
Abstract
Background
Non-obstructive azoospermia (NOA) is considered to be the most severe form of male infertility. Before the emergence of surgical testicular sperm extraction and assisted reproductive technology, NOA patients could hardly become biological fathers of their children. However, failure of the surgery could cause physical and psychological harm to patients such as testicular damage, pain, hopeless of fertility and additional cost. Therefore, predicting the successful sperm retrieval (SSR) is so important for NOA patients to make their choice whether to do the surgery or not. Because seminal plasma is secreted by the testes and accessory gonads, it can reflect the spermatogenic environment, making it a preferential choice for SSR valuation. The purpose of this paper is to summarize the available evidence and provide the reader with a broad overview of biomarkers in seminal plasma for SSR prediction.
Results
A total of 15,390 studies were searched from PUBMED, EMBASE, CENTRAL and Web of Science, but only 6615 studies were evaluated after duplications were removed. The abstracts of 6513 articles were excluded because they were irrelevant to the topic. The full texts of 102 articles were obtained, with 21 of them being included in this review. The included studies range in quality from medium to high. In the included articles, surgical sperm extraction methods included conventional testicular sperm extraction (TESE) and microdissection testicular sperm extraction (micro-TESE). Currently, the biomarkers in seminal plasma used to predict SSR are primarily RNAs, metabolites, AMH, inhibin B, leptin, survivin, clusterin, LGALS3BP, ESX1, TEX101, TNP1, DAZ, PRM1 and PRM2.
Conclusion
The evidence does not conclusively indicate that AMH and INHB in seminal plasma are valuable to predict the SSR. It is worth noting that RNAs, metabolites and other biomarkers in seminal plasma have shown great potential in predicting SSR. However, existing evidence is insufficient to provide clinicians with adequate decision support, and more prospective, large sample size, and multicenter trials are urgently needed.
Résumé
Contexte
L’azoospermie non obstructive (ANO) est considérée comme la forme la plus grave d’infertilité masculine. Avant l’émergence de l’extraction chirurgicale de spermatozoïdes testiculaires et de la procréation médicalement assistée, les patients atteints d’ANO pouvaient difficilement devenir les pères biologiques de leurs enfants. Cependant, l’échec de la chirurgie peut causer des dommages physiques et psychologiques aux patients, tels que des lésions testiculaires, des douleurs, une fertilité impossibilité et des coûts financiers supplémentaires. Par conséquent, prédire une récupération réussie de spermatozoïdes (RRS) est très important pour les patients avec ANO, pour faire leur choix de réaliser ou non la chirurgie. Comme le plasma séminal est sécrété par les testicules et les glandes accessoires, il peut être le reflet de l’environnement de la spermatogenèse, ce qui en fait un choix préférentiel pour l’évaluation de la RRS. Le but du présent article est de résumer les preuves disponibles, et de fournir au lecteur un aperçu général des biomarqueurs du plasma séminal susceptibles de prédire la RRS.
Résultats
Au total, 15390 études ont été consultées à partir de PUBMED, EMBASE, CENTRAL et Web of Science, mais seulement 6615 ont été évaluées après suppression des doublons. Les résumés de 6513 articles ont été exclus car non pertinents pour le sujet. Les textes intégraux de 102 articles ont été obtenus, dont 21 ont été inclus dans cette revue. La qualité des études incluses varie de moyenne à élevée. Dans ces articles inclus, la méthode chirurgicale d’extraction de spermatozoïdes était soit l’extraction conventionnelle de spermatozoïdes testiculaires (TESE), soit l’extraction de spermatozoïdes testiculaires par microdissection (micro-TESE). Actuellement, les biomarqueurs du plasma séminal utilisés pour prédire la RRS sont principalement les ARN, les métabolites, l’AMH, l’inhibine B, la leptine, la survivine, la clusterine, LGALS3BP, ESX1, TEX101, TNP1, DAZ, PRM1 et PRM2.
Conclusions
Les preuves n’indiquent pas de façon concluante que l’AMH et l’INHB dans le plasma séminal sont utiles pour prédire la RRS. Il convient de noter que les ARN, métabolites et autres biomarqueurs du plasma séminal ont montré un potentiel élevé de prédiction de la RRS. Cependant, les preuves existantes sont insuffisantes pour fournir aux cliniciens une aide à la décision adéquate ; des essais plus prospectifs, de grande taille, et multicentriques sont nécessaires de toute urgence.
Similar content being viewed by others

Introduction
It is estimated that infertility affects 8–12% of couples globally, with a male factor being a primary or contributing cause in approximately 50% of couples [1, 2]. Non-obstructive azoospermia (NOA) is defined as the absence of sperm in ejaculation caused by impaired spermatogenesis, which is the most severe form of male infertility. The prevalence of NOA is 1% in all men and 10-15% in infertile men [3,4,5]. Historically, NOA men are considered to be infertile, but the emergence of testicular sperm extraction and ICSI has made it possible for NOA men to become biological fathers of their children. Although the testicular sperm extraction technology is constantly improving, about 50% of NOA patients still cannot find sperm through surgery, and surgery will inevitably lead to testicular damage and increase the pain and cost consumption of patients. Therefore, how to determine whether it is necessary to carry out testicular sperm extraction through preoperative evaluation is a problem that reproductive andrologists have been exploring. Successful sperm retrieval (SSR) is defined as obtaining at least one spermatozoon via surgical testicular sperm extraction [6]. Although the value of serum hormonal markers in predicting SSR was expected, the research results were unsatisfactory [7].
