
Abstract
Introduction
Musculoskeletal pain (MP) is prevalent in our society, having a strong negative impact on physical and psychosocial quality of life. Heat therapy (HT) has been frequently described as a treatment strategy for musculoskeletal pain, but scientific evidence is still poor. The aim of the present Delphi method study is to gather a consensus among European experts on the role of HT in MP.
Methods
To address this topic, a list of 54 statements was developed, concerning mechanism of action of heat on muscle, types of MP eligible for heat treatment, efficacy of HT, time and modalities of treatment, maximizing compliance to HT, safety (based on heat wraps), wrong beliefs and common errors in the prescription of HT and the role of HT in preventing muscular damage in athletes. The survey was distributed to 116 European experts, using a 5-point Likert scale to express agreement or disagreement with the statements; 66% concordance with the statements was needed to define a consensus.
Results
Consensus was reached on 78% of statements. There was a strong consensus on the mechanism of action of heat on muscle, the indication in chronic MP, its effectiveness as part of a multimodal approach to MP and the safety and tolerability of superficial heat therapy. A low-level of consensus was obtained on the role of heat in preventing muscular damage and in acute MP.
Conclusion
This Delphi consensus recognizes the role of HT mostly in chronic MP and highlights the need for stronger scientific evidence to regulate the use of this therapy in clinical practice.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Heat therapy is commonly used in clinical practice for musculoskeletal pain, but scientific consensus on its use is still missing. |
This Delphi consensus recognizes the role of heat therapy mostly in chronic musculoskeletal pain. |
This study highlights the need for stronger scientific evidence on heat therapy. |
Introduction
Musculoskeletal pain (MP) affects > 30% of global population and can lead to significant functional disability and emotional distress [1]. MP can be acute or chronic (when it last or recurs for > 3 months), focal or diffuse. MP can occur with no identifiable structural cause or can be secondary to underlying tissue damage or disease, affecting bones, joints, muscles and/or related soft tissues [2].
Referring to the Global Burden of Diseases in 2010, MP is a major burden in our society, with low back pain the primary cause. Unfortunately, there is still a mismatch between the burden of MP conditions and an appropriate health policy response [3].
Heat is one of the oldest treatment methods known in medicine. Its use has been described for centuries for several diseases, pain being one of the most traditional [4, 5]. Heat therapy (HT) represents a non-pharmacological treatment approach and is defined as the application of an external source of heat to a specific body area to increase the tissues’ temperature [6, 7]. Topical application of heat does not induce any change in “core temperature” [8]. Physiological effects of heat on tissues are vasodilatation, increased blood flow, increased metabolism, increased inflammation, increased extensibility, activating the transient receptor potential (TRP) channel and reducing pain [6].
HT can be applied either superficially or deeply, and it can be delivered by three different mechanisms: conduction, convection and conversion [6]. In clinical practice, heat can be provided in a variety of forms, including superficial heat pads or wraps, hot baths, heat lamps, ultrasounds and diathermy [6]. Some of these treatment modalities are limited to the hospital setting (e.g., ultrasound and diathermy), while others, such as continuous superficial low-level heat therapy, can be easily provided at home.
HT is part of the multimodal approach in the treatment of MP. Evidence of its efficacy is reported in spinal (low back and neck), knee and wrist pain and delayed-onset muscle soreness (DOMS) [7, 9].
Despite its frequent use in clinical practice, scientific evidence available on this topic is still limited, and no general guidelines exist.
The aim of the present study is to gather a consensus of experts on the role of HT in the treatment of MP and to generate clinical insights on the common use of HT, in particular superficial heat therapy.
We used a Delphi methodology to elaborate a consensus among a group of European physicians and physical therapists specialized in heat therapy in MP.
Methods
The Delphi methodology aims to facilitate the achievement of a consensus on a specific topic in a group of experts through an anonymous questionnaire where a panel of experts must express their agreement or not with specific statements on the topic under discussion [10,11,12].
The present study consisted in a modified Delphi method, which took place between September and November 2021. Considering the international nature of the participants, the study was conducted in English. An English online survey was developed by a European panel of nine experts on MP, hereafter referred to as key opinion leaders (KOLs), who were selected based on their previous experience in heat therapy. In particular, the KOL panel was composed by three rheumatologists, two sports medicine physicians, one family medicine physician, one physiotherapist and two physiatrists. The KOLs performed an extensive review of current literature on heat therapy on PubMed. Although not systematic, the KOLs believe that the literature review performed included the main available evidence. This literature review represents the basis for the identification of 8 topics and 54 statements by the KOLs aiming to evaluate the role of HT in the management of MP. The topics were: mechanism of action of heat on muscle, types of MP eligible for heat treatment, efficacy of HT, time and modalities of heat treatment, maximizing compliance to HT, safety of HT (based on heat wraps), wrong beliefs and common errors in the prescription of HT, and role of HT in preventing muscular damage in athletes (see Table 1). Once developed, the questionnaire was distributed online to 94 experts on MP, who were asked to rate their agreement or not to each statement, using a 5-point Likert scale where 1 = “strongly disagree” and 5 = “strongly agree.” The answers were collected anonymously and analyzed by the KOLs. In this study, a sum of 1–2 points was considered “negative consensus” while a sum of 3–5 points was considered “positive consensus” [13].
