
Abstract
Purpose
Surgical therapy of infective endocarditis (IE) is challenging and can be associated with high mortality. In this study, we present the early outcomes of patients who underwent cardiac surgery for IE.
Methods
From 2017 until 2019, 66 patients underwent surgical treatment for IE. Staphylococcus aureus infection was identified in 14 patients (21%). In the same period, about 813 valve replacement procedures were performed with 8% incidence of IE. Mean age was 66 ± 12 years and 32% were females. Mean ejection fraction was 55 ± 9%. Seven patients (11%) had stroke due to septic embolism preoperatively. In 20 patients (30%), prosthetic valve endocarditis was an indication for reoperation. Thirty-day postoperative mortality and impact of preoperative stroke were analyzed.
Results
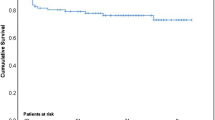
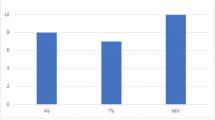
Thirty-day mortality was 17% (n = 11). Mean EuroSCORE I was 28 ± 22%. Mean cross clamp time was 63 ± 37 min. Fourty patients (61%) underwent one-valve procedure, 25 patients (38%) had double-valve, and one (1%) triple-valve operation. All seven patients with preoperative neurologic dysfunction had unremarkable postoperative course without death or neurologic deterioration. Five of them had no worsening in neurological status, while 2 patients had slight improvement in speech. The comparison between the two groups (patients without preoperative neurological vs. patients with preoperative neurological dysfunction) revealed no significance in the postoperative mortality rate (18% vs. 0% with p = 0.26). Postoperative echocardiography revealed competent valve function in all cases.
Conclusion
Surgical treatment for IE still remains a challenge with high morbidity and mortality. Patients with preoperative neurologic dysfunction due to septic embolism have good early postoperative results without increased mortality.
Similar content being viewed by others

References
Cahill TJ, Baddour LM, Habib G, et al. Challenges in infective endocarditis. J Am Coll Cardiol. 2017;69:325–44.
Navia JL, Elgharably H, Hakim AH, et al. Long-term outcomes of surgery for invasive valvular endocarditis involving the aortomitral fibrosa. Ann Thorac Surg. 2019;108:1314–23.
Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin Infect Dis. 2000;30:633–8.
Kang DH. Timing of surgery in infective endocarditis. Heart. 2015;101:1786–91.
Bretschneider HJ. Myocardial protection. Thorac Cardiovasc Surg. 1980;28:295–302.
Bakhtiary F, El-Sayed Ahmad A, Borger M. Modification of reconstruction of intervalvular fibrous body for extensive infective endocarditis. Ann Thorac Surg. 2020;109:E211–E214.
Seeburger J, Borger MA, Falk V, et al. Minimal invasive mitral valve repair for mitral regurgitation-results of 1339 consecutive patients. Eur J Cardiothorac Surg. 2008;34:760–5.
Zamorano J, de Isla LP, Malangatana G, et al. Infective endocarditis: mid-term prognosis in patients with good in-hospital outcome. J Heart Valve Dis. 2005;14:303–9.
Kang DH, Kim YJ, Kim SH, et al. Early surgery versus conventional treatment for infective endocarditis. N Engl J Med. 2012;366:2466–73.
Gatti G, Benussi B, Gripshi F, et al. A risk factor analysis for in-hospital mortality after surgery for infective endocarditis and a proposal of a new predictive scoring system. Infection. 2017;45:413–23.
Chu VH, Park LP, Athan E, et al. Association between surgical indications, operative risk, and clinical outcome in infective endocarditis: a prospective study from the International Collaboration on Endocarditis. Circulation. 2015;131:131–40.
Jakuska P, Ereminiene E, Muliuolyte E, et al. Predictors for early mortality after surgical treatment of infective endocarditis: a single-center experience. Perfusion. 2019. https://doi.org/10.1177/0267659119872345
Suzuki K, Yoshioka D, Toda K, et al. Results of surgical management of infective endocarditis associated with Staphylococcus aureus. Eur J Cardiothorac Surg. 2019;56:30–37.
Musci M, Hubler M, Amiri A, et al. Surgical treatment for active infective prosthetic valve endocarditis: 22-year single-center experience. Eur J Cardiothorac Surg. 2010;38:528–38.
Oliveira JLR, Santos MAD, Arnoni RT, et al. Mortality predictors in the surgical treatment of active infective endocarditis. Braz J Cardiovasc Surg. 2018;33:32–9.
Sá MP, Rueda FG, Ferraz PE, Chalegre ST, Vasconcelos FP, Lima RC. Is there any difference between blood and crystalloid cardioplegia for myocardial protection during cardiac surgery? A meta-analysis of 5576 patients from 36 randomized trials. Perfusion. 2012;27:535–46.
Funding
None
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Statement of human rights/ethical approval
This retrospective study complies with the principles of the Declaration of Helsinki and was approved by the institutional ethics committee. All procedures being performed were part of the routine care.
Informed consent
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Monsefi, N., Öztürk, M., Shavahatli, T. et al. Outcome of surgery for acute infective endocarditis: does preoperative stroke have an impact on mortality?. Indian J Thorac Cardiovasc Surg 36, 373–381 (2020). https://doi.org/10.1007/s12055-020-00943-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12055-020-00943-y