
Abstract
Objective
Endoluminal brachytherapy (EBT) has been shown to be an effective neoadjuvant monotherapy for rectal adenocarcinoma. Radiographic predictors of response are used to guide treatment in rectal cancer; however, no predictors of response to EBT have been identified.
Methods
This is a single-institutional prospective study from 2010 to 2013. Analysis included 17 patients undergoing EBT and 13 patients undergoing conventional external beam chemoradiation (CRT). Clinical response to therapy was assessed with serial MRI and PET/CT variables. Pathological response to therapy was assessed using tumor regression grade (TRG) and compared with clinical response.
Results
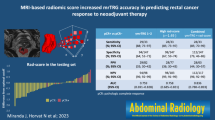
EBT and CRT patients did not differ with respect to age, sex, race, carcinoembryonic antigen, or clinical stage of disease. There was a similar rate of pathologic complete response for both groups, with a trend towards more TRG 0 with EBT compared with CRT (35.3% vs. 7.7%, p = 0.08). Four days of EBT resulted in a significantly greater reduction in tumor volume on MRI than did CRT (92.7% vs. 63.1%, p = 0.004). Using receiver operating characteristic analysis, change in peak standardized uptake value was the best predictor for complete pathologic response in EBT patients (sensitivity 67%, specificity 82%). False-positive findings for nodal disease on MRI were seen in 59% of EBT patients and 23% of CRT patients.
Conclusions
This study demonstrates that EBT is an effective alternative with similar response rates to CRT. However, the inability of MRI and PET/CT to discern reactive from malignant tumor and nodes may pose limitations in their use for guiding further therapy. Larger randomized studies are needed.


