
Abstract
Introduction
There have been public health concerns about a potential association between human papillomavirus (HPV) vaccines and premature ovarian failure (POF) in young women.
Objective
To identify a potential safety signal of POF after HPV vaccination using the United States (US) Vaccine Adverse Event Reporting System (VAERS) database.
Methods
We manually selected relevant MedDRA preferred terms related to POF and identified in VAERS all POF reports in women less than 40 years of age between 2 July 1990 and 14 May 2018, followed by a review of narratives to confirm the cases. We conducted descriptive analyses on age, POF type, HPV vaccine type (HPV2, HPV4, HPV9), time to onset of POF, and dose rank. We described trends in reporting over time and assessed a potential safety signal using the proportional reporting ratio (PRR).
Results
Of the 228,341 eligible POF reports, 281 (0.1%) were suspected to be associated with HPV vaccines. Median patient age was 15 years (range 11–39 years). POF events consisted mainly of amenorrhea (80.4%) and premature menopause (15.3%). Mean number of reported POF events significantly increased after the first HPV vaccine launch in 2006 with 22.2 POF cases/year up from 1.4 POF cases/year before the launch. PRR was 46.1 (95% confidence interval: 31.7–67.2) and sensitivity analyses yielded similar estimates.
Conclusion
Our study suggests the presence of a potential safety signal of POF associated with HPV vaccination, which may only be partly attributed to notoriety bias. Due to the well-known limitations of spontaneous reporting data, further investigations are warranted.
Similar content being viewed by others


Using a quantitative approach, this study uncovered a potential safety signal of POF following HPV vaccination. |
The large proportional reporting ratio (PRR) estimate obtained may not be entirely explained by reporting or notoriety bias, nor by the Weber effect. |
1 Introduction
Premature ovarian failure (POF) is the cessation of ovarian function before 40 years of age, with a possibility of ovarian function fluctuating (a state called primary ovarian insufficiency [POI]) before complete cessation [1]. The time between onset of altered menstrual cycle as an initial symptom and POF diagnosis is variable and may reach 5 years [2]. For young women POF has an important social and psychological impact, in addition to physiological consequences such as loss of bone mineral density amongst others [3]. POF is a rare condition with an estimated prevalence of 0.87 per 1,000,000 person-months (95% confidence interval (CI): 0.12–6.16) in 11- to 14-year-olds, and 4.08 per 1,000,000 person-months (95% CI: 1.70–9.79) in 15- to 18-year-olds [4]. About 74–90% of POF cases have an unknown etiology [1].
Concerns raised by the observations of cases of female infertility after human papillomavirus (HPV) vaccination emerged following the publication of two case series, respectively in 2013 and 2014, involving POF in 14- to 21-year-olds [1, 5]. Subsequently, safety statements on the absence of risk of infertility after HPV vaccination were made by the World Health Organization (WHO) Global Advisory Committee on Vaccine Safety (GACVS) as well as by the Centers for Disease Control and Prevention (CDC) and the US Food and Drug Administration (FDA) [6, 7]. In addition, a review of the POF cases reported to the United States (US) Vaccine Adverse Event Reporting System (VAERS) database was conducted. In this study there were 17 cases of POF identified, of which 15 were excluded because of insufficient information to confirm the diagnosis [8]. An observational study based on electronic health records (Vaccine Safety Datalink Study [VSD]) found no increased risk of POF after HPV vaccine, but was statistically underpowered [4]. Evidence of an association was also not supported in a recent cross-sectional study conducted using US NHANES data, which was, however, based on inaccurate measurement of POF and self-reported past HPV vaccination [9].
During the time period covered by our study, there were three HPV vaccine types on the US market: bivalent (HPV2), quadrivalent (HPV4), and nonavalent (HPV9). Our study used a pharmacovigilance approach to identify a potential safety signal of POF associated with HPV vaccination in VAERS by: (i) identifying reported cases of POF events suspected to be associated with HPV vaccination with no exclusion on the basis of missing data; (ii) describing the characteristics of POF cases and trends over time in event types, HPV vaccine type, time to onset of POF from HPV vaccination, dose rank, and age group; and (iii) determining whether there is a potential safety signal of POF related to HPV vaccination through a disproportionality analysis.
