
Abstract
Purpose
This retrospective cohort study derived a “quick” version of the Pitt bacteremia score (qPitt) using binary variables in patients with Gram-negative bloodstream infections (BSI). The qPitt discrimination was then compared to quick sepsis-related organ failure assessment (qSOFA) and systemic inflammatory response syndrome (SIRS).
Methods
Hospitalized adults with Gram-negative BSI at Palmetto Health hospitals in Columbia, SC, USA from 2010 to 2013 were identified. Multivariate Cox proportional hazards regression was used to determine variables associated with 14-day mortality.
Results
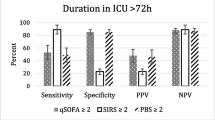
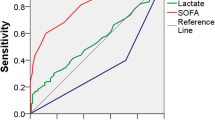
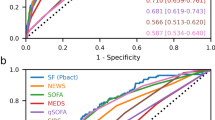
Among 832 patients with Gram-negative BSI, median age was 65 years and 449 (54%) were women. After adjustments for age and Charleston comorbidity score, all five components of qPitt were independently associated with mortality: temperature < 36 °C [hazard ratio (HR) 3.02, 95% confidence interval (CI) 1.95–4.62], systolic blood pressure < 90 mmHg or vasopressor use (HR 2.40, 95% CI 1.37–4.13), respiratory rate ≥ 25/min or mechanical ventilation (HR 3.01, 95% CI 1.81–5.14), cardiac arrest (HR 5.35, 95% CI 2.81–9.43), and altered mental status (HR 3.99, 95% CI 2.44–6.80). The qPitt had higher discrimination to predict mortality [area under receiver operating characteristic curve (AUROC) 0.85] than both qSOFA (AUROC 0.77, p < 0.001) and SIRS (AUROC 0.63, p < 0.001). There was a significant difference in mortality between appropriate and inappropriate empirical antimicrobial therapy in patients with qPitt ≥ 2 (24% vs. 49%, p < 0.001), but not in those with qPitt < 2 (3% vs. 5%, p = 0.36).
Conclusions
The qPitt had good discrimination in predicting mortality following Gram-negative BSI and identifying opportunities for improved survival with appropriate empirical antimicrobial therapy.

Similar content being viewed by others
References
Goto M, Al-Hasan MN. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe. Clin Microbiol Infect. 2013;19:501–9.
Uslan DZ, Crane SJ, Steckelberg JM, et al. Age-and sex-associated trends in bloodstream infection. Arch Intern Med. 2007;167:834–9.
McGregor JC, Rich SE, Harris AD, et al. A systematic review of the methods used to assess the association between appropriate antibiotic therapy and mortality in bacteremic patients. Clin Infect Dis. 2007;45:329–37.
Al-Hasan MN, Lahr BD, Eckel-Passow JE, Baddour LM. Predictive scoring model of mortality in gram-negative bloodstream infection. Clin Microbiol Infect. 2013;19:948–54.
Al-Hasan MN, Juhn YJ, Bang DW, et al. External validation of Gram-negative bloodstream infection mortality risk score in a population-based cohort. Clin Microbiol Infect. 2014;20:886–91.
Retamar P, Portillo MM, López-Prieto MD, et al. Impact of inadequate empirical therapy on the mortality of patients with bloodstream infections: a propensity score-based analysis. Antimicrob Agents Chemother. 2012;56:472–8.
Cain SE, Kohn J, Bookstaver PB, et al. Stratification of the impact of inappropriate empirical antimicrobial therapy for gram-negative bloodstream infections by predicted prognosis. Antimicrob Agents Chemother. 2015;59:245–50.
Korvick JA, Bryan CS, Farber B, et al. Prospective observational study of Klebsiella bacteremia in 230 patients: outcome for antibiotic combinations versus monotherapy. Antimicrob Agents Chemother. 1992;36:2639–44.
Paterson DL, Ko WC, Von Gottberg A, et al. International prospective study of Klebsiella pneumoniae bacteremia: implications of extended-spectrum beta-lactamase production in nosocomial Infections. Ann Intern Med. 2004;140:26–32.
Rhee JY, Kwon KT, Ki HK, et al. Scoring systems for prediction of mortality in patients with intensive care unit-acquired sepsis: a comparison of the Pitt bacteremia score and the Acute Physiology and Chronic Health Evaluation II scoring systems. Shock. 2009;31:146–50.
Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis: for the third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315:762–74.
Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315:801–10.
Sundén-Cullberg J, Rylance R, Svefors J, Norrby-Teglund A, Björk J, Inghammar M. Fever in the emergency department predicts survival of patients with severe sepsis and septic shock admitted to the ICU. Crit Care Med. 2017;45:591–9.
Laupland KB, Church DL. Population-based epidemiology and microbiology of community-onset bloodstream infections. Clin Microbiol Rev. 2014;27:647–64.
Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36:309–32.