Seminal plasma (SP) is a biological fluid made up of secretions from glands, such as testes, in the male urogenital tract. It could be a rich source of noninvasive biomarkers, including tissue-specific RNAs and proteins, where abnormal changes could directly indicate a pathological process in the testis [8]. Therefore, the utility of SP biomarkers in predicting SSR is constantly being investigated. To date, the genomic, transcriptomic, proteomic, and metabolomic profiles of human SP have been studied to predict SSR, with promising results [9]. This review aims to summarize the differences in SP biomarkers in NOA men with positive and negative surgical TESE outcomes and to provide the reader with a broad overview of SP biomarkers for predicting SSR.
Material and methods
A search of PUBMED, EMBASE, CENTRAL and Web of Science were made for studies that compared SP biomarkers in NOA men with positive and negative surgical testicular sperm extraction (Table 1). The search terms considered the following MeSH (Medical Subject Headings) terms, which were adjusted for each database: (Semen OR “Seminal Plasma” OR “Plasma, Seminal” OR “Seminal fluid” ) AND (Azoospermia OR Aspermia). No language or date limits were set. Studies that compared biomarkers in SP of patients with NOA and patients with Obstructive Azoospermia (OA) or oligospermia or normozoospermia were excluded because these studies were not direct evidence to predict SSR. Only studies that compared SP biomarkers in NOA men with positive and negative outcomes of surgical testicular sperm extraction were included. Newcastle-Ottawa scale (NOS) was used to evaluate the quality assessment of the enrolled nonrandomized studies [10]. The quality assessment of the selected studies was independently completed by two reviewers (Junjun Li and Xujun Yu). Studies were then classified according to their quality into poor (0–4), moderate (5–6), or high quality (7–9).
Results
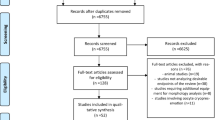
A total of 15,390 studies were searched, but only 6615 studies were included for evaluation after duplications were removed. 6513 articles were excluded based on the abstracts irrelevant to the topic. The full texts of 102 articles were retrieved, of which 81 articles did not meet the inclusion criteria and were excluded from the review (Fig. 1). Therefore, a total of 21 articles [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31] were included in this review. One study did not mention the surgical sperm extraction method [11], 13studies [12,13,14,15,16,17,18,19,20, 23,24,25,26] compared the difference of SP biomarkers between positive and negative conventional testicular sperm extraction (TESE) outcomes, and six studies [22, 27,28,29,30,31] compared the difference of SP biomarkers between positive and negative microdissection testicular sperm extraction (micro-TESE) outcomes in NOA men. One study studied both TESE and micro-TESE [21]. Among the SP biomarkers investigated are RNAs, metabolites, AMH, inhibin B and others (See Table 2 ). According to the NOS for nonrandomized studies, the quality assessment was considered moderate [11, 12, 14, 15, 19,20,21,22,23,24,25,26, 30] and high quality [13, 17, 18, 27,28,29, 31], as demonstrated in Table 3.

Flowchart of study selection process. A total of 15,390 studies were searched, but only 6615 studies were evaluated after duplications were removed. The abstracts of 6513 articles were excluded because they were irrelevant to the topic. The full texts of 102 articles were obtained, with 21 of them being included in this review
Discussion
Seminal Plasma Transcriptome (RNAs)
The term transcriptome refers to the total amount of RNA in a specific specimen. The human SP contains approximately 700 extracellular RNAs that are involved in regulating vesicle-mediated transport, protein kinase inhibition, and cell response to zinc, which may reflect the spermatogenesis state in the testis [32]. To date, the biomarkers studied in studies of SP RNAs difference between NOA patients with positive and negative surgical sperm extraction include microRNAs [26, 30], long noncoding RNAs [28], circRNAs [29], and tsRNAs [31].
MicroRNAs
MicroRNAs (miRNAs) are small noncoding RNA molecules with 18–25 nucleotides, which can regulate post translation gene expression by triggering translation inhibition or mRNA degradation. It has been confirmed that miRNAs are involved in the regulation of germ cell development and spermatogenesis [33, 34]. Given the abnormal expression of various miRNAs involved in spermatogenesis in NOA patients and the importance of miRNAs targeting pathways in successful spermatogenesis [35], it is reasonable to believe that miRNA has a high potential for predicting SSR. In fact, miRNAs exist not only in the intracellular environment but also in the extracellular environment, particularly in various biofuels, such as SP [36]. miRNAs are found in SP as microvesicular bodies and protein-bonded complexes [37]. Because of the existence and distribution of miRNAs, semen miRNAs are protected from degradation by existing RNase enzymes, making them potential noninvasive indicators of spermatogenesis.