2 Methods
2.1 Data Source
We used the VAERS, created in 1990 in the US to fulfil a requirement of the National Childhood Vaccine Injury Act of 1986, which consists of a spontaneous and voluntary reporting system for any suspected adverse drug reaction (ADR) associated with vaccine use [10]. The system can receive reports of suspected ADRs from healthcare professionals, manufacturers, patients, parents, and caregivers [11]. The reporting form includes fields that capture information on the person who experienced the suspected ADR, the reporter, the suspected ADR, and the vaccine. Reports are coded using the Preferred Terms (PTs) of the Medical Dictionary for Regulatory Activities (MedDRA) [12]. Data from primary reports, after the removal of patient sensitive information, are publicly available on the VAERS website and through the CDC Wide Online Data for Epidemiologic Research (WONDER) tool. This database receives reports from both US and non-US sources; between 2011 and 2014, VAERS received an annual average of 30,000 US reports and 6,000 non-US reports, with the majority (> 99%) from vaccine manufacturers [10].
2.2 Eligibility Criteria
Relevant PTs for POF events were manually identified a priori by two medical doctors with respective expertise in vaccinology (CT) and pharmacovigilance (GC) using Standardized MedDRA Queries (SMQs) and examination of all PTs for either a symptom or a sign of POF. Events were divided into four categories: proportion of POF reports among HPV vaccine-associated reports, proportion of non-POF events in HPV vaccines, proportion of POF in other vaccines, and proportion of non-POF events in other vaccines. The denominator for proportions was restricted to women below 40 years of age or of unknown age between 2 July 1990 (i.e., the date an adverse event was first reported in VAERS) and 14 May 2018 (i.e., the date of data extraction). We defined exposure to HPV vaccination by the mention, in a case report, of an exposure of at least one dose of any HPV vaccine type (bivalent, quadrivalent, or nonavalent) for which the ADR was suspected to have occurred. Regardless of the vaccine reported, we excluded reports of cases aged ≥ 40 years, of unknown sex (analyzed only in a sensitivity analysis), and with known causes of POF with their corresponding MedDRA codes (vaginal septum [10064513], idiopathic hypogonadotropic hypogonadism [10059594], Turner’s syndrome [10045181], pregnancy [10036556], and polycystic ovaries [10036049]).
2.3 Study Outcomes
We assessed the following types of POF, with corresponding MedDRA codes: amenorrhea (10001928), oligomenorrhea (10030295), premature menopause (10036601), ovarian failure (10033165), blood follicle-stimulating hormone increased (10005534), blood follicle-stimulating hormone abnormal (10005532), estradiol decreased (10030229), and estradiol abnormal (10063266). In addition, the narrative of each case was reviewed to confirm that the amenorrhea was not due to pregnancy.
2.4 Data Analysis
We used frequencies and percentages to describe reports of POF associated with HPV vaccination, according to patient age, time between vaccination and onset of POF event, POF event type, HPV vaccine type (HPV2, HPV4, HPV9), dose rank, time period, and region (whether US or non-US). An analysis of all POF events (regardless of the suspected vaccine) was also undertaken in order to compare the annual number of POF case reports in the period before the launch of the first HPV vaccine (1990–2006) to the annual number post-launch (2006–2018) and used Fisher’s exact test to assess the statistical significance of the differences.
Disproportionality was evaluated using the proportional reporting ratio (PRR), which is the ratio of the proportion of reports of POF events suspected to be associated with HPV vaccination to the proportion of reports of POF events suspected to be associated with all other vaccination in women age < 40 years or unknown age only [13]. The criteria for a signal of disproportionality were set at a PRR ≥ 2, the lower bound of the 95% CI for the PRR ≥ 1, and the number of cases ≥ 3 [14]. We conducted the following sensitivity analyses on the PRR: (i) inclusion of reports of unknown sex below 40 years of age; (ii) stricter definition of POF event (restricted to amenorrhea, premature menopause, and ovarian failure); (iii) exclusion of cases of unknown age; and (iv) restriction of the time period to post-launch only (July 2006–14 May 2018).
3 Results
3.1 Reports of Premature Ovarian Dysfunction in Vaccine Adverse Event Reporting System (VAERS)
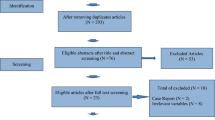
Figure 1 shows the flow of selection of reports, including reasons for exclusion. There were 228,341 AE reports for females less than 40 years of age or of unknown age recorded in the VAERS database between 2 July 1990 and 14 May 2018. Of those, 311 (0.14%) were POF events. Among the 311 POF cases, 281 (90.4%) were exposed to HPV vaccination (hence, were recorded in VAERS following the launches of the vaccine starting in 2006) and 30 (9.6%) were exposed to another vaccine. Of those 30, 23 (76.7%) occurred prior to 2006 and seven (23.3%) occurred thereafter. Meanwhile, of the 228,030 cases of other AEs, 78,220 (34.3%) were reported prior to 2006 and 149,810 (65.7%) were reported thereafter, of which 38,276 (25.6%) were exposed to HPV vaccination while 111,534 (74.5%) were exposed to another vaccine.