The panelists were selected base on their expertise in the topic, with the aim to equally distribute the questionnaire in terms of specialties and country. A cutoff of 66% of agreement/disagreement for each statement was necessary to define a consensus [13]. No consensus was reached if a statement received < 66% of concordant replies.
Descriptive statistics were used to analyze the results. Absolute numbers, percentage, media and standard deviation were the only statistical analyses performed. This study did not involve human participants or any patient data. Therefore, no ethical approval was needed.
Results
Degree of Consensus in the Delphi Process
Seventy-six participants responded to the questionnaire, with a response rate of 80% (76/94). Geographic distribution of the responders was 36 from Spain, 6 from Italy, 6 from Germany, 14 from Austria and 14 from Portugal. No further analysis of the panelists was performed, given the anonymous nature of the Delphi methodology.
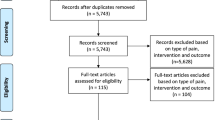
In the questionnaire, consensus was obtained for 78% (42/54) of statements; of these, 93% (39/42) were positive and 7% (3/42) were negative consensus (Fig. 1).

Delphi survey flowchart
No consensus was reached on 12 statements (22%) but no second round was proposed because the KOLs considered this lack of consensus secondary to the lack of concordant scientific evidence.
Table 2 summarizes the statements and percentage of agreement/disagreement for each statement.
Main topics are separately analyzed below
Mechanism of Action of Heat on Muscle
The panelists strongly agree that heat improves muscle flexibility (95%), increases blood flow and metabolism (100%) and can contribute to the healing process (91%). As the physiological mechanism of pain, the panelists strongly agree that heat application activates temperature-sensitive nerve endings (thermoreceptors), which in turn initiate signals that block the processing of nociceptive signals (91%), and agreed that the pressure used to apply some superficial heat therapy may activate proprioceptors, which in turn block the processing of nociceptive signals (75%).
The panelists did not reach a consensus on the statement “supplemental heat can improve muscle strength during physical activity” with 3% final agreement.
Types of Musculoskeletal Pain Eligible for Heat Treatment
The panelists strongly agreed that HT may be indicated in non-specific low back pain (95%) and chronic nociceptive pain (93%), whereas it is not indicated in acute inflammatory joint pain (95%). Mild to moderate consensus was obtained for the indication of heat therapy in tendinosis (80%), DOMS (83%), osteoarthritis (78%) and mechanical pain (83%). Moreover, 86% of participants agreed that HT “may be indicated in strain and sprain during the chronic phase of rehabilitation (or after the acute phase of rehabilitation).”
No consensus was reached on the indication of HT in acute nociceptive pain (percentage of agreement: 66%).
Efficacy of Heat Therapy
For this topic, consensus was reached for all statements. Panelists strongly agreed that superficial heat therapy “has a short-term effect on pain relief” (92%) and “can reduce the need of analgesics” (93%). There was also a consensus that superficial heat therapy “can contribute to a long-term effect if integrated in a multimodal approach to pain” (88%), “can reduce disability in low back pain” (87%), “improves daily living activities” (78%) and “can prevent worsening of low back pain” (70%).
Time and Modalities of Heat Treatment
For this topic, statements were divided according to the cause/area of pain.
For non-specific low back pain, no consensus was reached for the use of superficial heat therapy alone in mild acute or chronic pain (66%), whereas a low-level consensus was obtained for the use of superficial heat therapy in association with analgesics in moderate-severe acute and chronic pain (88%). Moreover, no consensus (66%) was reached for the statement “superficial heat therapy is more effective if applied early in acute low back pain”.
For neck pain, the panelists agreed that superficial heat therapy can be used alone in mild acute/chronic pain (68%) and in association with analgesics in moderate-severe acute/chronic pain (83%).
For osteoarthritis, a strong consensus was obtained only on the statement “superficial heat therapy is more effective if associated with kinesiotherapy/exercise” (90%). The panelists agreed that superficial heat therapy can be used alone or as an adjuvant therapy in osteoarthritis (71%) and in association with analgesics in moderate-severe pain situations (78%). No consensus was reached on the role of heat therapy alone in mild acute/chronic pain (57%).