Barceló et al. [26] found no significant differences in SP-miRNAs between eight NOA patients who had successful TESE and four NOA patients who had failed TESE. A multiple regression analysis model containing miR-539-5p and miR-941 had 100% sensitivity and specificity in predicting the presence of sperm in testicular biopsy for the samples in the study. Zhang et al. [30] recently examined the SP-miRNAs from NOA patients with successful and unsuccessful micro-TESE (n = 6 in each group) and fertile men (n = 6). Their results showed that high levels of hsa-miR-34b-3p and hsa-miR-34c-3p expressions were associated with successful micro-TESE. In contrast, high levels of hsa-miR-3065-3p and hsa-miR-4446-3p expressions are associated with failed micro-TESE. Furthermore, a predictive model based on these four miRNAs was developed with high predictive accuracy (AUC = 0.927). Although these SP-miRNAs need to be validated in larger cohort studies, the current results indicate that SP-miRNAs have a high potential for predicting the SSR of NOA patients.
Long noncoding RNAs
Long non-coding RNAs (lncRNAs) are a group of RNA transcripts with longer than 200 nucleotides and without protein-coding capacity. It was revealed that the lnc RNAs could be involved in the regulation of gene expression at the transcriptional, post-transcriptional and epigenetic levels, and chromatin remodeling. Studies have also demonstrated that lncRNAs play a critical role in spermatogenesis [38, 39], indicating that lncRNAs may be potential biomarkers for predicting SSR in NOA men. Xie et al. [28] recently sequenced the RNA of SP extracellular vesicle from six normozoospermic men and five idiopathic NOA patients with failed micro-TESE. They constructed and validated a lncRNA biomarker panel in 96 NOA patients receiving micro-TESE. Then, a prediction model (AUC was 0.986 in the training set and 0.960 in the validation set) with nine differentially expressed testis-specific lncRNAs, including LOC100505685, SPATA42, CCDC37-DT, GABRG3-AS1, LOC440934, LOC101929088 (XR_927561.2), LOC101929088 (XR_001745218.1), LINC00343, and LINC00301, was established. The most important finding of this study is that in the same group of patients with NOA, the prediction ability of the model based on these nine lncRNAs for SSR is significantly higher than that based on sex hormones. Finally, sperm retrieval surgery may be recommended if the score of the NOA case exceeds 0.532, according to the decision-making procedure made by the lncRNA panel. However, the regulatory functions and mechanisms of these lncRNAs in spermatogenesis must be clarified, and their predictive value must be confirmed in larger sample size studies.
CircRNAs
Circular RNAs (circRNAs) are covalent closed-loop structures formed by front-to-tail reverse shearing of precursor mRNAs [40].CircRNAs are stable in a variety of body fluids (such as semen and blood) because they are not affected by RNA exonuclease. CircRNAs could also be detected in seminal plasma at room temperature [41]. The role of circRNAs in spermatogenesis has been established, and several circRNAs have been found in seminal plasma, implying that circRNA deregulation is linked to various types of male infertility, including NOA [42]. Ji et al. [29] discovered three SP circRNAs (hsa_circ_0000277, hsa_circ_0060394 and hsa_circ_0007773) that differed between NOA patients with successful and unsuccessful micro-TESE, and these three circRNAs have a high predictive value for micro-TESE results (AUC values: 0.920, 0.928 and 0.891, respectively). Furthermore, a new prediction model based on the combination of the three circRNAs demonstrated good SSR prediction value (AUC value: 0.958), indicating that circRNAs derived from SP testis may be used as reliable biomarkers to predict SSR in patients with NOA. However, the number of cases in this study was small, and the function of these circRNAs and their relationship to spermatogenesis remain unknown.
tsRNAs
tRNA derived small RNAs (tsRNAs), known as new regulatory small non coding RNAs, are precisely regulated by the processing of tRNA and its precursors. It has been demonstrated that tsRNAs are widely involved in large quantities of physiological and pathological processes [43]. According to studies, tsRNAs are closely related to mammalian sperm maturation and fertilization and are abundant in SP [44, 45], implying that tsRNAs could be potential biomarkers for SSR prediction. Han et al. [31] recently compared the SP extracellular vesicle tsRNA levels in 18 NOA patients with successful micro-TESE and 23 NOA patients with unsuccessful micro-TESE and found that tRF-Val-AAC-010 expression levels were higher in the successful micro-TESE group than in the unsuccessful micro-TESE group, resulting in good predictive accuracy (AUC = 0.89, sensitivity = 72%, specificity = 91%, P < 0.0001). Moreover, tRF-Val-AAC-010 had a higher predictive accuracy than testicular volume and serum FSH. More importantly, it was demonstrated that tRF-Val-AAC-010 can be expressed in testicular tissues of patients with NOA and participate in spermatogenesis, implying that tRF-Val-AAC-010 could be a potential SP biomarker for predicting SSR.
Metabolites
Following genomics and proteomics, metabonomics is a developed discipline that is an important part of systems biology. Gene and protein expression are closely linked, whereas metabolites can better reflect the cell environment, which is closely related to cell nutrition, the role of drugs and pollutants in the environment, and other external factors. Approximately 40,000 human metabolites have been found in the 3.0 Human Metabolome Database [46]. At present, a number of metabonomic methods have been defined, including metabolome mapping, metabolic fingerprinting, metabolic profiling, metabolic footprinting, and metabolic target analysis, and untargeted metabolic profiling. The classification of specific metabolic biomarkers, in particular, is useful in better identifying male infertility [47]. Existing research suggests that metabolic fingerprinting of seminal plasma can be used as a useful diagnostic tool for men experiencing infertility [48, 49]. To the best of our knowledge, Gilany et al. [24] investigated metabolic profiling of SP of NOA men with successful and unsuccessful TESE and discovered 36 distinguishing metabolites as prognostic biomarkers for positive and negative TESE men. Furthermore, another study [25] revealed that the metabolic fingerprint, particularly the oxidative status, differed significantly between positive and negative TESE patients. These results indicate that SP metabolites have great potential as specific biomarkers for SSR prediction. The main shortcoming of these studies is that these metabolites lack effective validation and are not included in the Human Metabolome Database. Hence, more in-depth studies are required in the future.
