risk factor analyses related to mortality data. Almost all publications reported AMR in S. aureus infections.
Discussion
This review provides a comprehensive overview of the available data sources and gaps for estimating BoD for five priority (P)VPD in ageing adults in the EU/EAA.
Our expert surveys reveal that morbidity data are generally available for the diseases of interest. Furthermore, the majority of countries collect mortality data for norovirus, PnPn and RSV, or for the associated syndromic disease, such as acute gastroenteritis. These results are corroborated by the results of the literature review, especially for S.aureus, ExPEC and RSV.
We found that summary BoD estimates, such as DALYs and QALYs, are rarely available for the five diseases. These summary measures are particularly valuable for understanding the health impacts from a specific (P)VPD in relation to other health conditions that affect ageing adults [30]. Additionally, some parameters are missing, such as the disability weights (DWs) needed to calculate summary BoD estimates. DWs indicate the severity of illness for a given non-fatal health outcome and are typically based on the preferences of a panel of patients or medical experts that rates the relative undesirability of hypothetical health outcomes [31, 32]. Since DWs can depend on the cultural values and distribution of health conditions that are specific to the setting in which they are elicited, their valuation should be ideally based on elicitation panels specific for the population of interest [33]. However, in practice, the analysts make use of large databases of elicited DWs covering a wide range of diseases/health conditions such as those produced for the Global Burden of Disease study [34, 35].
Another important data gap is the overall absence of completeness assessments of morbidity data. Given that population-based disease incidence and/or prevalence data are the central components of summary BoD measures, it is fundamental to assess the validity of these parameters. Notwithstanding the high quality of current EU infectious disease surveillance systems, underestimation is known to be a common issue in surveillance data. Its magnitude may vary depending on the disease, country, time period, and patient characteristics, and this variation can be due to various factors such as differences in healthcare-seeking behaviour, case management, and surveillance systems [36,37,38]. Estimates of underestimation may be obtained, for example, by comparing passive surveillance system data to population-based survey data. Several methods are available to adjust BoD input data and thus estimate true incidence [30].
Moreover, morbidity/incidence data were not systematically stratified by age and risk group. The lack of age-specific parameters that are needed for accurate DALY/QALY computation represents a critical data gap in the context of ageing adults. Kristensen et al. [39] studied BoD in ageing adults for four vaccine-preventable diseases and pinpointed that more precise BoD estimates could be obtained by specifying age-specific, rather than ‘age-agnostic’, indicators (i.e. overall values). It is noteworthy that stratification on age is also important for transition probabilities (e.g., the risk of developing complications following acute infection) and is expected to be larger in ageing adults, but these were not investigated in our review.
Although it is preferable to rely on country-specific data to estimate BoD, estimates for some parameters can be extrapolated from another country if no country-specific data are available. For example, case-fatality rates from one country may be applicable to other countries with similar health care systems. However, unlike case-fatality rates, incidence data usually depend greatly on the country, and therefore, country-specific incidence estimates are critical for BoD estimates.
Although we have seen that morbidity data are widely available, these data might not always be pathogen specific. For (P)VPDs, such as PnPn or norovirus, laboratory confirmation and pathogen-specific incidence data are currently scarce in EU/EEA, and, consequently, it might be challenging to estimate BoD for these pathogens. In this case, data on the incidence of a clinically-defined set of symptoms or clinical syndrome (e.g. pneumonia, gastroenteritis, etc.) need to be first attributed to the responsible pathogen(s), usually by resorting to an attributable fraction obtained from the literature, or otherwise estimated. For PnPn and norovirus, more such data are needed to accurately estimate the BoD of (P)VPDs for European countries.
For ExPEC, which is usually a hospital-detected infection, the attribution of BoD to the infection or the patient’s underlying condition poses an additional challenge for the estimation of BoD that needs to be handled. The true ExPEC infection incidence must be extrapolated from available observed cases. Indeed, infections in ageing adults are often associated with co-morbidities, and thus, are reported as secondary diagnoses in hospital care [7].