Maximizing Compliance to Heat Therapy
The panelists strongly agreed that superficial heat therapy can be used with caution as self-help therapy in mild pain (95%) and that heat wraps are normally well tolerated by patients (93%). They also agreed that heat therapy should not be self-prescribed in recurrent uninvestigated pain (89%). No consensus was obtained on the role of self-help use of superficial heat therapy in moderate-severe pain (51%).
Safety of Heat Therapy (Based on Heat Wraps)
Ninety-three percent of participants agreed that superficial heat therapy has a good safety profile. To guarantee efficacy and safety of superficial heat therapy, 95% agreed that the ideal temperature is approximately 40 °C. Regarding safety concerns, the panelists strongly agreed that “caution is required in subjects with active autoimmune diseases, cancer, active osteoarthritis, neurological diseases (multiple sclerosis, amyotrophic lateral sclerosis, spinal injuries), zoster and skin inflammatory conditions and circulation defects” (96%) and skin integrity is required (97%).
The panelists agreed that “superficial heat therapy has fewer side effects than pharmacological treatment” (89%) and that, compared to other heat therapies, heat wraps have a low risk profile (82%).
No consensus was reached on the safety of HT at night (rate of agreement: 59%).
Wrong Beliefs and Common Errors in the Prescription of Heat Therapy
The panelists disagreed on the role of heat therapy in preventing joint deterioration (74%), whereas no consensus was obtained on the role of heat therapy to prevent any pain associated with atmospheric pressure changes (rate of disagreement: 61%). The panelists agreed that heat therapy can be used also for dysmenorrhea (78%).
Considering the efficacy of superficial heat therapy, the panelists disagreed on the common idea that the higher the temperature, the better the effect (79%) and agreed that the time needed to increase body temperature depends on subcutaneous fat tissue thickness (80%).
Role of Heat Therapy as a Prevention of Muscular Damage in Athletes
The panelists strongly agreed that superficial heat therapy “can help to enhance range of movement and flexibility” (92%). They also agreed superficial heat therapy “can reduce pain before the application of any other therapy” (71%). A negative consensus (68%) was observed on the better role of heat versus cold after exercise.
No consensus was found for three statements: on the role of superficial heat therapy used before exercise to prevent muscular injuries (54% disagreed) and used after exercise to prevent pain (51% agreed); 64% disagreed about the comparison between heat therapy and stretching in preventing muscular damage.
Discussion
The purpose of the study was to perform a Delphi survey among a panel of European experts from different fields normally involved in the treatment of MP (rheumatologists, sport physicians, physiotherapists, family physicians, physiatrists) to gather an expert consensus on the role of HT in the treatment of MP as well as to generate clinical insights on the general use of superficial heat therapy.
After one round, a consensus was reached on 42/54 statements. A second round was not proposed by the KOLs because the absence of a consensus was either considered secondary to the heterogeneity of the panelists or reflected the absence of scientific evidence on specific topic. The Delphi methodology uses an anonymous panel of experts to answer to the survey proposed by the KOLs [12]. For this reason, no speculations on the panelist distribution could be performed. The fact that experts with different scientific profiles were asked to respond to specific topics (e.g., the topic “role of heat therapy as a prevention of muscular damage in athletes”) probably explains the heterogeneity of answers obtained in some statements. At the same time, in our opinion, the 78% of consensus reached in the first round despite the heterogeneity of the panelists gave a stronger value to the agreement/disagreement to the statements proposed.
Overall, the panelists strongly agreed with most statements defining the mechanism of action of heat on muscle. Referring to MP, heat applications determine the activation of thermoreceptors that inhibit the nociceptive signal. Several studies report that the analgesic effect of heat is mainly mediated by the activation of transient receptor potential (TRP) membrane channels, which modulate a descending anti-nociceptive pathway [4, 7, 14,15,16].
In addition, heat increases blood flow and metabolism in the area where it is applied and determines an improvement of muscle flexibility [17]. Heat can also contribute to the healing process in case of muscular injuries. Erasala et al. demonstrated that an increased tissue temperature of 38 °C, 40 °C and 42 °C (measured in the trapezius muscle of healthy volunteers) corresponded to increased local blood flow of respectively 27%, 77% and 144% [18]. As reported by Cameron et al., an increase of 1° determines an increase of 10–15% in local tissue metabolism; the increased metabolism contributes to the healing process by increasing catabolic and anabolic reactions and removing toxic products [19].
No consensus was obtained in the statement “supplemental heat can improve muscle strength during physical activity.” The difference between this statement and the others mentioned on this topic may be secondary to the more recent scientific demonstration of the role of heat in muscle strength. Freiwald et al. showed that adding superficial heat therapy to basic multimodal treatment in chronic low back pain determines a significant effect on muscular strength for both extension and rotation. Strength depends on muscular mass, activation of available muscles fibers and metabolic supply. When heat is applied, it causes increased blood flow, which increases the oxygen and nutrition supply to the muscle, enabling an increase of metabolic activity. This mechanism may lead to an increase in muscular activation and strength, with a consequent improvement in daily mobility [20,21,22].