Flow diagram of identification of eligible reports for the study. POF premature ovarian failure, AE adverse event, HPV human papilloma virus. aSome cases were counted for more than one reason of exclusion
3.2 Characteristics of Cases of Premature Ovarian Failure (POF) Suspected of Being Associated with Human Papillomavirus (HPV) Vaccination or Other Vaccination
The characteristics of the 281 POF events following HPV vaccination are described in Table 1. The median age of patients was 15 years at the time of reporting (range: 11–39 years). Over half of the cases (58.0%) were in the younger age group (< 20 years) and age was unknown for a large portion (27.0%). Time to onset of POF events after the date of HPV vaccine exposure was documented in 128 (45.6%) of cases; median was 20.5 days and ranged from 0 to 2,017 days (0–5.5 years). The great majority of cases (84.3%) had received the quadrivalent vaccine (HPV4), which was the first introduced on the US market in 2006. There were eight types of POF events, which were not mutually exclusive and fell into either clinical or laboratory notifications: amenorrhea accounted for the majority of cases (80.4%), followed by premature menopause (15.3%). In addition, laboratory findings were available for only a minority of cases; 5.0% of cases for blood follicle-stimulating hormone increased, 1.4% cases for estradiol decreased, and, 0.4% cases each for blood follicle-stimulating hormone abnormal and estradiol abnormal.
In relation to POF reports suspected to be associated with other vaccines between 1990 and 2018, there were 30 reports, out of which 23 (76.7%) had data for age with a median of 25 years (range: 12–38 years). There were 21 (70.0%) reports with data on duration from exposure to other vaccines to POF onset with a median of 11 days (range: 0–1951 days). Only four POF event types were recorded, with the majority being amenorrhea in about 83.3% (25/30) of cases, while the rest were premature menopause (3.3%, one report), oligomenorrhoea (10.0%, three reports), and decreased estradiol level (3.3%, one report). There were about 17 other vaccines suspected to be linked to these 30 POF reports, which were: measles vaccine (one report), hepatitis B vaccine (nine reports), measles, mumps, and rubella vaccine (four reports), varicella virus live vaccine (four reports), tetanus and diphtheria toxoids vaccine (one report), tetanus toxoid (one report), Lyme disease vaccine (one report), rabies virus vaccine (one report), hepatitis A vaccine (one report), anthrax vaccine (three reports), trivalent influenza virus vaccine (two reports), quadrivalent influenza virus vaccine (one report), inactivated polio vaccine (one report), meningococcal group B vaccine (one report), tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis vaccine (one report), meningococcal conjugate vaccine (A,C,W-135,Y) (one report), and tick-borne encephalitis vaccine (one report).
3.3 POF Cases Before and After the Introduction of HPV Vaccines on the Market
Out of the 311 reports of POF events, 288 (92.6%) were reported in the time period after the first introduction of the HPV vaccine (i.e., 2006), while 23 (7.4%) were reported before its introduction (Table 2). As shown in Table 3, out of 288 reports of POF events in 2006–2018, the great majority (97.6%) were suspected to be associated with HPV vaccination, while only seven (2.4%) were suspected to be associated with other vaccines. There was a statistically significant shift in age distribution after the introduction of HPV vaccines: In the period after the introduction of HPV vaccine on the US market (2006–2018), more than half (57.3%) of the 288 POF cases were of the younger age group (< 20 years) and age was unknown for a large portion (27.1%), while in the period before the introduction, about one-quarter (26.1%) of the 23 cases found were aged less than 20 years.
The age distribution of POF associated with HPV vaccines versus other vaccines was heterogeneous (p = 0.03523); the majority of women with HPV vaccine-associated POF were less than 20 years of age (58.0%), while there was no clustering in specific age groups for the other vaccines (Table 3).
As shown in Table 4, the distribution of POF reports by age group was homogenous across vaccine types (HPV2, HPV4, HPV9) (p = 0.3081), while the distribution of dose rank by vaccine type was heterogeneous (p = 0.03723). Heterogeneity of the latter was due to differences in the proportion of reports with unknown dose rank. Overall, before the introduction of the HPV vaccine, the mean number of POF reports was 1.4 cases per year (accounting for 23 cases for other marketed vaccines), and following the introduction, it increased to 22.2 cases per year (accounting for 288 cases for both HPV vaccine and other vaccines) (p < 0.0001). After the introduction of the HPV vaccines, 21.6 cases suspected of being associated with HPV vaccine per year were reported, while 0.5 cases suspected of being associated with other vaccines per year were reported. As shown in Fig. 2, the number of POF reports suspected to be associated with HPV vaccination (n = 281) following the market launch of the HPV vaccine in 2006 has been increasing over time, with a peak occurring in July 2016.