Similar content being viewed by others


References
Camma C et al (2000) Preoperative radiotherapy for resectable rectal cancer: a meta-analysis. JAMA 284(8):1008–1015
Colorectal Cancer Collaborative, G (2001) Adjuvant radiotherapy for rectal cancer: a systematic overview of 8,507 patients from 22 randomised trials. Lancet 358(9290):1291–1304
Rodel C et al (2003) Phase I/II trial of capecitabine, oxaliplatin, and radiation for rectal cancer. J Clin Oncol 21(16):3098–3104
Meyer J et al (2011) Update on treatment advances in combined-modality therapy for anal and rectal carcinomas. Curr Oncol Rep 13(3):177–185
Sauer R et al (2004) Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 351(17):1731–1740
Vuong T et al (2005) The safety and usefulness of high-dose-rate endoluminal brachytherapy as a boost in the treatment of patients with esophageal cancer with external beam radiation with or without chemotherapy. Int J Radiat Oncol Biol Phys 63(3):758–764
Martinez-Monge R et al (2009) Phase I-II trial of perioperative high-dose-rate brachytherapy in oral cavity and oropharyngeal cancer. Brachytherapy 8(1):26–33
Harms W et al (2001) Contemporary role of modern brachytherapy techniques in the management of malignant thoracic tumors. Semin Surg Oncol 20(1):57–65
Smith JA et al (2012) Clinicopathologic comparison of high-dose-rate endorectal brachytherapy versus conventional chemoradiotherapy in the neoadjuvant setting for resectable stages II and III low rectal cancer. Int J Surg Oncol 2012:406568
Vuong T et al (2002) Conformal preoperative endorectal brachytherapy treatment for locally advanced rectal cancer: early results of a phase I/II study. Dis Colon rectum 45(11):1486–1493 discussion 1493-5
Vuong T, Devic S, Podgorsak E (2007) High dose rate endorectal brachytherapy as a neoadjuvant treatment for patients with resectable rectal cancer. Clin Oncol (R Coll Radiol) 19(9):701–705
Vuong T, Devic S (2015) High-dose-rate pre-operative endorectal brachytherapy for patients with rectal cancer. J Contemp Brachytherapy 7(2):183–188
Eisenhauer EA et al (2009) New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 45(2):228–247
Wahl RL et al (2009) From RECIST to PERCIST: evolving considerations for PET response criteria in solid tumors. J Nucl Med 50(Suppl 1):122S–150S
Ryan R et al (2005) Pathological response following long-course neoadjuvant chemoradiotherapy for locally advanced rectal cancer. Histopathology 47(2):141–146
Tang, L.H., et al. 2013 Protocol for the examination of specimens from patients with primary carcinoma of the colon and rectum. College of American Pathologists. ColonRectum 3.3.0.0.
Appelt AL et al (2015) High-dose chemoradiotherapy and watchful waiting for distal rectal cancer: a prospective observational study. Lancet Oncol 16(8):919–927
Hesselager C et al (2013) Short-term outcome after neoadjuvant high-dose-rate endorectal brachytherapy or short-course external beam radiotherapy in resectable rectal cancer. Color Dis 15(6):662–666
Wiltshire KL et al (2006) Preoperative radiation with concurrent chemotherapy for resectable rectal cancer: effect of dose escalation on pathologic complete response, local recurrence-free survival, disease-free survival, and overall survival. Int J Radiat Oncol Biol Phys 64(3):709–716
Rodel C et al (2005) Prognostic significance of tumor regression after preoperative chemoradiotherapy for rectal cancer. J Clin Oncol 23(34):8688–8696
Gerard JP et al (2006) Preoperative radiotherapy with or without concurrent fluorouracil and leucovorin in T3-4 rectal cancers: results of FFCD 9203. J Clin Oncol 24(28):4620–4625
Bosset JF et al (2006) Chemotherapy with preoperative radiotherapy in rectal cancer. N Engl J Med 355(11):1114–1123
Branagan G et al (2004) Can magnetic resonance imaging predict circumferential margins and TNM stage in rectal cancer? Dis Colon rectum 47(8):1317–1322
Kuo LJ et al (2005) Interpretation of magnetic resonance imaging for locally advanced rectal carcinoma after preoperative chemoradiation therapy. Dis Colon rectum 48(1):23–28
Chen CC et al (2005) How accurate is magnetic resonance imaging in restaging rectal cancer in patients receiving preoperative combined chemoradiotherapy? Dis Colon rectum 48(4):722–728
Heijnen, L.A. 2016 et al., Nodal staging in rectal cancer: why is restaging after chemoradiation more accurate than primary nodal staging? Int J Colorectal Dis.
Koh DM et al (2008) Evaluating mesorectal lymph nodes in rectal cancer before and after neoadjuvant chemoradiation using thin-section T2-weighted magnetic resonance imaging. Int J Radiat Oncol Biol Phys 71(2):456–461
Prall F et al (2006) Tumour regression and mesorectal lymph node changes after intensified neoadjuvant chemoradiation for carcinoma of the rectum. APMIS 114(3):201–210
Capirci C et al (2007) Sequential FDG-PET/CT reliably predicts response of locally advanced rectal cancer to neo-adjuvant chemo-radiation therapy. Eur J Nucl Med Mol Imaging 34(10):1583–1593
de Geus-Oei LF et al (2009) Monitoring and predicting response to therapy with 18F-FDG PET in colorectal cancer: a systematic review. J Nucl Med 50(Suppl 1):43S–54S
Denecke T et al (2005) Comparison of CT, MRI and FDG-PET in response prediction of patients with locally advanced rectal cancer after multimodal preoperative therapy: is there a benefit in using functional imaging? Eur Radiol 15(8):1658–1666
De Cecco, C.N., et al. 2016 , Performance of diffusion-weighted imaging, perfusion imaging, and texture analysis in predicting tumoral response to neoadjuvant chemoradiotherapy in rectal cancer patients studied with 3T MR: initial experience. Abdom Radiol (NY).
Hotker, A.M., et al. 2016 Multiparametric MRI in the assessment of response of rectal cancer to neoadjuvant chemoradiotherapy: a comparison of morphological, volumetric and functional MRI parameters. Eur Radiol.
De Nardi P, Carvello M (2013) How reliable is current imaging in restaging rectal cancer after neoadjuvant therapy? World J Gastroenterol 19(36):5964–5972
Melton GB et al (2007) Efficacy of preoperative combined 18-fluorodeoxyglucose positron emission tomography and computed tomography for assessing primary rectal cancer response to neoadjuvant therapy. J Gastrointest Surg 11(8):961–969 discussion 969
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This work was supported by the Elekta/Nucletron company who provided study support; however, no salary support was provided for the investigators.
Conflict of interest
Rebecca Craig-Schapiro, Ihab R. Kamel, Michael Sacerdote, Joseph Canner, Meredith Pittman, Caitlin W. Hicks, Amy Hacker-Prietz, Robert F. Hobbs, Elwood P. Armour, Jonathan E. Efron, Elizabeth C. Wick, and Nilofer S. Azad, declare that they have no conflict of interest. Joseph M. Herman and Susan L. Gearhart were investigators on a grant with Elekta/Nucletron who supplied financial support for the study; however, no salary support was given for this study.
Ethical approval
This study was approved by the institutional review board of Johns Hopkins, and written informed consent was obtained from all study participants. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in this study.
Rights and permissions
About this article

Cite this article
Craig-Schapiro, R., Kamel, I.R., Sacerdote, M. et al. Radiographic predictors of response to endoluminal brachytherapy for the treatment of rectal cancer. J Radiat Oncol 6, 287–294 (2017). https://doi.org/10.1007/s13566-017-0302-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13566-017-0302-y