Panelists also agreed with 89% of statements on the indication of superficial heat therapy in MP. Participants agreed that superficial heat therapy can be indicated in non-specific low back pain, chronic musculoskeletal pain, mechanical pain, DOMS, strain and sprain during the chronic phase of rehabilitation and that it is not indicated in acute inflammatory joint pain. Low-level consensus was obtained on the indication of superficial heat therapy in tendinosis and osteoarthritis, while no consensus was reached on the indication in acute MP. This suggests that the panelists were more likely to think that heat therapy is better indicated for active musculoskeletal complaints than for problems with the passive structures. It is possible that this opinion also addresses the fact that heat should not necessarily be applied for inflammatory complaints.
In non-specific low back pain, superficial heat therapy is indicated in acute, sub-acute and chronic phases. Non-specific low back pain represents a symptom more than a disease and is defined as pain in the back for which the pathoanatomical cause is undetermined [23]. In this scenario, non-pharmacological treatments, e.g., exercise, education, physiotherapy and heat therapy, represent the first-line therapies [7, 24, 25], and were demonstrated to be superior to NSAIDs, acetaminophen or inert therapies [26,27,28,29].
Regarding the statements on the indication of superficial heat therapy in acute vs. chronic MP, the observation of no consensus on its use in acute pain may be secondary to the generic definition of acute MP. In fact, in this case, heat should be used carefully and is not indicated in case of acute pain secondary to trauma, infections or malignancy. Moreover, in acute inflammatory pain, heat could be counterproductive because of the increased inflammation of tissues induced by heat [6]. In chronic MP, especially mechanical pain, the effectiveness of HT, mostly in combination with other non-pharmacological interventions, has been demonstrated in spinal, wrist and knee pain [30,31,32]. The indication of HT is also mentioned in Canadian and American guidelines for chronic mild to moderate MP [33, 34].
In DOMS, scientific evidence shows that heat can effectively reduce the pain degree with a comparable effectiveness to cold [9]; however, the correct time point for its application is still controversial [35, 36]. For Petrofsky et al., heat appears to be more effective when applied immediately after finishing an exercise or before exercise to prevent muscular damage [37], whereas Hotfiel et al. recommend the primary application of cold after muscle-damaging exercises to minimize the inflammatory response, followed by heat therapy [38].
All participants agreed that heat therapy has a short-term effect on pain and mobility [7, 39, 40], improving daily living activities. To obtain a long-term effect in chronic pain, a multimodal approach is preferable. A low-level consensus was reached on the role of heat therapy to prevent worsening of low back pain. The KOLs discussed this item and agreed that heat therapy is more effective as a rescue therapy in case of recurrence of pain than as a preventive treatment. This is mostly secondary to the fact that low back pain is most frequently non-specific, in which case, to prevent the recurrence of pain, exercises and education are the main interventions indicated [23, 41].
Considering the economic aspect, superficial heat therapy has a nonrefundable individual cost which may represent a limit to its use as prevention. This aspect may also explain the absence of consensus on the statement further investigated in the survey on “discontinuation or not of heat therapy after the resolution of pain,” where the low compliance to pain treatment normally observed in clinical practice may also represent a reason not to propose the continuation of the treatment after resolution of symptoms [42,43,44]. The debate on the overall economic cost for the health care system of nonadherence to pain treatments is of great relevance nowadays, as nonadherence increases the cost for the system [45]. therefore, an accurate economic reflection on superficial heat therapy should be performed in further studies.
Less agreement was found regarding the time and modalities of superficial heat therapy in specific conditions, reflecting a lack of scientific evidence on this topic. In fact, superficial heat therapy represents a common non-pharmacological strategy used in clinical practice but evidence on how to use it and for how long is limited or of low quality [39]. The panelists generally agreed that in moderate to severe pain a multimodal approach with a combination of different treatments is most indicated, while in case of mild pain they did not agree on the use of heat as monotherapy. The KOLs were surprised to see a weak positive consensus on the possible use of heat alone in osteoarthritis; the rheumatologist in the KOLs disagreed, considering that a combination of pharmacological and non-pharmacological treatments is most indicated in osteoarthritis (OA) no matter how severe is the pain. Bannuru et al., in the OARSI guideline [46], and Kolasinski et al., in the ACR recommendations [47], reported that exercise and education combined with NSAIDs are the most appropriate interventions in OA, while heat has only low-quality evidence of effectiveness. Moreover, for mild or recurrent pain, the self-prescribed use of superficial heat therapy is indicated with caution, whereas no consensus was reached on the use of superficial heat therapy as self-help in moderate to severe pain. The KOLs were surprised by the non-consensus on the discouraged use of self-prescribed heat therapy in moderate to severe pain as they had expected strong agreement on this. In their opinion, in this case a medical consultancy is indicated and should not be delayed; moreover, severe pain should not be managed by the patients themselves.
