
Abstract
Objective
We postulated that a contiguous rectal dose-volume threshold curve obtained via a best mathematical fit of the toughest literature recommended dose-volume thresholds could be deemed as “safe” related to the risk of rectal toxicity. The practicality of restricting rectal doses to such ideal volume thresholds in clinical practice was tested by comparing data collected from a pool of prostate patients treated with external beam radiation therapy (EBRT) in our institution.
Methods
Available rectal dose-volume constraint recommendation in prostate EBRT was collected. At each dose level, the toughest recommended volume limit was identified and an ideal dose-volume threshold curve was generated using a best mathematical fit. Rectal dose-volume data on 105 prostate patients treated to 75.6 Gy dose with intensity modulated radiation therapy (IMRT) in our institution were retrospectively reviewed.
Results
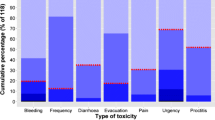
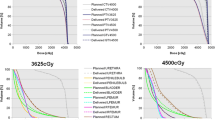
The “ideal” rectal dose-volume threshold curve is defined by V 75 ≤ 7%, V 70 ≤ 11%, V 65 ≤ 15%, V 60 ≤ 20%, V 50 ≤ 30%, V 40 ≤ 43%, and V 30 ≤ 60%. At doses larger or equal to 65 Gy, our patient averaged dose-volume histograms (DVHs) for all groups converged with the ideal curve. At intermediate and low doses (less than 60 Gy), higher volumes of rectum were irradiated than described by the hypothetical curve, with pelvic group receiving more rectal dose than prostate only group respectively. Rectal mean dose correlated strongly with V 40 values (R 2 = 0.84).
Conclusion
Our “ideal” rectal dose-volume curve generated from literature dose-volume thresholds in the most stringent manner is realistic and achievable at high doses (≥60 Gy) and not realistic at intermediate and low doses (≤50 Gy). Standardizing rectal definition and dose-volume metrics will make published analyses and dose-volume constraint recommendations easier to follow.




Similar content being viewed by others

References
Viani GA, Stefano EJ, Alfonso SL (2009) Higher-than-conventional radiation doses in localized prostate cancer treatment: a meta-analysis of randomized, controlled trials. Int J Radiat Oncol Biol Phys 74:1405–1418
Brenner DJ (2004) Fractionation and late rectal toxicity. Int J Radiat Oncol Biol Phys 74:1405–1418
Wachter S, Gerstner N, Goldner G et al (2001) Rectal sequelae after conformal radiotherapy of prostate cancer: dose-volume histograms as predictive factors. Radiother Oncol 59:65–70
Fiorino C, Cozzarini C, Vavassori V et al (2002) Relationships between DVHs and late rectal bleeding after radiotherapy for prostate cancer: analysis of a large group of patients pooled from three institutions. Radiother Oncol 64:1–12
Kuban D, Pollack A, Huang E et al (2003) Hazards of dose escalation in prostate cancer radiotherapy. Int J Radiat Oncol Biol Phys 57:1260–1268
Beckendorf V, Guerif S, Le Prise E et al (2004) The GETUG 70 Gy vs. 80 Gy randomized trial for localized prostate cancer: feasibility and acute toxicity. Int J Radiat Oncol Biol Phys 60:1056–1065
Koper PCM, Heemsbergen WD, Hoogeman MS et al (2004) Impact of volume and location of irradiated rectum wall on rectal bold loss after radiotherapy of prostate cancer. Int J Radiat Oncol Biol Phys 58:1072–1082
Peeters ST, Hoogeman MS, Heemsbergen WD et al (2006) Rectal bleeding, fecal incontinence, and high stool frequency after conformal radiotherapy for prostate cancer: normal tissue complication probability modeling. Int J Radiat Oncol Biol Phys 66:11–19
Fiorino C, Sanguineti G, Cozzarini C et al (2003) Rectal dose-volume constraints in high-dose radiotherapy of localized prostate cancer. Int J Radiat Oncol Biol Phys 57:953–962
Zapatero A, Garcia-Vicente F, Modolell I et al (2004) Impact of mean rectal dose on late rectal bleeding after conformal radiotherapy for prostate cancer: dose-volume effect. Int J Radiat Oncol Biol Phys 59:1343–1351
