
Abstract
Objectives
The primary goal of this study is to determine prognostic factors associated with freedom from biochemical failure (FFBF) and survival for men with localized prostate cancer treated with intensity-modulated radiation therapy (IMRT) stratified according to the NCCN 2015 guidelines in a community hospital setting. A secondary objective is to evaluate long-term toxicity at last follow-up compared to pretreatment status (bowel, bladder, and sexual functioning) using a modified Radiation Therapy Oncology Group (RTOG) toxicity grading system. A final objective is to compare our results of IMRT in a community-based radiation practice to published results from academic institutions.
Methods
Two hundred and twenty-eight consecutive men treated with IMRT for organ-confined prostate cancer at Delaware County Memorial Hospital (DCMH) from 2003 when the IMRT program began to 2012 were reviewed on this IRB-approved retrospective study. Biochemical failure was assessed using the Phoenix Nadir +2 definition. CT and MRI treatment planning was used and treatment volumes included prostate +/− seminal vesicles and true pelvic lymph nodes depending on risk assessment based on pretreatment prognostic factors. Median dose to the prostate was 75.6 Gy. Median follow-up for the entire group was 72 months.
Results
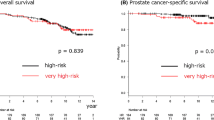
Ten-year actuarial FFBF for the entire group was 83.2 %. Eight-year actuarial FFBF stratified by 2015 NCCN risk stratification was 95.2 % very low risk, 96.3 % low risk, 81.5 % intermediate risk, 75.4 % high risk, and 38.7 % for the very high risk group (p = 0.02). Patients with PSA <30.65 had improved 8-year FFBF of 85.9 % compared with 46.1 % for PSA >30.65 (p = 0.0001). Multivariable analysis revealed only the five NCCN risk groups were independent prognosticators for FFBF. Ten-year actuarial survival for the entire group was 61.1 %. Only 8 deaths were secondary to prostate cancer out of 59 total deaths (13.6 %). Ten-year actuarial overall survival stratified by 2015 NCCN risk stratification was 68.8 % very low risk, 81.5 % low risk, 67.2 % intermediate risk, 46.3 % high risk, and 54.9 % for the very high risk group (p = 0.02). Ten-year overall survival rates stratified by age less than or greater than 71.5 were 75.9 % for age ≤71.5 and 55.2 % for age >71.5 (p = 0.01). Multivariable analysis revealed only age was an independent significant factor for survival with p = 0.0008. Grade 3 GI toxicity at last follow-up was 0.5 % with no grade 4 toxicities. Grade 3 GU toxicity at last follow-up was 1 % with no grade 4 toxicities. FFBF and toxicity rates are comparable to those reported by academic institutions and literature review of published data with comparison to our community hospital data will be presented.
Conclusions
The outcome of IMRT for men with prostate cancer treated in a community hospital is comparable to that of published literature from academic institutions. NCCN 2015 risk stratification is prognostic for FFBF. Age at diagnosis was the only significant independent predictor of survival, suggesting that cancer-specific mortality is minimized after IMRT in localized prostate cancer.