The panelists agreed on the safety profile of superficial heat therapy, which is also considered well tolerated by the patients. The ideal safe tissue temperature reached with superficial heat therapy is approximately 40 °C [27, 31, 36, 40, 48]. Skin integrity is required before any application of heat. Caution should be used in case of active autoimmune diseases, malignancies, active osteoarthritis or other inflammatory diseases, neurological diseases or conditions where peripheral sensitivity may be altered (multiple sclerosis, amyotrophic lateral sclerosis, spinal injuries, diabetes) and pregnancies. Although scientific evidence documented the safety profile of heat wrap use also at night [49], and its use at night is generally approved, the KOLs, considering the non-consensus obtained in the survey, suggest that the best advice to provide to the patient should be that the first application of a heat wrap should be performed during the daytime to monitor the effectiveness of the therapy and possible side effects.
The aim of the topic “wrong beliefs and common error in prescribing HT” was to gather an expert consensus to reinforce the correct indications for heat therapy and dispel common wrong ideas that are widely spread by non-scientific media or professionals. What emerged from the agreement/disagreement on the statements proposed is a strong agreement among experts about the wrong belief that “the higher the temperature, the better effect,” which may expose patients to severe side effects (burns/skin lesion), and that “heat therapy can heal structural diseases, for example osteoarthritis” (heat therapy is a symptomatic treatment). Moreover, they agreed on the statement “the time needed to achieve the goal temperature rise is proportional to the increased thickness of subcutaneous fat” (normally with 2 cm of subcutaneous fat the time needed to reach 40 °C is 30 min.
Finally, the last topic was the role of heat in the prevention of muscular damage in athletes. Unlike the previous topics, this represented a more specific and specialized item. The aim of KOLs was to evaluate the general knowledge among a heterogeneous group of experts on the role of heat in sports or active exercises. The lack of consensus in 50% of statements may reflect that this topic is unfamiliar to most clinicians. A first general consideration proposed by the KOLs is that, to guarantee the best possible treatment in any context, a multidisciplinary team should be involved in the management of patients with MP. Evaluating the single statements, the negative consensus on heat vs. cold used after exercise was considered interesting. The panelists strongly disagreed that heat was superior to cold, but scientific evidence on this topic is controversial. Petrofsky et al. demonstrated that the application of heat immediately after exercise was superior to cold in preventing muscular damage and strength loss, but the application after 24 h was inferior to cold in pain perception, and both were useless in preventing muscular damage [37]. Clijsen et al. reported that in pain perception cold is more effective than heat [50].
Another interesting observation is the statement “application of superficial heat therapy 4 h before exercise can help to prevent pain and muscular injuries,” for which consensus was not reached. It is commonly known that warming up before exercise helps the body's metabolism. The panelists may have thought that active warming up is more effective than superficial heat therapy. Mayer et al., in their randomized controlled trial on continuous low-level HT in the prevention and treatments of DOMS, showed that patients who received HT 4 h before any intense exercise had an increase of physical function (enhancing range of movement and flexibility) and pain relief [36].
Limits of this study were related mainly to the extent of the topic, which has different use profiles depending on the modality, indication and setting of use, and to the heterogenicity of the panelists. To minimize this second bias, panelists were identified according to their long-term experience in MP management.
Conclusion
In conclusion, the results of the Delphi survey suggest that European experts agreed on the effectiveness of superficial heat therapy in the treatment of MP as part of a multimodal approach to pain where different experts play a role in the patient’s treatment. Superficial heat therapy is indicated mostly in chronic musculoskeletal pain when secondary causes are excluded. Superficial heat therapy represents a safe, well-tolerated therapy that can be integrated in the treatment of MP by different specialists and in different settings (hospital, home, rehabilitation clinics). The use of this therapy should be regulated by scientific evidence and not left mainly to clinical evidence or to the patient’s discretion.
There are still some aspects where a consensus was not obtained, reflecting the persistence of open issues related to this topic. Moreover, there is still an important lack of good-quality evidence on the role of superficial heat therapy in musculoskeletal pain. Further studies are required to understand the effectiveness of this therapy.
Change history
31 October 2022
A Correction to this paper has been published: https://doi.org/10.1007/s40122-022-00449-y
References
Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain. 2019;160:19–27.
Puntillo F, Giglio M, Paladini A, et al. Pathophysiology of musculoskeletal pain: a narrative review. Ther Adv Musculoskelet Dis. 2021;13:1759720X21995067.