AMH
The Anti-Mullerian hormone (AMH), which plays an important role in the maturation and differentiation of spermatogenic cells, is expressed in Sertoli cells and it governs the regression of the Müllerian ducts of the male fetus [50]. It is worth noting that after puberty, AMH secretion into the seminiferous tubule lumen by apical Sertoli cells is greater than basal secretion into the interstitium and blood circulation. Therefore, AMH concentrations in SP are higher in adult males than in serum [51, 52]. Moreover, AMH in SP can provide direct information about spermatogenesis [53]. This suggests that when investigating the possible relationship between AMH and spermatogenesis, it is preferable to measure SP-AMH rather than serum AMH. For this reason, the importance of SP-AMH in predicting SSR in patients with NOA is emphasized.
Fénichel et al. [11] published the first study comparing the concentrations of SP-AMH between patients with NOA who failed with surgical sperm extraction and those who succeeded in 1999, and the results revealed that of the 14 cases in which AMH could not be detected, 11 were negative for surgical sperm extraction, whereas seven of the nine cases in which AMH was detected were positive for surgical sperm extraction, indicating that AMH in SP is related to the SSR. However, the method of surgical sperm extraction was not mentioned in this study, and the sample size was only 23. Sabetian et al. [16] also reported that SP-AMH concentrations differed significantly between successful and unsuccessful TESE NOA men. Other studies came to the opposite conclusions as a result. Mostafa et al. [13] found that in the 17 cases where AMH could not be detected, 10 were successful TESE (58.2%), and 14 of the 23 cases where AMH was detected were unsuccessful TESE (57.5%), with no difference in SP-AMH levels between successful and unsuccessful TESE NOA men. Similarly, Duvilla et al. [14] found no difference in SP-AMH levels between successful and unsuccessful TESE NOA men. Afterward, a prospective study [17] with 139 NOA men compared SP-AMH concentrations between positive and negative TESE outcomes and concluded that SP-AMH concentrations did not differ significantly between successful and unsuccessful TESE patients. Furthermore, their logistic regression failed to demonstrate the predictive value of SP-AMH for SSR. In summary, SP-AMH cannot currently be used as an effective biomarker for positive sperm extraction.
Inhibin B
Inhibin B (INHB), a glycoprotein primarily produced by Sertoli cells, has a negative correlation with gonadotropin and FSH in feedback regulation and is closely related to the degree of spermatogenesis in testicular histology [54]. However, the value of serum INHB in predicting focal spermatogenesis remains debatable. Because the majority of INHB secreted by Sertoli cells enters the lumen space, the level of INHB in SP may more accurately reflect the functional state of seminiferous tubules. Nevertheless, there have been few studies on the use of SP-INHB to predict SSR.
Nagata et al. [12] compared SP-INHB concentrations in 17 NOA patients who had successful TESE to 45 NOA patients who had failed TESE and found that the SP-INHB concentrations in the successful TESE group were significantly higher. Further analysis revealed that the best discriminating level was 27.0 pg/mL (sensitivity 88.2%, specificity 93.3%), and multivariate logistic regression analysis revealed that SP-INHB was a significant predictor of TESE outcome. Similarly, Soudabeh et al. [16] showed that the SP-INHB concentrations in the successful TESE NOA men were significantly higher. On the other hand, a preliminary study [14] found no difference in SP-INHB between successful and unsuccessful TESE NOA men (n = 26). Another study [17] with a larger sample size compared the concentrations of SP-INHB between 60 NOA patients who had successful TESE and 79 NOA patients who had failed TESE and found that SP-INHB did not differ significantly between the two groups. The area under the receiver operating characteristic curve for SP-INHB was 0.502, and logistic regression did not show SP-INHB predictive value for SSR.
Overall, given the above contradictory results, the predictive value of SP-INHB for SSR in patients with NOA remains debatable. Randomized clinical trials with a large sample size and a multicenter design may help to clarify whether seminal plasma inhibin B contributes to SSR prediction in patients with NOA.