Trend over time of reports of POF after market launch of the first HPV vaccine. POF premature ovarian failure, HPV human papilloma virus
3.4 Proportional Reporting Ratio
The distribution of adverse events (AEs) according to type (POF vs. other AEs) and vaccination status (HPV vaccines vs. other vaccines) is reported in Table 5. Using these counts the PRR was estimated at 46.1 (95% CI: 31.7–67.2).
An arbitrary time window of a 1-year interval was used and any POF event occurring within 30 days after HPV or other vaccination was not suspected to be associated with the vaccine. For HPV vaccination, a cluster distribution for the 45.6% (128/281) HPV vaccine-related POF reports with data on time to onset was observed. The reporting period 31 days to 1 year from HPV vaccination was registered in 32.0% (41/128) of POF cases (Fig. 3). On the other hand, the cluster distribution of POF cases suspected to be associated with other vaccines, of which 70.0% (21/30) reported data on time to onset, involved (28.6% [6/21]) reports that fell within 31 days to 1 year. It is not known if time to onset is from the first, second, or third dose of the vaccine. The risk window of 31 days to 1 year was also applied to other vaccine proportions.

Time to onset for POF reports following HPV vaccination. POF premature ovarian failure, AE adverse event, HPV human papilloma virus
3.5 Sensitivity Analysis on the Proportional Reporting Ratio
The first sensitivity analysis included the 80,133 cases (14 POF events and 80,119 other AEs) of unknown sex and age below 40 years. Assuming that these cases might have been women (conservative approach), the sensitivity analysis yielded a PRR estimate of 52.6 (95% CI: 36.2–76.6). When cases of POF events were restricted to amenorrhea, premature menopause and ovarian failure, the reports decreased by only 6.4% (PRR 50.2; 95% CI: 33.6–75.0). The third sensitivity analysis involving the exclusion of reports of unknown age yielded a PRR estimate of 47.4 (95% CI: 30.9–72.9). In the final sensitivity analysis, the time period was restricted to the period following market launch of the first HPV vaccine (i.e., July 2006 to 14 May 2018), and the PRR estimate was more than double its initial estimate at 112.6 (95% CI: 53.4–238.3). The observed peak in reporting that occurred in 2016 may be the result of notoriety bias. An additional sensitivity analysis was thus conducted excluding the 47 cases reported in 2016, and the PRR remained high at 38.4 (95% CI: 26.3–56.2).
4 Discussion
Using the US VAERS data, a high disproportionality in the reports was found, which suggests the presence of a potential signal of an association between HPV vaccine and POF events. To address some of the limitations of spontaneous data, such as missing data in the reports, namely unknown sex or age, sensitivity analyses were conducted, which yielded similar results of disproportionality. Applying a stricter definition of POF (amenorrhea, premature menopause, ovarian failure) or restricting the time period post-launch of HPV vaccines, the PRRs increased, but as shown by very broad 95% CIs, the estimates were very imprecise. In relation to sensitivity analysis involving unknown sex, even if the 14 POF events were assigned to females and the 80,119 other events to males, the signal was still present. It is worth noting that histological findings on gonad functioning of male rats after HPV vaccination was normal in preclinical trials [15], which confirms that the sensitivity analysis on unknown sex yielded conservative estimates of the PRR.
This high PRR estimate, which meets the threshold of a lower bound of 95% CI ≥1, and number of reports ≥3 supports the evidence generated from published case reports and case series on the potential association between HPV vaccine and POF subsequent to declining menstrual function in girls aged between 14 and 21 years [1, 5]. The observed increase in POF events reported in the VAERS after the first HPV vaccine introduction (2006) should be interpreted with caution as the reporting of ADRs is known to be influenced by the novelty of the product [16].