Blyth FM, Briggs AM, Schneider CH, Hoy DG, March LM. The global burden of musculoskeletal pain-where to from here? Am J Public Health. 2019;109:35–40.
Malanga GA, Yan N, Stark J. Mechanisms and efficacy of heat and cold therapies for musculoskeletal injury. Postgrad Med. 2015;127(1):57–65.
Papaioannou TG, Karamanou M, Protogerou AD, Tousoulis D. Heat therapy: an ancient concept re-examined in the era of advanced biomedical technologies. J Physiol. 2016;594(23):7141–2.
Nadler SF, Weingand K, Kruse RJ. The physiologic basis and clinical applications of cryotherapy and thermotherapy for the pain practitioner. Pain Physician. 2004;7(3):395–9.
Freiwald J, Magni A, Fanlo-Mazas P, et al. A role for superficial heat therapy in the management of non-specific, mild-to-moderate low back pain in current clinical practice: a narrative review. Life (Basel). 2021;11(8):780.
Kim K, Reid BA, Casey CA, et al. Effects of repeated local heat therapy on skeletal muscle structure and function in humans. J Appl Physiol. 2020;128(3):483–92.
Wang Y, Li S, Zhang Y, et al. Heat and cold therapy reduce pain in patients with delayed onset muscle soreness: a systematic review and meta-analysis of 32 randomized controlled trials. Phys Ther Sport. 2021;48:177–87.
Giannarou L, Zervas E. Using Delphi technique to build consensus in practice. Int J Bus Sci Appl Manag. 2014;9:65–82.
Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000;32:1008–15.
McPherson S, Reese C, Wendler MC. Methodology update: Delphi studies. Nurs Res. 2018;67(5):404–10.
Bruttomesso D, Laviola L, Avogaro A, et al. The use of real time continuous glucose monitoring or flash glucose monitoring in the management of diabetes: a consensus view of Italian diabetes experts using the Delphi method. Nutr Metab Cardiovasc Dis. 2019;29(5):421–31.
Green BG. Temperature perception and nociception. J Neurobiol. 2004;61(1):13–29.
Palazzo E, Rossi F, Maione S. Role of TRPV1 receptors in descending modulation of pain. Mol Cell Endocrinol. 2008;286(Suppl 1):S79-83.
Hung CY, Tan CH. TRP channels in nociception and pathological pain. Adv Exp Med Biol. 2018;1099:13–27.
Knight AC, Rutledge CR, Cox ME, Acosta M, Hall SJ. Effect of superficial heat, deep heat, and active exercise warm-up on the extensibility of the plantar flexors. Phys Ther. 2001;81(6):1206–14.
Erasala GN, Rubin JM, Tuthill TA, et al. The effect of topical heat treatment on trapezius muscle blood flow using power Doppler ultrasound. Phys Ther. 2001;81:A5.
Cameron MH. Thermal agents: physical principles, cold and superficial heat. In: Physical agents in rehabilitation: from research to practice. Philadelphia: Saunders; 1999. p. 149–75.
Michlovitz SL, Bellew JW, Nolan TP Jr. Modalities for therapeutic intervention. 5th ed. Philadelphia: F.A. Davis; 2011.
Gordon R, Bloxham S. A systematic review of the effects of exercise and physical activity on non-specific chronic low back pain. Healthcare (Basel). 2016;4(2):22.
Freiwald J, Hoppe MW, Beermann W, Krajewski J, Baumgart C. Effects of supplemental heat therapy in multimodal treated chronic low back pain patients on strength and flexibility. Clin Biomech (Bristol, Avon). 2018;57:107–13.
Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. 2017;389(10070):736–47.
Gianola S, Castellini G, Andreano A, et al. Effectiveness of treatments for acute and sub-acute mechanical non-specific low back pain: protocol for a systematic review and network meta-analysis. Syst Rev. 2019;8(1):196.
Gianola S, Bargeri S, Del Castillo G, et al. Effectiveness of treatments for acute and subacute mechanical non-specific low back pain: a systematic review with network meta-analysis. Br J Sports Med. 2021; bjsports-2020-103596.
Nadler SF, Steiner DJ, Erasala GN, et al. Continuous low-level heat wrap therapy provides more efficacy than Ibuprofen and acetaminophen for acute low back pain. Spine (Phila Pa 1976). 2002;27(10):1012–7.
Nadler SF, Steiner DJ, Erasala GN, Hengehold DA, Abeln SB, Weingand KW. Continuous low-level heatwrap therapy for treating acute nonspecific low back pain. Arch Phys Med Rehabil. 2003;84:329–34.