Other biomarkers
Survivin, which can regulate apoptosis, is found in rodent testes germ cells, particularly mature spermatocytes [55], and a decrease in survivin expression may result in spermatogenesis disorder [56]. Moreover, seminal survivin was detectable in 24 NOA men who had successful TESE but not in 13 NOA men who had unsuccessful TESE [15], implying that seminal survivin was associated with SSR in NOA men. Sertoli cells produce clusterin, which is secreted into the liquid of spermatogenic epithelium and deposited on the membranes of elongated sperm cells and mature sperm [57, 58]. Fukuda et al. [22] found no statistically significant differences of SP-clusterin levels between nine NOA patients who had successful micro-TESE and 19 patients who had failed micro-TESE. However, it is worth noting that their univariate analysis suggested SP-clusterin as a predictor of SSR. Leptin has been linked to spermatogenesis [59]. Ma et al. [18] found a significant difference in SP-leptin levels between positive and negative SSR groups, with a cut-off value of 2.9 ng/mL (sensitivity of 43.1% and specificity of 75.0%) to predict SSR at TESE with a limited value, but using artificial neural networks (ANNs) to combine leptin and other markers can significantly improve the prediction accuracy of sperm retrieval in NOA patients. However, in this study, there were no differences in neutral alpha glucosidase (NAG) and fructose levels between positive and negative TESE NOA patients. Freour et al. [20] used an isotope-coded protein label (ICPL)-based proteomic strategy coupled with a conventional protein assay to identify biomarkers of residual spermatogenesis in SP of NOA men. The results showed that the average concentrations of lectin galactoside binding and soluble 3 binding protein (LGALS3BP) in SP of patients with positive TESE were higher than those in patients with negative TESE, and SP-LGALS3BP concentrations less than 153 ng/mL were correlated with negative TESE results (sensitivity of 100% and specificity of 45%), indicating that SP-LGALS3BP may be an effective predictor of SSR. Furthermore, a number of germ cell-specific moleculars have been discovered to be useful in predicting SSR. By comparing histopathological results and germ cell-specific molecules, Aslani et al. [19] found that the expression of DAZ and PRM2 was related to the results of histopathological examination. There is also evidence that other germ cell-specific moleculars (such as TEX101 [23], ESX1 [21], TNP1, and PRM1 [27]) may help predict SSR, though the evidence is weak.
Conclusions
Although the predictive value of SP-AMH and SP-INHB for SSR was expected, the available evidence suggests that neither SP-AMH nor SP-INHB is widely accepted as predicting SSR in men with NOA. It is worth noting that RNAs, metabolites, and other biomarkers in SP have demonstrated a high potential in predicting SSR. If the specific role of these RNAs and metabolites in spermatogenesis can be confirmed in future research and further prospective, large sample size, and multicenter trials, it will provide more powerful support for SSR prediction.
Availability of data and materials
All data generated or analysed during this study are included in this published article and its supplementary information files.
Abbreviations
- AMH:
-
Anti Mullerian hormone
- ANNs:
-
Artificial neural networks
- ART:
-
Assisted reproductive technology
- circRNAs:
-
Circular RNAs
- INHB:
-
Inhibin B
- LGALS3BP:
-
lectin galactoside binding and soluble 3 binding protein
- lncRNAs:
-
Long non-coding RNAs
- micro-TESE:
-
Microdissection testicular sperm extraction
- miRNAs:
-
MicroRNAs
- NAG:
-
Neutral alpha glucosidase
- NOA:
-
Non-obstructive azoospermia
- NOS:
-
Newcastle-Ottawa scale
- OA:
-
Obstructive azoospermia
- SP:
-
Seminal plasma
- SSR:
-
Successful sperm retrieval
- TESE:
-
Conventional testicular sperm extraction
- tsRNAs:
-
tRNA derived small RNAs
References
Agarwal A, Baskaran S, Parekh N, Cho CL, Henkel R, Vij S, et al. Male infertility. Lancet. 2021;397(10271):319–33. https://doi.org/10.1016/S0140-6736(20)32667-2.
Minhas S, Bettocchi C, Boeri L, Capogrosso P, Carvalho J, Cilesiz NC, et al. European Association of Urology Guidelines on male sexual and Reproductive Health: 2021 update on male infertility. Eur Urol. 2021;80(5):603–20. https://doi.org/10.1016/j.eururo.2021.08.014.
Jarow JP, Espeland MA, Lipshultz LI. Evaluation of the Azoospermic patient. J Urol. 1989;142(1):62–5. https://doi.org/10.1016/s0022-5347(17)38662-7.
Stephen EH, Chandra A. Declining estimates of infertility in the United States:1982–2002. Fertil Steril. 2006;86(3):516–23. https://doi.org/10.1016/j.fertnstert.2006.02.129.
Tharakan T, Luo R, Jayasena CN, Minhas S. Non-obstructive azoospermia: current and future perspectives. Fac Rev. 2021;10:7. https://doi.org/10.12703/r/10-7.
Ramasamy R, Schlegel PN. Microdissection testicular sperm extraction: effect of prior biopsy on success of sperm retrieval. J Urol. 2007;177(4):1447–9. https://doi.org/10.1016/j.juro.2006.11.039.
Zarezadeh R, Fattahi A, Nikanfar S, Oghbaei H, Ahmadi Y, Rastgar Rezaei Y, et al. Hormonal markers as noninvasive predictors of sperm retrieval in non-obstructive azoospermia. J Assist Reprod Genet. 2021;38(8):2049–59. https://doi.org/10.1007/s10815-021-02176-3.
Drabovich AP, Saraon P, Jarvi K, Diamandis EP. Seminal plasma as a diagnostic fluid for male reproductive system disorders. Nat Rev Urol. 2014;11(5):278–88. https://doi.org/10.1038/nrurol.2014.74.
Zarezadeh R, Nikanfar S, Oghbaei H, Rastgar Rezaei Y, Jafari-Gharabaghlou D, Ahmadi Y, et al. Omics in seminal plasma: an effective strategy for Predicting sperm Retrieval Outcome in non-obstructive azoospermia. Mol Diagn Ther. 2021;25(3):315–25. https://doi.org/10.1007/s40291-021-00524-8.
Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–5. https://doi.org/10.1007/s10654-010-9491-z.
Fénichel P, Rey R, Poggioli S, Donzeau M, Chevallier D, Pointis G. Anti-Müllerian hormone as a seminal marker for spermatogenesis in non-obstructive azoospermia. Hum Reprod. 1999;14(8):2020–4. https://doi.org/10.1093/humrep/14.8.2020.
Nagata Y, Fujita K, Banzai J, Kojima Y, Kasima K, Suzuki M, et al. Seminal plasma inhibin-B level is a useful predictor of the success of conventional testicular sperm extraction in patients with non-obstructive azoospermia. J Obstet Gynaecol Res. 2005;31(5):384–8. https://doi.org/10.1111/j.1447-0756.2005.00306.x.
Mostafa T, Amer MK, Abdel-Malak G, Nsser TA, Zohdy W, Ashour S, et al. Seminal plasma anti-Müllerian hormone level correlates with semen parameters but does not predict success of testicular sperm extraction (TESE). Asian J Androl. 2007;9(2):265–70. https://doi.org/10.1111/j.1745-7262.2007.00252.x.
Duvilla E, Lejeune H, Trombert-Paviot B, Gentil-Perret A, Tostain J, Levy R. Significance of inhibin B and anti-mullerian hormone in seminal plasma: a preliminary study. Fertil Steril. 2008;89(2):444–8. https://doi.org/10.1016/j.fertnstert.2007.03.032.
Roshdy N, Mostafa T. Seminal plasma survivin in fertile and infertile males. J Urol. 2009;181(3):1269–72. https://doi.org/10.1016/j.juro.2008.10.158.
Soudabeh S, Ali MA, Mahshid H, Mohammad Mehdi A, Haleh S, Naser A, et al. Comparing seminal plasma biomarkers between normospermic and azoospermic men. J Reprod Infertil. 2010;11(1):39–46. doi: not provided.
Mitchell V, Boitrelle F, Pigny P, Robin G, Marchetti C, Marcelli F, et al. Seminal plasma levels of anti-Müllerian hormone and inhibin B are not predictive of testicular sperm retrieval in nonobstructive azoospermia: a study of 139 men. Fertil Steril. 2010;94(6):2147–50. https://doi.org/10.1016/j.fertnstert.2009.11.046.
Ma Y, Chen B, Wang H, Hu K, Huang Y. Prediction of sperm retrieval in men with non-obstructive azoospermia using artificial neural networks: leptin is a good assistant diagnostic marker. Hum Reprod. 2011;26:294–8. https://doi.org/10.1093/humrep/deq337.
Aslani F, Modarresi MH, Soltanghoraee H, Akhondi MM, Shabani A, Lakpour N, et al. Seminal molecular markers as a non-invasive diagnostic tool for the evaluation of spermatogenesis in non-obstructive azoospermia. Syst Biol Reprod Med. 2011;57(4):190–6. https://doi.org/10.3109/19396368.2011.569906.
Freour T, Com E, Barriere P, Bouchot O, Jean M, Masson D, et al. Comparative proteomic analysis coupled with conventional protein assay as a strategy to identify predictors of successful testicular sperm extraction in patients with non-obstructive azoospermia. Andrology. 2013;1(3):414–20. https://doi.org/10.1111/j.2047-2927.2012.00059.x.
Pansa A, Sirchia SM, Melis S, Giacchetta D, Castiglioni M, Colapietro P, et al. ESX1 mRNA expression in seminal fluid is an indicator of residual spermatogenesis in non-obstructive azoospermic men. Hum Reprod. 2014;29(12):2620–7. https://doi.org/10.1093/humrep/deu261.
Fukuda T, Miyake H, Enatsu N, Matsushita K, Fujisawa M. Seminal level of clusterin in infertile men as a significant biomarker reflecting spermatogenesis. Andrologia. 2016;48(10):1188–94. https://doi.org/10.1111/and.12558.
Korbakis D, Schiza C, Brinc D, Soosaipillai A, Karakosta TD, Légaré C, et al. Preclinical evaluation of a TEX101 protein ELISA test for the differential diagnosis of male infertility. BMC Med. 2017;15(1):60. https://doi.org/10.1186/s12916-017-0817-5.
Gilany K, Mani-Varnosfaderani A, Minai-Tehrani A, Mirzajani F, Ghassempour A, Sadeghi MR, et al. Untargeted metabolomic profling of seminal plasma in nonobstructive azoospermia men: a noninvasive detection of spermatogenesis. Biomed Chromatogr. 2017;31(8). https://doi.org/10.1002/bmc.3931.
Gilany K, Jafarzadeh N, Mani-Varnosfaderani A, Minai-Tehrani A, Sadeghi MR, Darbandi M et al. Pahlevanzadeh Z. Metabolic Fingerprinting of Seminal Plasma from Non-obstructive Azoospermia Patients: Positive Versus Negative Sperm Retrieval. J Reprod Infertil. 2018;19(2):109–114. doi: not provided.