There were 281 reports of HPV vaccine and POF events following the first approval (in 2006) till 14 May 2018, and reports significantly increased among adolescents below 20 years of age as expected due the indicated age to vaccinate against HPV and peak coverages in the female population [17,18,19,20]. This is consistent with the age of patients reported in the published case series [1, 5], with a mean of 16.5 years. Using an arbitrary time frame of POF onset date, this study showed that almost a third of POF reports with time of onset fell within 31 days to 1 year, a period that might be of concern. The majority of reports of POF associated with HPV vaccination cited HPV4 as the suspected vaccine type. These results were expected as the HPV4 vaccine contributed the most doses since approval from June 2006 till present (at least 60 million doses distributed in the US compared to at least 720,000 doses for HPV2 and at least 28 million for HPV 9 distributed in the US) [7]. While published case series described cases that received HPV4 vaccines only, the current study identified reports of POF events not only for HPV4 vaccine but also for HPV2 and HPV9 vaccines, even if substantially less. It is important to note that the case series referred to were published in 2013 and 2014, respectively, at the time when both HPV2 and HPV4 were already on the market [1, 5]. Also, the study showed that among the 281 reports, POF events were suspected of HPV vaccine irrespective of dose rank. Cases where POF occurred following the first, second, or third dose could not be reliably derived from VAERS.
The use of amenorrhea as a proxy for POF identification is supported by the fact that it is the main initial symptom in women with POF [2], which was also the main observed POF in our data (i.e., 80.4% of 281 reports). However, only few reports referred to ovarian failure (6.4%) and premature menopause (15.3%) as well as recorded increased follicle-stimulating hormone level (5.0%) and decreased estrogen hormone level (1.4%). Acknowledging the fact that events of declining menstrual function after HPV vaccine are unexpected AEs with apparent lack of research in pre- and post-licensing studies, little or no efforts by clinicians in actual practice to follow up patients after vaccination is expected. This may lead to incomplete ascertainment of ovarian failure and supporting laboratory investigations in the spontaneous reports. This under-reporting in the real-world setting ties with findings from post-licensing HPV vaccine safety studies based on claims data [21] as well as others that were not able to recognize them as serious AEs [22, 23]. Thus, pharmacoepidemiological studies based on data sources including information about vaccination, events, and potential confounders at patient level are required by using large cohorts and a long duration of follow-up.
Following the published case series, the CDC and FDA addressed public concerns on POF after HPV vaccination through a VAERS review and a Vaccine Safety Datalink study. According to the VAERS review, there were three reports among 29 million doses of HPV9 vaccine administered in the population (1 December 2014–31 December 2017) [7]. All three were determined as unconfirmed (lacking sufficient information to confirm a diagnosis of POI). Among 17 reports following 60 million HPV4 vaccine doses (January 2006–2015), two had a physician diagnosis of POF, whereas the remaining 15 did not have enough information to confirm the diagnosis. Upon further causality assessment of physician-diagnosed POFs, an association with HPV4 vaccine was deemed unlikely. The impact of POF being an unexpected AE may explain the dismissal of reports as hearsay. In the Vaccine Safety Datalink study, among 199,078 girls aged 9–26 years who had been vaccinated with the HPV vaccine, only one confirmed case of POF was found, leading to no increased risk [4]. The study acknowledged that it was underpowered to detect small increases in POI risk associated with vaccination. Also, apart from absolute measures, estimations of the relative risk using as reference unvaccinated patients or periods free of vaccination would provide information of the association between HPV vaccination and POF.
In the literature, biological plausibility may be possible either through toxicity or autoimmune mechanism. Both the aluminum- and non-aluminum-containing HPV vaccines contain polysorbate 80. One study noted that newborn rats injected with polysorbate 80 experienced similar ovarian damage to those injected with diethylstilbestrol, affecting ovaries across all doses tested over a tenfold range [24, 25]. Nevertheless, like quantitative signal detection methods, the association found in this study may be due to chance. Hence, it is required that it is followed up with a more robust methodology, which might further investigate the effect of polysorbate 80 as an autoimmune hypothesis. However, other vaccines contain polysorbate 80, such as vaccines against rotavirus, pneumococcal and meningococcal diseases, diphtheria, tetanus, pertussis, influenza, hepatitis A and B, and poliomyelitis [26]. It is possible, however, that they tend to be administered mostly to babies or to the elderly, and these people may not be at risk of POF.
This study appears to be the first to quantitatively identify a potential safety signal of disproportionate reporting of POF events following HPV vaccination using a spontaneous reporting database (VAERS). VAERS is a national database that covers over 300 million inhabitants, supplemented by non-US cases that may also be reported. Such a large coverage also enables the detection of rare adverse events, including POF events. More specific to VAERS is the length of coverage, as data are available since its inception in 1990, which allows the investigation of safety reports of HPV vaccines from the time they were launched on the market.