Lurie-Luke E, Neubauer G, Lindl C, Breitkreutz H, Fischer P, Hitzeroth S. An exploratory workplace study to investigate the perceived value of continuous low-level heatwrap therapy in manual workers. Occup Med. 2003;53:173–8.
Tao XG, Bernacki EJ. A randomized clinical trial of continuous low-level heat therapy for acute muscular low back pain in the workplace. J Occup Environ Med. 2005;47:1298–306.
Michlovitz S, Hun L, Erasala GN, Hengehold DA, Weingand KW. Continuous low-level heat wrap therapy is effective for treating wrist pain. Arch Phys Med Rehabil. 2004;85(9):1409–16.
Petrofsky JS, Laymon M, Alshammari F, Khowailed IA, Lee H. Use of low level of continuous heat and Ibuprofen as an adjunct to physical therapy improves pain relief, range of motion and the compliance for home exercise in patients with nonspecific neck pain: a randomized controlled trial. J Back Musculoskelet Rehabil. 2017;30(4):889–96.
Petrofsky JS, Laymon MS, Alshammari FS, Lee H. Use of low level of continuous heat as an adjunct to physical therapy improves knee pain recovery and the compliance for home exercise in patients with chronic knee pain: a randomized controlled trial. J Strength Cond Res. 2016;30(11):3107–15.
Côté P, Wong JJ, Sutton D, et al. Management of neck pain and associated disorders: a clinical practice guideline from the Ontario Protocol for Traffic Injury Management (OPTIMa) Collaboration. Eur Spine J. 2016;25(7):2000–22.
Qaseem A, Wilt TJ, McLean RM, et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the american college of physicians. Ann Intern Med. 2017;166(7):514–30.
Heiss R, Lutter C, Freiwald J, et al. Advances in delayed-onset muscle soreness (DOMS)—part ii: treatment and prevention. Sportverletz Sportschaden. 2019;33(1):21–9.
Mayer JM, Mooney V, Matheson LN, et al. Continuous low-level heat wrap therapy for the prevention and early phase treatment of delayed-onset muscle soreness of the low back: a randomized controlled trial. Arch Phys Med Rehabil. 2006;87(10):1310–7.
Petrofsky JS, Khowailed IA, Lee H, et al. Cold vs. heat after exercise-is there a clear winner for muscle soreness. J Strength Cond Res. 2015;29(11):3245–52.
Hotfiel T, Carl HD, Swoboda B, et al. Current conservative treatment and management strategies of skeletal muscle injuries. Z Orthop Unfall. 2016;154(3):245–53.
French SD, Cameron M, Walker BF, Reggars JW, Esterman AJ. A Cochrane review of superficial heat or cold for low back pain. Spine (Phila Pa 1976). 2006;31(9):998–1006.
Lewis SE, Holmes PS, Woby SR, Hindle J, Fowler NE. Short-term effect of superficial heat treatment on paraspinal muscle activity, stature recovery, and psychological factors in patients with chronic low back pain. Arch Phys Med Rehabil. 2012;93(2):367–72.
Krismer M, van Tulder M. Low back pain group of the bone and joint health strategies for Europe Project. Strategies for prevention and management of musculoskeletal conditions. Low back pain (non-specific). Best Pract Res Clin Rheumatol. 2007;21(1):77–91.
Jack K, McLean SM, Moffett JK, Gardiner E. Barriers to treatment adherence in physiotherapy outpatient clinics: a systematic review. Man Ther. 2010;15(3):220–8.
Bennell KL, Dobson F, Hinman RS. Exercise in osteoarthritis: moving from prescription to adherence. Best Pract Res Clin Rheumatol. 2014;28(1):93–117.
Diiulio J, Militello LG, Andraka-Christou BT, et al. Factors that influence changes to existing chronic pain management plans. J Am Board Fam Med. 2020;33(1):42–50.
Margolis JM, Princic N, Smith DM, et al. Economic impact of adherence to pain treatment guidelines in chronic pain patients. Pain Med. 2019;20(10):1907–18.
Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr Cartil. 2019;27(11):1578–89.
Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken). 2020;72(2):149–62.
Mayer JM, Ralph L, Look M, et al. Treating acute low back pain with continuous low-level heat wrap therapy and/or exercise: a randomized controlled trial. Spine J. 2005;5(4):395–403.
Nadler SF, Steiner DJ, Petty SR, Erasala GN, Hengehold DA, Weingand KW. Overnight use of continuous low-level heatwrap therapy for relief of low back pain. Arch Phys Med Rehabil. 2003;84(3):335–42.
Clijsen R, Stoop R, Hohenauer E, et al. Local heat applications as a treatment of physical and functional parameters in acute and chronic musculoskeletal disorders or pain. Arch Phys Med Rehabil. 2021; S0003-9993(21)00505-0.
