
Abstract
Background
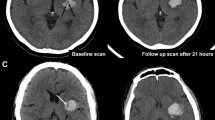
Early hematoma expansion in intracerebral hemorrhage (ICH) patients is associated with poor outcome. We aimed to investigate whether the minimal computed tomography (CT) attenuation value predicted hematoma expansion and poor outcome.
Methods
This study involved spontaneous ICH patients of two cohorts who underwent baseline CT scan within 6 h after ICH onset and follow-up CT scan within 24 h after initial CT scan. We determined the critical value of the minimal CT attenuation value via retrospective analysis of the data from a derivation cohort. Then, a prospective study on the validation cohort of three clinical centers was performed for determining the association between the minimal CT attenuation value and hematoma expansion as well as poor outcome (modified Rankin Scale scores > 3) at 90 days by using univariate and multivariate logistic regression analyses.
Results
One hundred and forty eight ICH patients were included in the derivation cohort. Minimal CT attenuation value ≤ 31 Hounsfield units (HU) was demonstrated as the critical value to predict hematoma expansion by using receiver operating characteristic analysis. A total of 311 ICH patients were enrolled in the validation cohort, 86 (27.7%) and 133 (42.8%) of which were found hematoma expansion and poor outcome. Minimal CT attenuation value ≤ 31 HU was positive in 73 patients (23.5%). The multivariate logistic regression analysis demonstrated minimal CT attenuation value and minimal CT attenuation value ≤ 31 HU independently predicted hematoma expansion (p < 0.001) and poor outcome (p < 0.001). The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of minimal CT attenuation value ≤ 31 HU for hematoma expansion and poor outcome prediction were 64.0, 92.0, 75.3, 87.0, 84.2 and 45.1%, 92.7%, 82.2%, 69.3%, 72.3%, respectively.
Conclusions
The minimal CT attenuation value independently predicts early hematoma expansion and poor outcome in patients with ICH.




Similar content being viewed by others


References
van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9:167–76.
Demchuk AM, Dowlatshahi D, Rodriguez-Luna D, et al. Prediction of haematoma growth and outcome in patients with intracerebral haemorrhage using the CT-angiography spot sign (PREDICT): a prospective observational study. Lancet Neurol. 2012;11:307–14.
Hemphill JC 3rd, Greenberg SM, Anderson CS, et al. Guidelines for the management of spontaneous intracerebral hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2015;46:2032–60.
Dowlatshahi D, Demchuk AM, Flaherty ML, et al. Defining hematoma expansion in intracerebral hemorrhage: relationship with patient outcomes. Neurology. 2011;76:1238–44.
Delgado Almandoz JE, Yoo AJ, Stone MJ, et al. Systematic characterization of the computed tomography angiography spot sign in primary intracerebral hemorrhage identifies patients at highest risk for hematoma expansion: the spot sign score. Stroke. 2009;40:2994–3000.
Barras CD, Tress BM, Christensen S, et al. Density and shape as CT predictors of intracerebral hemorrhage growth. Stroke. 2009;40:1325–31.
Sporns PB, Schwake M, Kemmling A, et al. Comparison of spot sign, blend sign and black hole sign for outcome prediction in patients with intracerebral hemorrhage. J Stroke. 2017;19:333–9.
Li Q, Zhang G, Huang YJ, et al. Blend sign on computed tomography: novel and reliable predictor for early hematoma growth in patients with intracerebral hemorrhage. Stroke. 2015;46:2119–23.
Li Q, Zhang G, Xiong X, et al. Black hole sign: novel imaging marker that predicts hematoma growth in patients with intracerebral hemorrhage. Stroke. 2016;47:1777–81.
Selariu E, Zia E, Brizzi M, Abul-Kasim K. Swirl sign in intracerebral haemorrhage: definition, prevalence, reliability and prognostic value. BMC Neurol. 2012;12:109.
Xu X, Chen X, Zhang J, et al. Comparison of the Tada formula with software slicer: precise and low-cost method for volume assessment of intracerebral hematoma. Stroke. 2014;45:3433–5.
Qureshi AI, Palesch YY, Barsan WG, et al. Intensive blood-pressure lowering in patients with acute cerebral hemorrhage. N Engl J Med. 2016;375:1033–43.
Hanley DF, Lane K, McBee N, et al. Thrombolytic removal of intraventricular haemorrhage in treatment of severe stroke: results of the randomised, multicentre, multiregion, placebo-controlled CLEAR III trial. Lancet. 2017;389:603–11.