Similar content being viewed by others

References
Sheets NC et al (2012) Intensity-modulated radiation therapy, proton therapy, or conformal radiation therapy and morbidity and disease control in localized prostate cancer. JAMA 307:1611–1620
Jacobs BL et al (2013) Use of advanced treatment technologies among men at low risk of dying from prostate cancer. JAMA 309:2587–2595
Hayes JH et al (2010) Active surveillance compared with initial treatment for men with low-risk prostate cancer: a decision analysis. JAMA 304:2373–2380
Hayes JH et al (2013) Observation versus initial treatment for men with localized, low-risk prostate cancer: a cost-effectiveness analysis. Ann Intern Med 158:853–860
Wilt TJ et al (2012) Radical prostatectomy versus observation for localized prostate cancer. N Engl J Med 367:203–213
Nguyen PL et al (2011) Cost implications of the rapid adoption of newer technologies for treating prostate cancer. J Clin Oncol 29:1517–1524
Thames H et al (2003) Comparison of alternative biochemical failure definitions based on clinical outcome in 4839 prostate cancer patients treated by external beam radiotherapy between 1986 and 1995. Int J Radiat Oncol Biol Phys 57:929–943
Jacobs BL et al (2014) Comparative effectiveness of external-beam radiation approaches for prostate cancer. Eur Urol 65:162–168
Chism DB et al (2003) Late morbidity profiles in prostate cancer patients treated to 79-84 Gy by a simple four-field coplanar beam arrangement. Int J Radiat Oncol Biol Phys 55:71–77
Lawton CA et al (1991) Long-term treatment sequelae following external beam irradiation for adenocarcinoma of the prostate: analysis of RTOG studies 7506 and 7706. Int J Radiat Oncol Biol Phys 21:935–939
Smit WG et al (1990) Late radiation damage in prostate cancer patients treated by high dose external radiotherapy in relation to rectal dose. Int J Radiat Oncol Biol Phys 18:23–29
Ling CC et al (1996) Conformal radiation treatment of prostate cancer using inversely-planned intensity-modulated photon beams produced with dynamic multileaf collimation. Int J Radiat Oncol Biol Phys 35:721–730
Zelefsky MJ et al (2000) Clinical experience with intensity modulated radiation therapy (IMRT) in prostate cancer. Radiother Oncol 55:241–249
Zelefsky MJ et al (2002) High-dose intensity modulated radiation therapy for prostate cancer: early toxicity and biochemical outcome in 772 patients. Int J Radiat Oncol Biol Phys 53:1111–1116
Spratt DE et al (2013) Long-term survival and toxicity in patients treated with high-dose intensity modulated radiation therapy for localized prostate cancer. Int J Radiat Oncol Biol Phys 85:686–692
Dearnaley DP et al (2007) Escalated-dose versus standard-dose conformal radiotherapy in prostate cancer: first results from the MRC RT01 randomised controlled trial. Lancet Oncol 8:475–487
Pollack A et al (2000) Preliminary results of a randomized radiotherapy dose-escalation study comparing 70 Gy with 78 Gy for prostate cancer. J Clin Oncol 18:3904–3911
Zietman AL et al (2005) Comparison of conventional-dose vs high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate. JAMA J Am Med Assoc 294:1233
Peeters STH et al (2006) Dose-response in radiotherapy for localized prostate cancer: results of the Dutch multicenter randomized phase III trial comparing 68 Gy of radiotherapy with 78 Gy. J Clin Oncol 24:1990–1996
Cahlon O et al (2008) Ultra-high dose (86.4 Gy) IMRT for localized prostate cancer: toxicity and biochemical outcomes. Int J Radiat Oncol Biol Phys 71:330–337
Eade TN et al (2007) What dose of external-beam radiation is high enough for prostate cancer? Int J Radiat Oncol Biol Phys 68:682–689
Litwin MS et al (2007) Quality of life after surgery, external beam irradiation, or brachytherapy for early-stage prostate cancer. Cancer 109:2239–2247
Penson DF, Litwin MS (2003) Quality of life after treatment for prostate cancer. Curr Urol Rep 4:185–195
Zelefsky MJ et al (2008) Long-term results of conformal radiotherapy for prostate cancer: impact of dose escalation on biochemical tumor control and distant metastases-free survival outcomes. Int J Radiat Oncol Biol Phys 71:1028–1033
Kupelian PA, Willoughby TR, Reddy CA, Klein EA, Mahadevan A (2007) Hypofractionated intensity-modulated radiotherapy (70 Gy at 2.5 Gy per fraction) for localized prostate cancer: Cleveland Clinic Experience. Int J Radiat Oncol Biol Phys 68:1424–1430
Teh BS et al (2001) Intensity-modulated radiation therapy (IMRT) for prostate cancer with the use of a rectal balloon for prostate immobilization: acute toxicity and dose-volume analysis. Int J Radiat Oncol Biol Phys 49:705–712
De Meerleer GO et al (2007) Intensity-modulated radiation therapy for prostate cancer: late morbidity and results on biochemical control. Radiother Oncol 82:160–166
De Meerleer GO et al (2000) Radiotherapy of prostate cancer with or without intensity modulated beams: a planning comparison. Int J Radiat Oncol Biol Phys 47:639–648
Pollack A et al (2002) Prostate cancer radiation dose response: results of the M. D. Anderson phase III randomized trial. Int J Radiat Oncol Biol Phys 53:1097–1105
Reese AC, Pierorazio PM, Han M, Partin AW (2012) Contemporary evaluation of the national comprehensive cancer network prostate cancer risk classification system. Urology 80:1075–1079
Jani AB, Su A, Correa D, Gratzle J (2007) Comparison of late gastrointestinal and genitourinary toxicity of prostate cancer patients undergoing intensity-modulated versus conventional radiotherapy using localized fields. Prostate Cancer Prostatic Dis 10:82–86. doi:10.1038/sj.pcan.4500910
Vora SA, Wong WW, Schild SE, Ezzell GA, Halyard MY (2007) Analysis of biochemical control and prognostic factors in patients treated with either low-dose three-dimensional conformal radiation therapy or high-dose intensity-modulated radiotherapy for localized prostate cancer. Int J Radiat Oncol Biol Phys 68:1053–1058. doi:10.1016/j.ijrobp.2007.01.043
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This retrospective study was reviewed and approved by the Crozer Keystone Health Care System’s Institutional Review Board.
Conflicts of interest
All authors declare that they have no competing interests.
Consent to participate
For this type of study, formal consent is not required.
Rights and permissions
About this article

Cite this article
Ricco, A., Lanciano, R. & Hanlon, A. Predictors of long-term survival for localized prostate cancer treated with high-dose IMRT stratified by NCCN 2015 guidelines in a community hospital setting. J Radiat Oncol 5, 95–101 (2016). https://doi.org/10.1007/s13566-015-0224-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13566-015-0224-5