4.1 Study Limitations
Like all spontaneous reporting systems, VAERS is prone to reporting bias, which includes the under-reporting of AEs, especially for those with delayed onset, such as POF. Despite the likely under-reporting, a strong safety signal was uncovered in this study. Hence, more cases included may not have changed the conclusions. However, differential under-reporting, i.e., more reporting of POF cases for HPV vaccines compared to other vaccines, may have spuriously inflated the strength of the signal. Greater reporting of POF cases associated with HPV vaccines may have been caused by the novelty of the vaccine compared to the other vaccines, or by media/literature coverage, as found for other products [27]. Such an increase may have been due to greater scrutiny in the time period following marketing of new vaccines, referred to as the Weber effect [16], or following the publication of the VSD study in 2014 [4]. This is unlikely because the number of cases has remained fairly stable in the time period following launch, while acknowledging the fact that the increase was attributable to non-US cases as trends over time in US cases plateaued during this time period. In addition, the sensitivity analysis excluding the peak of reports in 2016 still yielded a large PRR. Though manufacturers make up greater than 99% of non-US reports [10], it is not known how many countries have contributed to non-US cases overtime. A Weber effect would be associated with an increase immediately after launch followed by a decrease over time in the number of reports. The increase in the number of reports following the launch of HPV vaccines could be due to the characteristics of the target population for the HPV vaccines (young women) rather than a vaccine effect. In fact, more contact with the healthcare system would occur due to the vaccination and therefore increase the probability of detecting POF. Concerning non-US reports, a greater majority come from manufacturers in compliance with an FDA requirement, which may lead to differences in the types of events reported and the information provided in the reports (information bias) [10]. However, with under-reporting of cases being the main concern, reporting by manufacturers is of little concern for this particular study. As of 1 May 2017 the HPV4 vaccine has no longer been available, leaving the HPV9 vaccine as the only vaccine being distributed in the USA after its recommendation by the US Advisory Committee on Immunization Practices in 2014 [28]. With the HPV4 vaccine, the vaccine type registered in the majority of POF reports, no longer in circulation in the market, it is reasonable to expect a drop in POF reports after 2016.
There was a variability in the quality and completeness of POF case reports, such as absence of information on follicle-stimulating hormone and estrogen hormone levels in the majority of the reports. Incomplete data call into question whether or not the identified reports for HPV vaccine and POF events are actually valid cases, with POF as the true diagnosis. Finally, VAERS cannot be used to determine whether a vaccine caused an AE as it could be due to chance, confounders, or bias. Therefore, this study only generated the hypothesis that there may be a signal of disproportionate reporting for POF events and HPV vaccine that warrants further investigation.
5 Conclusion
This study has detected a strong disproportionality in the reporting of POF events after HPV vaccine in VAERS. Besides amenorrhea, which is the most frequently mentioned POF event, other events such as ovarian failure, premature menopause, oligomenorrhea, and blood follicle hormone and estrogen hormone levels were also reported. These findings along with other sources of evidence such as the published case series and the biological plausibility lend support to the presence of a safety signal. The public has been reassured by health authorities of the absence of a causal relationship between HPV vaccine and POF not only based on safety studies that lacked data on ovarian dysfunction but also on those studies with sources of data that were insufficiently powered to detect events of declining ovarian function. With an increase in the uptake of HPV vaccination programs in more countries, the population of adolescent girls (9–16 years) at risk of potential ovarian dysfunction after HPV vaccination is increasing and combined with the significant negative consequences on future health and prospects of motherhood, this signal warrants well-designed and appropriate epidemiological research. If the signal is confirmed, the risk is small compared to the lifetime risk of cervical cancer, especially in developing countries. The population-based benefit-risk will always be very high. However, on an individual basis, the vaccinee needs to be made aware as POF may not be of minor importance for everyone, and the benefit-risk of vaccination regarding the risk of POF versus cervical cancer would need to be assessed differently in each situation.
References
Little DT, Ward HRG. Adolescent premature ovarian insufficiency following human papillomavirus vaccination: a case series seen in general practice. J Investig Med High Impact Case Rep. 2014;2(4):12. https://doi.org/10.1177/2F2324709614556129.
Alzubaidi NH, Chapin HL, Vanderhoof VH, Calis KA, Nelson LM. Meeting the needs of young women with secondary amenorrhea and spontaneous premature ovarian failure. Obstet Gynecol. 2002;99(5 Pt 1):720–5.
Kovanci E, Schutt AK. Premature ovarian failure: Clinical presentation and treatment. Obstet Gynecol Clin N Am. 2015;42(1):153–61.