Barceló M, Mata A, Bassas L, Larriba S. Exosomal microRNAs in seminal plasma are markers of the origin of azoospermia and can predict the presence of sperm in testicular tissue. Hum Reprod. 2018;33(6):1087–98. https://doi.org/10.1093/humrep/dey072.
Hashemi MS, Mozdarani H, Ghaedi K, Nasr-Esfahani MH. Could analysis of testis-specific genes, as biomarkers in seminal plasma, predict presence of focal spermatogenesis in non-obstructive azoospermia? Andrologia. 2020;52(2):e13483. https://doi.org/10.1111/and.13483.
Xie Y, Yao J, Zhang X, Chen J, Gao Y, Zhang C, et al. A panel of extracellular vesicle long noncoding RNAs in seminal plasma for predicting testicular spermatozoa in nonobstructive azoospermia patients. Hum Reprod. 2020;35(11):2413–27. https://doi.org/10.1093/humrep/deaa184.
Ji C, Wang Y, Wei X, Zhang X, Cong R, Yao L, et al. Potential of testis-derived circular RNAs in seminal plasma to predict the outcome of microdissection testicular sperm extraction in patients with idiopathic non-obstructive azoospermia. Hum Reprod. 2021;36(10):2649–60. https://doi.org/10.1093/humrep/deab196.
Zhang Y, Tang Y, Huang J, Liu H, Liu X, Zhou Y, et al. Circulating microRNAs in seminal plasma as predictors of sperm retrieval in microdissection testicular sperm extraction. Ann Transl Med. 2022;10(7):392. https://doi.org/10.21037/atm-21-5100.
Han X, Hao L, Shi Z, Li Y, Wang L, Li Z, et al. Seminal plasma extracellular vesicles tRF-Val-AAC-010 can serve as a predictive factor of successful microdissection testicular sperm extraction in patients with non-obstructive azoospermia. Reprod Biol Endocrinol. 2022;20(1):106. https://doi.org/10.1186/s12958-022-00978-3.
Jodar M, Sendler E, Krawetz SA. The protein and transcript profiles of human semen. Cell Tissue Res. 2015;363(1):85–96. https://doi.org/10.1007/s00441-015-2237-1.
Hayashi K, de Sousa Lopes SMC, Kaneda M, Tang F, Hajkova P, Lao K, et al. MicroRNA biogenesis is required for mouse primordial germ cell development and spermatogenesis. PLoS ONE. 2008;3(3):e1738. https://doi.org/10.1371/journal.pone.0001738.
Bouhallier F, Allioli N, Lavial F, Chalmel F, Perrard M-H, Durand P, et al. Role of miR-34c microRNA in the late steps of spermatogenesis. RNA. 2010;16(4):720–31. https://doi.org/10.1261/rna.1963810.
Rastgar Rezaei Y, Zarezadeh R, Nikanfar S, Oghbaei H, Nazdikbin N, Bahrami-Asl Z, et al. microRNAs in the pathogenesis of non-obstructive azoospermia: the underlying mechanisms and therapeutic potentials. Syst Biol Reprod Med. 2021;67(5):337–53. https://doi.org/10.1080/19396368.2021.1951890.
Weber JA, Baxter DH, Zhang S, Huang DY, How Huang K, Jen Lee M, et al. The MicroRNA spectrum in 12 body fuids. Clin Chem. 2010;56(11):1733–41. https://doi.org/10.1373/clinchem.2010.147405.
Li H, Huang S, Guo C, Guan H, Xiong C. Cell-free seminal mRNA and MicroRNA exist in different forms. PLoS ONE. 2012;7(4):e34566. https://doi.org/10.1371/journal.pone.0034566.
Luk AC, Chan WY, Rennert OM, Lee TL. Long noncoding RNAs in spermatogenesis: insights from recent high-throughput transcriptome studies. Reproduction. 2014;147(5):R131–41. https://doi.org/10.1530/REP-13-0594.
Joshi M, Rajender S. Long non-coding RNAs (lncRNAs) in spermatogenesis and male infertility. Reprod Biol Endocrinol. 2020;18(1):103. https://doi.org/10.1186/s12958-020-00660-6.
Meng S, Zhou H, Feng Z, Xu Z, Tang Y, Li P, et al. CircRNA: functions and properties of a novel potential biomarker for cancer. Mol Cancer. 2017;16(1):94. https://doi.org/10.1186/s12943-017-0663-2.
Dong WW, Li HM, Qing XR, Huang DH, Li HG. Identification and characterization of human testis derived circular RNAs and their existence in seminal plasma. Sci Rep. 2016;6:39080. https://doi.org/10.1038/srep39080.
Saberiyan M, Karimi E, Safi A, Movahhed P, Dehdehi L, Haririan N, et al. Circular RNAs: novel biomarkers in spermatogenesis defects and male infertility. Reprod Sci. 2022. https://doi.org/10.1007/s43032-022-00885-3.
Geslain R, Eriani G. Regulation of translation dynamic and neoplastic conversion by tRNA and their pieces. Translation (Austin). 2014;2(1):e28586. https://doi.org/10.4161/trla.28586.
Sharma U, Conine CC, Shea JM, Boskovic A, Derr AG, Bing XY, et al. Biogenesis and function of tRNA fragments during sperm maturation and fertilization in mammals. Science. 2016;351(6271):391–6. https://doi.org/10.1126/science.aad6780.