Based on studies including outpatient PnPn, the burden of PnPn is underestimated when using only hospitalised patient data [40, 41]. Therefore, the identified lack of data on outpatient pneumonia should be taken into account, and assessments of the degree of under-reporting and under-ascertainment of the incidence data are also needed. Furthermore, there is a lack of serotype-specific data, which is mainly due to methodological challenges. As long as pneumococcal vaccines do not cover all serotypes, the BoD for the vaccine-preventable part of all PnPn can only be estimated with available serotype-specific data.
In the case of ExPEC and S.aureus, incidence and mortality data are available but are often restricted to resistant strains. Also, summary BoD measure estimates might be underestimated because patients infected with drug-susceptible strains are not included in the calculations.
The main limitation of our study is that not all EU/EEA countries were covered by the disease expert survey. Also, the survey responses were not formally validated, even though the results were shared and discussed within the IMI2-VITAL project Consortium. In addition, although the extended literature review allowed us to capture peer-reviewed literature, only a limited and selected amount of grey literature was covered in our study. The literature reviews were restricted to English language publications, and in consequence, we may have missed some important data sources. Finally, the disease outcome trees, the duration of possible sequelae, and transition probabilities between health outcomes were not considered in our study, although these parameters would also be needed to compute summary BoD measures.
Conclusions
Despite the fact that several methodological tools are available to overcome at least some of the data gaps identified, the results of this review have highlighted the need for more BoD studies to be conducted. Our findings may guide future studies towards specific (P)VPDs, countries and parameters for which information is currently lacking. Furthermore, all the data retrieved can be used to find references for specific BoD parameters. This information will be useful for the remainder of the IMI2-VITAL project, but may also be used to inform other BoD studies on (P)VPD. In addition, this study provides a framework that can be easily adapted to other vaccine-preventable diseases in the future.
Availability of data and materials
The data supporting the conclusions of this article are included within the article and its additional files.
Abbreviations
- AMR:
-
Antimicrobial resistance
- BoD:
-
Burden of Disease
- BSI:
-
Bloodstream Infection
- DALY:
-
Disability-Adjusted Life Year
- DW:
-
Disability weight
- ECDC:
-
European Centre for Disease Prevention and Control
- ExPEC:
-
Extra-intestinal pathogenic Escherichia coli
- HA-BSI:
-
Hospital-Associated Bloodstream Infections
- IMI:
-
Innovative Medicine Initiative
- LRTI:
-
Lower respiratory tract infection
- PnPn:
-
Pneumococcal pneumonia
- (P)VPD:
-
(Potentially) vaccine-preventable diseases
- QALY:
-
Quality-Adjusted Life Year
- QoL:
-
Quality of Life
- RSV:
-
Respiratory syncytial virus
- S. aureus :
-
Staphylococcus aureus
- URTI:
-
Lower respiratory tract infection
- VITAL:
-
Vaccines and InfecTious Diseases in the Ageing PopuLation
- YLD:
-
Years Lived with Disability
- YLL:
-
Years of Life Lost
References
Esposito S, Franco E, Gavazzi G, de Miguel AG, Hardt R, Kassianos G, et al. The public health value of vaccination for seniors in Europe. Vaccine. 2018;36(19):2523–8. https://doi.org/10.1016/j.vaccine.2018.03.053.
World, B., World Bank staff estimates based on age/sex distributions of United Nations Population Division's World Population Prospects: 2019 Revision. 2019 Available at: https://data.worldbank.org/indicator/SP.POP.65UP.TO.ZS?contextual=default&end=2018&start=1960&view=chart.
Choi C, S.N.F, Vaffis S, John J, Patel J, Gerhart J, et al. Aging of the global population. Value Outcomes Spotlight. 2019;5(5):22.