Acknowledgements
The authors thank the participants in the Delphi process: Enrique Abarrio (Spain), Jaime Almazan Polo (Spain), Sara Alonso Castro (Spain), João Amaro (Portugal), Karner-Nechvile Angelika (Austria), Luis Arboleya (Spain), Olga Arroyo (Spain), Daniel Belavy (Germany), Pablo Belderrain (Spain), Elena Bueno-Gracia (Spain), Sara Cabanillas Barea (Spain), Margarida Cantista (Portugal), Alberti Capa (Spain), Andoni Carrasco-Uribarren (Spain), Antonio Carriero (Italy), Tiago Carvalho (Portugal), Juan Casar (Spain), Juan Ignacio Castillo Martin (Spain), Luis Ceballos Laita (Spain), Gabriella Cerna-Stadlmann (Austria), Elsa Maria Couto (Portugal), Isabel Crespo (Portugal), Richard Crevenna (Austria), Salvatore D'Angelo (Italy), Johannes Dersch (Germany), Lösel Dirk (Germany), Christina Duftner (Austria), Iñaki Erquicia Peralt (Spain), Marco Ezechieli (Germany), Valentin Ferrer Fernandez (Spain), Fátima Gandarez (Portugal), Jose Manuel Garzón Hernández (Spain), Melanie Glätzle (Austria), Vanessa Gonzalez Rueda (Spain), Johann Gruber (Austria), Álvaro Guerrero Cabezudo (Spain), Cesar Hidalgo Garcia (Spain), Sandra Jiménez-del-Barrio (Spain), Fernando Jirout (Spain), Marko Kayser (Austria), Peter Lang (Austria), Gerhard Leiner (Austria), Carlos López de Celis (Spain), Lourdes López de Munaín (Spain), Ana Machado Lima (Portugal), Miguel Malo Urriés (Spain), Ernesto Martìnez Estrada (Spain), Tecla Mastronuzzi (Italy), Diogo Manuel Melo Soares (Portugal), Dobner Michael (Austria), Santiago Miranda (Spain), Valerie Nell-Duxneuner (Austria), Filomena Cabral Pacheco de Melo (Portugal), Juan Carlos Palacio (Spain), Sara Paradinha (Portugal), Domenico Pasculli (Italiy), Jorge Pérez Rey (Spain), Fabio Massimo Perrotta (Italy), João Pinto Coelho (Portugal), Cesar Ricardo Román Banks (Spain), Josu Sagarduy De La Mar (Spain), Rubén Saiz Reguera (Spain), Susana Santos (Portugal), Dorothea Schmelzer (Austria), Angelo Semeraro (Italy), Francisco Tavares (Portugal), Tischer Thomas (Germany), Rita Tomás (Portugal), Mónica Toth Fernández (Spain), María José Villanueva Díaz (Spain), Lutz Vogt (Germany), Barbara Wagner (Austria), Melanie Wohlgenannt Wohlgenannt (Austria), Isabel Zapico (Spain), Carlos Zubizarreta Lain (Spain). The listed authors have authorized the submission of their manuscript via third party and approved any statements or declarations.
Funding
The editorial and rapid service fee has been realized thanks to unconditional support of Angelini Pharma.
Medical Writing and/or Editorial Assistance
The authors acknowledge the writing support of Irene Avagnina.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Authors' Contributions
All authors conceived, read and approved the manuscript.
Disclosures
Ennio Lubrano, Pablo Fanlo Mazas, Jurgen Freiwald, Karsten Krüger, Ignazio Grattagliano, Erich Mur, Ruben Queiro Silva, Guillermo Rodríguez Maruri, Luís Sequeira de Medeiros declare that they have no competing interests.
Compliance with Ethics Guidelines
The study was carried out in accordance with the European Data Protection Rules with informed consent from all participants. According to article 1, paragraph 1, of the legislative decree no. 211 of 2003 (legislation implementing the European Directive 2001/20/EC on the application of good clinical practice in the execution of clinical trials of medicinal products for clinical use), no formal ethics approval was needed since no research on human tissue or other biological material was performed.
The participants were informed about the use and publication of their anonymized data for this study and that their names will be included in the paper. Participation in the study was voluntary. Returning the completed questionnaire was interpreted as informed consent to participate in the study. No incentives were offered.
Data Availability
All data generated or analyzed during this study are included in this published article/as supplementary information files.
Author information
Authors and Affiliations
Corresponding author
Additional information
The original online version of this article was revised: to correct the alignment of few entries in Table 2 and to correct a sentence.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Lubrano, E., Mazas, P.F., Freiwald, J. et al. An International Multidisciplinary Delphi-Based Consensus on Heat Therapy in Musculoskeletal Pain. Pain Ther 12, 93–110 (2023). https://doi.org/10.1007/s40122-022-00419-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40122-022-00419-4