Kowalczykiewicz D, Swiercz A, Handschuh L, Lesniak K, Figlerowicz M, Wrzesinski J. Characterization of Sus scrofa small non-coding RNAs present in both female and male gonads. PLoS ONE. 2014;9(11):e113249. https://doi.org/10.1371/journal.pone.0113249.
Wishart DS, Jewison T, Guo AC, Wilson M, Knox C, Liu Y, et al. HMDB 3.0–the human metabolome database in 2013. Nucleic Acids Res. 2013;41(Database issue):D801–807. https://doi.org/10.1093/nar/gks1065.
Minai-Tehrani A, Jafarzadeh N, Gilany K. Metabolomics: a state-of-the-art technology for better understanding of male infertility. Andrologia. 2016;48(6):609–16. https://doi.org/10.1111/and.12496.
Jafarzadeh N, Mani-Varnosfaderani A, Minai-Therani A, Savadi-Shiraz E, Sadeghi MR, Gilany K. Metabolomics fingerprinting of seminal plasma from unexplained infertile men: a need for novel diagnostic biomarkers. Mol Reprod Dev. 2015;82(3):150. https://doi.org/10.1002/mrd.22457.
Gilany K, Moazeni-Pourasil RS, Jafarzadeh N, Savadi-Shiraz E. Metabolomics fingerprinting of the human seminal plasma of asthenozoospermic patients. Mol Reprod Dev. 2014;81(1):84–6. https://doi.org/10.1002/mrd.22284.
Josso N, Lamarre I, Picard JY, Berta P, Davies N, Morichon N, et al. Anti-mullerian hormone in early human development. Early Hum Dev. 1993;33(2):91–9. https://doi.org/10.1016/0378-3782(93)90204-8.
Andersen JM, Herning H, Witczak O, Haugen TB. Anti-mullerian hormone in seminal plasma and serum: Association with sperm count and sperm motility. Hum Reprod. 2016;31(8):1662–7. https://doi.org/10.1093/humrep/dew121.
Kucera R, Ulcova-Gallova Z, Windrichova J, Losan P, Topolcan O. Anti-mullerian hormone in serum and seminal plasma in comparison with other male fertility parameters. Syst Biol Reprod Med. 2016;62(3):223–6. https://doi.org/10.3109/19396368.2016.1161864.
La Marca A, Sighinolfi G, Radi D, Argento C, Baraldi E, Artenisio AC, et al. Anti-mullerian hormone (AMH) as a predictive marker in assisted reproductive technology (ART). Hum Reprod Update. 2010;16(2):113–30. https://doi.org/10.1093/humupd/dmp036.
Jensen TK, Andersson AM, Hjollund NH, Scheike T, Kolstad H, Giwercman A, et al. Inhibin B as a serum marker of spermatogenesis: correlation to differences in sperm concentration and follicle-stimulating hormone levels. A study of 349 danish men. J Clin Endocrinol Metab. 1997;82(12):4059–63. https://doi.org/10.1210/jcem.82.12.4456.
Wang Y, Suominen JS, Hakovirta H, Parvinen M, Martinand-Mari C, Toppari J, et al. Survivin expression in rat testis is upregulated by stem-cell factor. Mol Cell Endocrinol. 2004;218(1–2):165–74. https://doi.org/10.1016/j.mce.2003.11.028.
Weikert S, Schrader M, Muller M, Krause H, Miller K. Expression of the apoptosis inhibitor survivin in testicular tissue of infertile patients. Int J Androl. 2004;27(3):161–5. https://doi.org/10.1111/j.1365-2605.2004.00467.x.
Bailey R, Griswold MD. Clusterin in the male reproductive system: localisation and possible function. Mol Cell Endcrinol. 1999;151(1–2):17–23. https://doi.org/10.1016/s0303-7207(99)00016-7.
Zhijian H, Zengjun W, Gong C, Bianjiang L, Pengchao L, Jie L, et al. Presence, localization, and origin of clusterin in normal human spermatozoa. J Assist Reprod Genet. 2012;29(8):751–7. https://doi.org/10.1007/s10815-012-9779-x.
Ishikawa T, Fujioka H, Ishimura T, Takenaka A, Fujisawa M. Expression of leptin and leptin receptor in the testis of fertile and infertile patients. Andrologia. 2007;39:22–7. https://doi.org/10.1111/j.1439-0272.2006.00754.x.
Acknowledgements
Not applicable.
Funding
This work was supported by the National Natural Science Foundation of China [grant numbers 81973647] and Xinglin Scholar Research Premotion Project of Chengdu University of TCM [grant numbers QJJJ2021007].
Author information
Authors and Affiliations
Contributions
Junjun Li and Xujun Yu: conceived and wrote the article; Fang yang and Liang Dong: collected and provided the literatures and data for the article; Degui Chang: revised the manuscript critically for important intellectual content; All Authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Li, J., Yang, F., Dong, L. et al. Seminal plasma biomarkers for predicting successful sperm retrieval in patients with nonobstructive azoospermia: a narrative review of human studies. Basic Clin. Androl. 33, 9 (2023). https://doi.org/10.1186/s12610-023-00184-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12610-023-00184-0
Keywords
- Male infertily
- Non-obstructive azoospermia
- Surgical testicular sperm extraction
- Successful sperm retrieval
- Seminal plasma