Eurostat. Population by age group. 2020.
Vollset SE, Goren E, Yuan CW, Cao J, Smith AE, Hsiao T, et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: a forecasting analysis for the global burden of disease study. Lancet. 2020;396(10258):1285–306. https://doi.org/10.1016/S0140-6736(20)30677-2.
SAATI, Adult vaccination: a key component of healthy ageing. The benefits of life-course immunisation in Europe. 2018.
Talbird SE, et al. Impact of population aging on the burden of vaccine-preventable diseases among older adults in the United States. Human Vaccines & Immunotherapeutics; 2020. p. 1–12.
Wester AL, Dunlop O, Melby KK, Dahle UR, Wyller TB. Age-related differences in symptoms, diagnosis and prognosis of bacteremia. BMC Infect Dis. 2013;13(1):346. https://doi.org/10.1186/1471-2334-13-346.
Abbara A, et al. Time to diagnosis of tuberculosis is greater in older patients: a retrospective cohort review. 2019. ERJ Open Research 5: 00228-2018.
El Chakhtoura NG, Bonomo RA, Jump RL. Influence of aging and environment on presentation of infection in older adults. Infect Dis Clin. 2017;31(4):593–608. https://doi.org/10.1016/j.idc.2017.07.017.
Wolff E, Storsaeter J, Örtqvist Å, Naucler P, Larsson S, Lepp T, et al. Cost-effectiveness of pneumococcal vaccination for elderly in Sweden. Vaccine. 2020;38(32):4988–95. https://doi.org/10.1016/j.vaccine.2020.05.072.
van Lier A, van Hoek AJ, Opstelten W, Boot HJ, de Melker HE. Assessing the potential effects and cost-effectiveness of programmatic herpes zoster vaccination of elderly in the Netherlands. BMC Health Serv Res. 2010;10(1):237. https://doi.org/10.1186/1472-6963-10-237.
De Graeve D, Lombaert G, Goossens H. Cost-effectiveness analysis of pneumococcal vaccination of adults and elderly persons in Belgium. Pharmacoeconomics. 2000;17(6):591–601. https://doi.org/10.2165/00019053-200017060-00005.
Vestergaard LS, et al. Excess all-cause and influenza-attributable mortality in Europe, December 2016 to February 2017. Eurosurveillance. 2017;22(14):30506.
Van Baarle D, Bollaerts K, Del Giudice G, Lockhart S, Luxemburger C, Postma MJ, Timen A, Standaert B. Preventing infectious diseases for healthy ageing: The VITAL public-private partnership project. Vaccine. 2020;38:5896–90.
WHO. Immunization, Vaccines and Biologicals: Vaccines and diseases. 2020.
Shiri T, Datta S, Madan J, Tsertsvadze A, Royle P, Keeling MJ, et al. Indirect effects of childhood pneumococcal conjugate vaccination on invasive pneumococcal disease: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(1):e51–9. https://doi.org/10.1016/S2214-109X(16)30306-0.
Davis SM, Deloria-Knoll M, Kassa HT, O’Brien KL. Impact of pneumococcal conjugate vaccines on nasopharyngeal carriage and invasive disease among unvaccinated people: review of evidence on indirect effects. Vaccine. 2013;32(1):133–45. https://doi.org/10.1016/j.vaccine.2013.05.005.
ECDC. Field Epidemiology Manual Wiki : Bloodstream Infection 2020.
ECDC. External quality assessment of laboratory performance - European Antimicrobial Resistance Surveillance Network (EARS-Net), 2017. Stockholm: ECDC; 2018.
Diekema DJ, Hsueh P-R, Mendes RE, Pfaller MA, Rolston KV, Sader HS, Jones RN. The microbiology of bloodstream infection: 20-year trends from the SENTRY antimicrobial surveillance program. Antimicrob Agents Chemother. 2019; 63:e00355-19.