Vargas C, Martinez A, Kestin L et al (2005) Dose-volume analysis of predictors for chronic rectal toxicity after treatment of prostate cancer with adaptive image-guided radiotherapy. Int J Radiation Oncol Biol Phys 62:1297–1308
Greco C, Mazzetta C, Cattani F et al (2003) Finding dose-volume constraints to reduce late rectal toxicity following 3D-conformal radiotherapy (3D-CRT) of prostate cancer. Radiother Oncol 69:215–222
Zelefsky MJ, Levin EJ, Hunt M et al (2008) Incidence of late rectal and urinary toxicities after three-dimensional conformal radiotherapy and intensity modulated radiotherapy for localized prostate cancer. Int J Radiat Oncol Biol Phys 70:1124–1129
Chan LW, Xia P, Gottschalk AR et al (2008) Proposed rectal dose constraints for patients undergoing definitive whole pelvic radiotherapy for clinically localized prostate cancer. Int J Radiat Oncol Biol Phys 72:69–77
Pollack AM, Zagars GK, Starkschall G et al (2002) Prostate cancer radiation dose response: results of thee M.D. Anderson Phase III randomized trial. Int J Radiat Oncol Biol Phys 53(5):1097–1105
Storey MR, Pollack A et al (2000) Complications from radiotherapy dose escalation in prostate cancer: preliminary results of a randomized trial. Int J Radiat Oncol Biol Phys 48:635–642
Swanson GP, Stathakis S (2011) Rectal dose constraints for intensity modulated radiation therapy of the prostate. Am J Clin Oncol 34(2):188–195
Gulliford SL, Foo K, Morgan RC et al (2010) Dose-volume constraints to reduce rectal side effects from prostate radiotherapy: evidence from MRC RT01 Trial ISRCTN 47772397. Int J Radiat Oncol Biol Phys 76(3):747–754
Michalski JM, Gay H, Jackson A et al (2010) Radiation dose-volume effects in radiation-induced rectal injury. Int J Radiat Oncol Biol Phys S123–S129
Fiorino C, Fellin G, Rancati T et al (2008) Clinical and dosimetric predictors of late rectal syndrome after 3D-CRT for localized prostate cancer: preliminary results of a multicenter prospective study. Int J Radiat Oncol Biol Phys. 7094):1130–1137
Pederson AW, Fricano J, Pelizzari CA et al (2012) Late toxicity after intensity-modulated radiation therapy for localized prostate cancer: an exploration of dose-volume histogram parameters to limit genitourinary and gastrointestinal toxicity. Int J Radiat Oncolo Biol Phys 82(1):235–241
Kopp RW, Duff M, Catalfamo F et al (2011) VMAT VS. 7-field IMRT: assessing the dosimetric parameters of prostate cancer treatment with a 292-patient sample. Med Dosim 36(4):365–372
Peterson JL, Buskirk SJ, Heckman MG et al (2014) Image-guided intensity-modulated radiation therapy for prostate cancer: dose constraints for the anterior rectal wall to minimize rectal toxicity. Med Dosim 39(1):12–17
Mirjolet C, Walker PM, Gauthier M et al (2016) Absolute volume of the rectum and AUC from rectal DVH between 25 Gy and 50 Gy predict acute gastrointestinal toxicity with IG-IMRT in prostate cancer. Radiat Oncol 11:145–150
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
The work was supported by the Department of Radiation Oncology, Montefiore Medical Center and the Albert Einstein College of Medicine in Bronx, New York, USA.
Conflict of interest
Author Ravindra Yaparpalvi declares that he has no conflict of interest.
Author Madhur K Garg declares that he has no conflict of interest.
Author Nitin Ohri declares that he has no conflict of interest.
Author William R Bodner declares that he has no conflict of interest.
Author Wolfgang A Tome declares that he has no conflict of interest.
Author Chandan Guha declares that he has no conflict of interest.
Author Shalom Kalnicki declares that he has no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Yaparpalvi, R., Garg, M.K., Ohri, N. et al. Defining an “ideal” continuous dose-volume constraint curve using literature recommended individual dose-volume thresholds for reducing rectal toxicity from external beam prostate radiation therapy. J Radiat Oncol 6, 405–411 (2017). https://doi.org/10.1007/s13566-017-0323-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13566-017-0323-6