Friedman ND, Kaye KS, Stout JE, et al. Health care-associated bloodstream infections in adults: a reason to change the accepted definition of community-acquired infections. Ann Intern Med. 2002;137:791–7.
Bone RC, Balk RA, Cerra FB, et al. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med 1992;20:864–874.
Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143:29–36.
Raith EP, Udy AA, Bailey M, et al. Prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for in-hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA. 2017;317:290–300.
Freund Y, Lemachatti N, Krastinova E, et al. Prognostic accuracy of sepsis-3 criteria for in-hospital mortality among patients with suspected infection presenting to the emergency department. JAMA. 2017;317:301–8.
Moskowitz A, Patel PV, Grossestreuer AV, et al. Quick sequential organ failure assessment and systemic inflammatory response syndrome criteria as predictors of critical care intervention among patients with suspected infection. Crit Care Med. 2017;45:1813–9.
Finkelsztein EJ, Jones DS, Ma KC, et al. Comparison of qSOFA and SIRS for predicting adverse outcomes of patients with suspicion of sepsis outside the intensive care unit. Crit Care. 2017;21:73.
Fernando SM, Tran A, Taljaard M, et al. Prognostic accuracy of the quick sequential organ failure assessment for mortality in patients with suspected infection: a systematic review and meta-analysis. Ann Intern Med. 2018;168:266–75.
Maitra S, Som A, Bhattacharjee S. Accuracy of quick sequential organ failure assessment (qSOFA) score and systemic inflammatory response syndrome (SIRS) criteria for predicting mortality in hospitalized patients with suspected infection: a meta-analysis of observational studies. Clin Microbiol Infect. 2018;24:1123–9.
Gransden WR, Leibovici L, Eykyn SJ, et al. Risk factors and a clinical index for diagnosis of Pseudomonas aeruginosa bacteremia. Clin Microbiol Infect. 1995;1:119–23.
Hammer KL, Justo JA, Bookstaver PB, Kohn J, Albrecht H, Al-Hasan MN. Differential effect of prior β-lactams and fluoroquinolones on risk of bloodstream infections secondary to Pseudomonas aeruginosa. Diagn Microbiol Infect Dis. 2017;87:87–91.
Augustine MR, Testerman TL, Justo JA, et al. Clinical risk score for prediction of extended-spectrum beta-lactamase producing Enterobacteriaceae in bloodstream isolates. Infect Control Hosp Epidemiol. 2017;38:266–72.
Battle SE, Kohn J, Bookstaver B, Albrecht H, Al-Hasan MN. Association between inappropriate empirical antimicrobial therapy and hospital length of stay in gram-negative bloodstream infections: stratification by prognosis. J Antimicrob Chemother. 2017;72:299–304.
Acknowledgements
The authors thank Prisma Health Antimicrobial Stewardship and Support Team in South Carolina, USA for their help in facilitating the conduct of this study. SEB, MRA and MNA have full access to all of the data in the study and take responsibility for the integrity of the data and accuracy of the analysis. The preliminary results of this study were presented in part at IDWeek annual meeting on October 7, 2017 in San Diego, CA, USA.
Funding
The study received internal funding from the Grant-in-Aid, Palmetto Health Richland Research and Education Foundation, Columbia, SC, USA. There were no other sources of funding for this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
MNA: Continuing medical education steering committee, Rockpointe Corporation. PBB: Advisory board member, CutisPharma; Speaker’s Bureau, Melinta Therapeutics; speaker and continuing medical education steering committee, Rockpointe Corporation. SEB, MRA, CMW, WO, JK, LMB: no conflicts.
Electronic supplementary material
Below is the link to the electronic supplementary material.
15010_2019_1277_MOESM1_ESM.tif
Supplementary material 1 Supplemental Figure 1: Calibration plot of qPitt model. The observed frequency of 14-day mortality plotted by deciles of predicted probability from the qPitt model (black dots). Perfect calibration is represented by the grey Y=X line (TIF 37 KB)
15010_2019_1277_MOESM2_ESM.tif
Supplementary material 2 Supplemental Figure 2: Receiver operating characteristic plot of qPitt model. Black line indicates receiver operating characteristic curve. Light color tangent line highlights the point in the curve that represents the best performance of the model. Area under receiver operating characteristic curve= 0.85 (TIF 48 KB)
15010_2019_1277_MOESM3_ESM.tif
Supplementary material 3 Supplemental Figure 3: Kaplan–Meier survival curves of patients with bloodstream infection and qPitt < 2 by appropriateness of empirical antimicrobial therapy (TIF 44 KB)
Rights and permissions
About this article

Cite this article
Battle, S.E., Augustine, M.R., Watson, C.M. et al. Derivation of a quick Pitt bacteremia score to predict mortality in patients with Gram-negative bloodstream infection. Infection 47, 571–578 (2019). https://doi.org/10.1007/s15010-019-01277-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s15010-019-01277-7