Boulouis G, Morotti A, Brouwers HB, et al. Association between hypodensities detected by computed tomography and hematoma expansion in patients with intracerebral hemorrhage. JAMA Neurol. 2016;73:961–8.
Kazui S, Naritomi H, Yamamoto H, Sawada T, Yamaguchi T. Enlargement of spontaneous intracerebral hemorrhage. Incidence and time course. Stroke. 1996;27:1783–7.
Goldstein JN, Fazen LE, Snider R, et al. Contrast extravasationon CT angiography predicts hematoma expansion inintracerebral hemorrhage. Neurology. 2007;68:889–94.
Sporns PB, Schwake M, Kemmling A, Minnerup J, Schwindt W, Niederstadt T, et al. Comparison of spot sign, blend sign and black hole sign for outcome prediction in patients with intracerebral hemorrhage. J Stroke. 2017;19:333–9.
Boulouis G, Morotti A, Brouwers HB, et al. Noncontrast computed tomography hypodensities predict poor outcome in intracerebral hemorrhage patients. Stroke. 2016;47:2511–6.
Dong J, Yang X, Xiang J, et al. Hypodensities detected at 1.5–3 h after intracerebral hemorrhage better predicts secondary neurological deterioration. J Neurol Sci. 2019;396:219–24.
Morotti A, Boulouis G, Romero JM, et al. Blood pressure reduction and noncontrast CT markers of intracerebral hemorrhage expansion. Neurology. 2017;89:548–54.
New PF, Aronow S. Attenuation measurements of whole blood and blood fractions in computed tomography. Radiology. 1976;121:635–40.
Schlunk F, Greenberg SM. The pathophysiology of intracerebral hemorrhage formation and expansion. Transl Stroke Res. 2015;6:257–63.
Wolverson MK, Crepps LF, Sundaram M, Heiberg E, Vas WG, Shields JB. Hyperdensity of recent hemorrhage at body computed tomography: incidence and morphologic variation. Radiology. 1983;148:779–84.
Boulouis G, Morotti A, Charidimou A, Dowlatshahi D, Goldstein JN. Noncontrast computed tomography markers of intracerebral hemorrhage expansion. Stroke. 2017;48:1120–5.
Brouwers HB, Chang Y, Falcone GJ, et al. Predicting hematoma expansion after primary intracerebral hemorrhage. JAMA Neurol. 2014;71:158–64.
Morotti A, Dowlatshahi D, Boulouis G, et al. Predicting intracerebral hemorrhage expansion with noncontrast computed tomography: the BAT score. Stroke. 2018;49:1163–9.
Chu H, Huang C, Dong J, et al. Lactate dehydrogenase predicts early hematoma expansion and poor outcomes in intracerebral hemorrhage patients. Transl Stroke Res. 2019;1:1. https://doi.org/10.1007/s12975-019-0686-7.
Morotti A, Brouwers HB, Romero JM, et al. Intensive blood pressure reduction and spot sign in intracerebral hemorrhage: a secondary analysis of a randomized clinical trial. JAMA Neurol. 2017;74:950–60.
Meretoja A, Churilov L, Campbell BC, et al. The spot sign and tranexamic acid on preventing ICH growth–AUStralasia Trial (STOP-AUST): protocol of a phase II randomized, placebo-controlled, double-blind, multicenter trial. Int J Stroke. 2014;9:519–24.
Author information
Authors and Affiliations
Contributions
HC and CH contributed to study design, data collection, and analysis and drafting of the manuscript. JD, XY, JX, and YM involved in data collection and analysis. QD and YT took part in conception and design, acquisition of clinical data, revision and approval of the manuscript. All authors gave the final approval of the version to be published. Authorship requirements have been met, and the final manuscript was approved by all authors. This manuscript has not been published elsewhere and is not under consideration by another journal.
Corresponding authors
Ethics declarations
Source of Support
This research was supported by grants from the National Natural Science Foundation of China (Nos. 81500998; 81701244; 81801290), Science and Technology Commission of Shanghai Municipality (No. 16140903200), and Shanghai Sixth People’s Hospital Medical Group (2017LY01).
Conflicts of interest
The authors declare that they have no conflict of interest.
Ethical Approval/Informed Consent
All patients or their next-of-kin gave their informed consent prior to inclusion in this study. This study was approved by and studied in accordance with the ethical standards of the Ethics Committee of Fudan University.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chu, H., Huang, C., Dong, J. et al. Minimal Computed Tomography Attenuation Value Within the Hematoma is Associated with Hematoma Expansion and Poor Outcome in Intracerebral Hemorrhage Patients. Neurocrit Care 31, 455–465 (2019). https://doi.org/10.1007/s12028-019-00754-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-019-00754-z