De Wit M, et al. Sensor, a population-based cohort study on gastroenteritis in the Netherlands: incidence and etiology. Am J Epidemiol. 2001;154(7):666–74. https://doi.org/10.1093/aje/154.7.666.
Tam CC, Rodrigues LC, Viviani L, Dodds JP, Evans MR, Hunter PR, et al. Longitudinal study of infectious intestinal disease in the UK (IID2 study): incidence in the community and presenting to general practice. Gut. 2012;61(1):69–77. https://doi.org/10.1136/gut.2011.238386.
O'Brien SJ, Rait G, Hunter PR, Gray JJ, Bolton FJ, Tompkins DS, et al. Methods for determining disease burden and calibrating national surveillance data in the United Kingdom: the second study of infectious intestinal disease in the community (IID2 study). BMC Med Res Methodol. 2010;10(1):39. https://doi.org/10.1186/1471-2288-10-39.
Mangen M-JJ, Huijts SM, Bonten MJM, de Wit GA. The impact of community-acquired pneumonia on the health-related quality-of-life in elderly. BMC Infect Dis. 2017;17(1):208. https://doi.org/10.1186/s12879-017-2302-3.
Mangen M-JJ, Rozenbaum MH, Huijts SM, van Werkhoven CH, Postma DF, Atwood M, et al. Cost-effectiveness of adult pneumococcal conjugate vaccination in the Netherlands. Eur Respir J. 2015;46(5):1407–16. https://doi.org/10.1183/13993003.00325-2015.
Nickler M, et al. Prospective evaluation of biomarkers for prediction of quality of life in community-acquired pneumonia. Clin Chem Lab Med. 2016;54(11):1831–46.
Andrade LF, Saba G, Ricard JD, Messika J, Gaillat J, Bonnin P, et al. Health related quality of life in patients with community-acquired pneumococcal pneumonia in France. Health Qual Life Outcomes. 2018;16(1):28. https://doi.org/10.1186/s12955-018-0854-6.
Organization, W.H., Central Asian and eastern European surveillance of antimicrobial resistance: annual report 2018. 2018.
IMI2-VITAL, Report on burden methodologies and data sources to assess potential and gaps. 2019: https://vital-imi.eu/work-package-1/.
Devleesschauwer B, Havelaar AH, Maertens de Noordhout C, Haagsma JA, Praet N, Dorny P, et al. Calculating disability-adjusted life years to quantify burden of disease. Int J Public Health. 2014;59(3):565–9. https://doi.org/10.1007/s00038-014-0552-z.
Mangen M, Plass D, Kretzschmar M. Estimating the current and future burden of communicable diseases in the European Union and EEA/EFTA; 2014.
de Noordhout CM, et al. Mapping EQ-5D utilities to GBD 2010 and GBD 2013 disability weights: results of two pilot studies in Belgium. Arch Public Health. 2017;75(1):1–12.
Haagsma JA, et al. Assessing disability weights based on the responses of 30,660 people from four European countries. Popul Health Metrics. 2015;13(1):1–15.
Salomon JA, Haagsma JA, Davis A, de Noordhout CM, Polinder S, Havelaar AH, et al. Disability weights for the global burden of disease 2013 study. Lancet Glob Health. 2015;3(11):e712–23. https://doi.org/10.1016/S2214-109X(15)00069-8.
Gibbons CL, Mangen MJ, Plass D, Havelaar AH, Brooke RJ, Kramarz P, et al. Measuring underreporting and under-ascertainment in infectious disease datasets: a comparison of methods. BMC Public Health. 2014;14(1):147. https://doi.org/10.1186/1471-2458-14-147.
Bijkerk, P., et al., State of infectious diseases in the Netherlands 2015. 2016.
Haagsma J, Geenen PL, Ethelberg S, Fetsch A, Hansdotter F, Jansen A, et al. Community incidence of pathogen-specific gastroenteritis: reconstructing the surveillance pyramid for seven pathogens in seven European Union member states. Epidemiol Infect. 2013;141(8):1625–39. https://doi.org/10.1017/S0950268812002166.