Naleway A, Mittendorf K, Irving S, Henninger M, Crane B, Smith N, Daley MF, Gee J. Primary ovarian insufficiency and adolescent vaccination. Pediatrics. 2018;142(3): e20180943. https://doi.org/10.1542/peds.2018-0943.
Colafrancesco S, Perricone C, Tomljenovic L, Shoenfeld Y. Human papilloma virus vaccine and primary ovarian failure: another facet of the autoimmune/inflammatory syndrome induced by adjuvants. Am J Reproduct Immunol. 2013;70(4):309–16.
WHO. Weekly Epidemiological Record (WER). World Health Organization. 2017. http://www.who.int/wer. Accessed 31 March 2021.
CDC. Questions about HPV Vaccine Safety. In: Vaccine Safety. Centers for Disease Control and Prevention. 2020. www.cdc.gov/vaccinesafety/vaccines/hpv/hpv-safety-faqs.html#A6. Accessed 31 March 2021.
Arana JE, Harrington T, Cano M, et al. Post-licensure safety monitoring of quadrivalent human papillomavirus vaccine in the Vaccine Adverse Event Reporting System (VAERS), 2009–2015. Vaccine. 2018;36:1781–8.
Schmuhl NB, Mooney KE, Zhang X, Cooney LG, Conway JH, LoConte NK. No association between HPV vaccination and infertility in U.S. females 18–33 years old. Vaccine. 2020;38(24):4038–43. https://doi.org/10.1016/j.vaccine.2020.03.035.
Shimabukuro TT, Nguyen M, Martin D, DeStefano F. Safety monitoring in the Vaccine Adverse Event Reporting System (VAERS). Vaccine. 2015. p. 4398–405.
Tanzi MG. CDC and FDA launch VAERS 2.0. Pharm Today [Internet]. Elsevier; 2017 Aug 1 [cited 2018 Sep 14];44. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1042099117311854.
Brown EG, Wood L, Wood S. The medical dictionary for regulatory activities (MedDRA). Drug Saf. 1999;20:109–17.
Härmark L, Van Grootheest AC. Pharmacovigilance: methods, recent developments and future perspectives. Eur J Clin Pharmacol. 2008;64:743–52.
European Medicines Agency. Guideline on the use of statistical signal detection methods in the eudravigilance data analysis system. In: Evaluation of Medicines for Human Use. European Medicines Agency. 2006. https://www.ema.europa.eu/en/documents/regulatory-procedural-guideline/draft-guideline-use-statistical-signal-detection-methods-eudravigilance-data-analysis-system_en.pdf. Accessed 31 Mar 2021.
Wise LD, Pauley CJ, Michael B, Wolf JJ. Lack of effects on male fertility from a quadrivalent HPV vaccine in Sprague-Dawley rats. Birth Defects Res Part B Dev Reprod Toxicol. 2010;89:376–81.
Arora A, Jalali RK, Vohora D. Relevance of the Weber effect in contemporary pharmacovigilance of oncology drugs. Ther Clin Risk Manag. 2017;13:1195–203.
Merck. Gardsil Package Insert. Food and Drug Administration. 2015. https://www.fda.gov/files/vaccines,blood&biologics/published/Package-Insert---Gardasil.pdf. Accessed 31 Mar 2021.
Merck. Gardasil 9 Package Insert. Food and Drug Administration. 2020. https://www.fda.gov/media/90064/download. Accessed 31 Mar 2021
Glaxosmithkline. Cervarix Package Insert. Food and Drug Administration. https://www.fda.gov/media/78013/download. Accessed 31 Mar 2021.
Bruni L, Diaz M, Barrionuevo-Rosas L, Herrero R, Bray F, Bosch FX, Sanjose SD, Castellsague X. Global estimates of human papillomavirus vaccination coverage by region and income level: a pooled analysis. Lancet Glob Health. 2016;4(7):e453–63. https://doi.org/10.1016/S2214-109X(16)30099-7.
Klein NP, Hansen J, Chao C, Velicer C, Emery M, Slezak J, Lewis N, Deosaransingh K, Sy L, Ackerson B, Cheetham C, Liaw K-L, Takhar H, Jacobsen SJ. Safety of quadrivalent human papillomavirus vaccine administered routinely to females. Arch Pediatr Adolesc Med. 2012;166(12):1140–8.
Arnheim-Dahlström L, Pasternak B, Svanström H, Sparén P, Hviid A. Autoimmune, neurological, and venous thromboembolic adverse events after immunisation of adolescent girls with quadrivalent human papillomavirus vaccine in Denmark and Sweden: Cohort study. BMJ. 2013;347: f5906. https://doi.org/10.1136/bmj.f5906.