Kristensen M, van Lier A, Eilers R, McDonald SA, Opstelten W, van der Maas N, et al. Burden of four vaccine preventable diseases in older adults. Vaccine. 2016;34(7):942–9. https://doi.org/10.1016/j.vaccine.2015.12.052.
Personne V, Chevalier J, Buffel du Vaure C, Partouche H, Gilberg S, de Pouvourville G. CAPECO: cost evaluation of community acquired pneumonia managed in primary care. Vaccine. 2016;34(19):2275–80. https://doi.org/10.1016/j.vaccine.2016.03.013.
KCE, Use of pneumococcal vaccines in the elderly: an economic evaluation 2016: https://kce.fgov.be/en/use-of-pneumococcal-vaccines-in-the-elderly-an-economic-evaluation.
Acknowledgements
We would like to thank all the disease experts that were asked to fill in the questionnaire for their time and insights.: Stephanie Jacquinet, Katrien Latour, Nathalie Bossuyt, Chloé Wyndham Thomas (Sciensano, Belgium), Germaine Hanquet (Belgium Health Care Knowledge Centre KCE, Belgium), Ingrid Friesema, Roan Pijnacker, Annelot Schoffelen, Anne Teirlinck (RIVM, Netherlands), Heidi Lange, Petter Elstrøm, Are Stuwitz Berg, Umaer Naseer, Brita Askeland Winje (Norwegian Institute of Public Health, Norway), Ágnes Dánielisz, Ágnes Csohán, Andrea Kurcz, Molnár Zsuzsanna (National Center for Public Health, Hungary), Susana Guix (Universidad de Barcelona, Spain), Luis Eduardo López Cortés (Hospital Virgen Macarena, Spain), Miquel Pujol (Hospital Universitario de Bellvitge, Spain), Rosa Rodriguez (Gregorio Marañon Hospital, Spain), Jesús Rodríguez Baño (Universidad de Sevilla, Spain), Rosario Menéndez (Univeristat de Valencia), Lasse Dam Rasmussen, Andreas Petersen, Ramona Trebbien, Flemming Scheutz, Palle Valentiner-Branth (Statens Serum Institut, Denmark), Giovanni Rezza, Monica Monaco, Marina Cerquetti, Romina Camilli (Istituto Superiore di Sanità, Italy). Next to that, we would like to acknowledge the help of Elvira Carrio and Alexandria Williams in writing assistance. The research leading to these results was conducted as part of the VITAL consortium. For further informaiton, please refer to www.vital-imi.eu.
Funding
The VITAL project has received funding from the Innovative Medicines Initiative 2 Joint Undertaking (JU) under grant agreement No 806776. The JU receives support from the European Union’s Horizon 2020 research and innovation programme, and EFPIA-members.
Author information
Authors and Affiliations
Contributions
E.M., J.F., T.A., B.A.W., A.O.S., A.S., S.A.M., K.B., M.J.K., have been involved in the design of the study and in drafting the content and structure of the manuscript and have approved the final version.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
E.M., J.F., T.A., B.A.W., A.S., S.A.M., K.B., M.J.K. have no competing interest. A.O.S. has received travel grants to attend meetings sponsored by pharmaceutical companies and has been principal investigator in studies sponsored by Sanofi Pasteur and Merck Sharp & Dohme.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Survey questionnaires.
Additional file 2.
Search strings literature reviews.
Additional file 3.
PRISMA flowcharts literature reviews.
Additional file 4.
References of literature reviews.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Méroc, E., Fröberg, J., Almasi, T. et al. European data sources for computing burden of (potential) vaccine-preventable diseases in ageing adults. BMC Infect Dis 21, 345 (2021). https://doi.org/10.1186/s12879-021-06017-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12879-021-06017-7