Bonanni P, Cohet C, Kjaer S, Latham N, Lambert P, Reisinger K, Haupt RM. A summary of the post-licensure surveillance initiatives for GARDASIL/SILGARD. Vaccine. 2010;28(30):4719–30.
Little D. Response to the fourth Brighton Collaboration Journal Club reviews on BMJ case presentation by Little DT and Ward HRG. http://u.b5z.net/i/u/16000121/f/Author_Little_DT_Response_to_4th_Brighton_Collaboration_Journal_Club.pdf. Accessed 31 March 2021.
Gajdova M, Jakubovsky J, Valky J. Delayed effects of neonatal exposure to Tween 80 on female reproductive organs in rats. Food Chem Toxicol. 1993;31(3):183–90.
CDC. Vaccine Excipient Summary-Excipients Included in U.S Vaccines. Centers for Disease Control and Prevention. 2020. https://www.cdc.gov/vaccines/pubs/pinkbook/downloads/appendices/b/excipient-table-2.pdf. Accessed 31 Mar 2021.
Langlade C, Gouverneur A, Bosco-Levy P, et al. Adverse events reported for Mirena levonorgestrel-releasing intrauterine device in France and impact of media coverage. Br J Clin Pharmacol. 2019;85:2126–33.
CDC. What's New with VISs. In: Vaccine Information Statements (VISs). Centers for Disease Control and Prevention. 2017. https://www.cdc.gov/vaccines/hcp/vis/what-is-new.html. Accessed 31 Mar 2021.
Acknowledgements
No funding was received for the conduct of this study. Collins Tatang (CT) was on a Master Scholarship program in Vaccinology and Pharmaceutical Clinical Development at the University of Siena, Italy funded by Fondazione Sclavo. We thank Dr. Genaro Castillon (GC) from YOLARX Consultants for his valuable advice and contribution to the analysis of VAERS data.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Collins Tatang, Yola Moride, Teigna Arredondo Bisonó, Aurore Bergamasco, Sue Ann Costa Clemens, and Francesco Salvo have no conflicts of interest to declare.
Ethics approval
This study did not require prior ethics approval because the data set is publicly available without restriction via the Centers for Disease Control and Prevention website.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and material
The datasets used for this study are available at https://vaers.hhs.gov/data.html.
Code availability
Not applicable.
Author contributions
Collins Tatang and Yola Moride conceived and designed the study; Collins Tatang prepared the original draft of the paper, Yola Moride carried out supervision, Collins Tatang and Teigna Arredondo Bisonó extracted and analyzed data. All authors reviewed the various drafts of the manuscript. All authors reviewed and approved the final manuscript.
Appendix 1- Sensitivity analyses
Appendix 1- Sensitivity analyses
1.1 Distribution of adverse events in women aged below 40 years with inclusion of unknown sex
Adverse events | |||
|---|---|---|---|
POF events | Other AEs | Total | |
HPV vaccination | 295 | 48,172 | 48,467 |
Other vaccinations | 30 | 259,441 | 259,471 |
Total | 325 | 307,613 | 307,938 |
1.2 Distribution of adverse event reports using a restricted definition of POF (amenorrhea, premature menopause, and ovarian failure)
Adverse events | |||
|---|---|---|---|
POF events | Other eventsa | Total | |
HPV vaccination | 265 | 38,292 | 38,557 |
Other vaccinations | 26 | 189,758 | 189,784 |
Total | 291 | 228,050 | 228,341 |
1.3 Distribution of adverse event reports excluding reports of unknown age
Adverse events | |||
|---|---|---|---|
POF events | Other events | Total | |
HPV vaccination | 205 | 31,588 | 31,793 |
Other vaccinations | 23 | 168,991 | 169,014 |
Total | 228 | 200,579 | 200,807 |
1.4 Distribution of adverse events in women below 40 years of age stratified by POF events and other events among exposure and non-exposure to HPV vaccination between 1 July 2006 and 14 May 2018
Adverse events | |||
|---|---|---|---|
POF events | Other AEs | Total | |
HPV vaccination | 281 | 38,276 | 38,557 |
Other vaccinations | 7 | 108,139 | 108,146 |
Total | 288 | 146,415 | 146,703 |
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Tatang, C., Arredondo Bisonó, T., Bergamasco, A. et al. Human Papillomavirus Vaccination and Premature Ovarian Failure: A Disproportionality Analysis Using the Vaccine Adverse Event Reporting System. Drugs - Real World Outcomes 9, 79–90 (2022). https://doi.org/10.1007/s40801-021-00271-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40801-021-00271-6