
Opinion statement
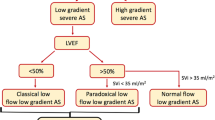
Severe low-gradient (LG) aortic stenosis (AS) [aortic valve area (AVA) ≤ 1.0 cm2, mean pressure gradient (MG) < 40 mmHg] represents a frequently encountered and challenging clinical dilemma. A systematic approach, which often requires several imaging modalities, should be undertaken to confirm the hemodynamic findings and rule out measurement error. Low-flow conditions often account for the discrepancy and can be present whether the left ventricular ejection fraction (LVEF) is depressed or normal. In patients with classical low-flow (LF), LG AS in which LVEF is reduced (<40–50 %), dobutamine stress echocardiography (DSE) should be used to distinguish patients with true severe AS and pseudo-severe AS, as well as to evaluate for the presence of left ventricular contractile or flow reserve. Surgical or transcatheter aortic valve replacement (AVR) should likely be reserved for those patients with true severe AS. Patient outcome with medical or surgical management generally relates to patient functional capacity, stenosis severity, and left ventricular functional reserve. Patients with severe LG AS with preserved LVEF can have a stroke volume that is either normal (>35 mL/m2) or low (<35 mL/m2). New data suggest that DSE can identify pseudo-severe AS in up to 30 % of patients with severe LF-LG AS with preserved LVEF. AVR should likely be restricted to those patients with true severe AS, although there is currently little data to support this strategy. Symptomatic patients with severe LG AS with preserved LVEF, whether they have normal or low flow, should be offered AVR. Transcatheter AVR provides an alternative therapeutic option in the high-risk patient.

Similar content being viewed by others


References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Nishimura RA, Otto CM, Bonow RO, et al. AHA/ACC Guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. ACC/AHA Task Force Members. Circulation. 2014;129:e521–643. An important document updating the previous 2006 AHA/ACC guidelines on the management of patients with valvular heart disease.
Vahanian A, Alfieri O, Andreotti F, et al. Guidelines on the management of valvular heart disease (version 2012): the Joint Task Force on Management of Valvular Heart Disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). ESC Committee for Practice Guidelines (CGP); Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (EACTS). Eur Heart J. 2012;2451–96.
Baumgartner H, Hung J, Bermejo J, et al. Echocardiographic assessment of vavle stenosis: EAS/ASE recommendations for clinical practice. American Society of Echocardiography; European Association of Echocardiography. J Am Soc Echocardiogr. 2009;22:1–23.
Otto CM, Burwash IG, Legget ME, et al. Prospective study of asymptomatic valvular aortic stenosis. Clinical, echocardiographic and exercise predictors or outcome. Circulation. 1997;95:2262–70.
Monin JL, Lancellotti P, Monchi M, et al. Risk score for predicting outcome in patients with asympatomatic aortic stenosis. Circulation. 2009;120:69–75.
Malouf J, Le Tourneau T, Pellikka P, et al. Aortic valve stenosis in community medical practice: determinants of outcome and implications for aortic valve replacement. J Thorac Cardiovasc Surg. 2012;144:1421–7.
Stewart RA, Kerr AJ, Whalley GA, et al. New Zealand Heart Valve Study Investigators. Left ventricular systolic and diastolic function assessed by tissue Doppler imaging and outcome in asymptomatic aortic stenosis. Eur Heart J. 2010;31:2216–22.
Minners J, Allgeier M, Gohlke-Baerwolf C, et al. Inconsistencies of echocardiographic criteria for the grading of aortic valve stenosis. Eur Heart J. 2008;29:1043–8.
Michelena HI, Margaryan E, Miller FA, et al. Inconsistent echocardiographic grading of aortic stenosis: is the left ventricular outflow tract important? Heart. 2013;99:921–31.
Hachicha Z, Dumesnil JG, Pibarot P. Usefulness of the valvuloarterial impedance to predict adverse outcome in asymptomatic aortic stenosis. J Am Coll Cardiol. 2009;54:1003–11.
Jander N, Minners J, Holme I, et al. Outcome of patients with low-gradient “severe” aortic stenosis and preserved ejection fraction. Circulation. 2011;123:887–95.
Mohty D, Magne J, Deltreuil M, et al. Outcome and impact of surgery in paradoxical low-flow, low-gradient severe aortic stenosis and preserved left ventricular ejection fraction: a cardiac catheterization study. Circulation. 2013;128(11 Suppl 1):S235–42.
Connolly HM, Oh JK, Orszulak TA, et al. Aortic valve replacement for aortic stenosis with severe left ventricular dysfunction. Prognostic indicators. Circulation. 1997;95:2395–400.
Connolly HM, Oh JK, Schaff HV, et al. Severe aortic stenosis with low transvalvular gradient and severe left ventricular dysfunction: result of aortic valve replacement in 52 patients. Circulation. 2000;101:1940–6.
Kulik A, Burwash IG, Kapila V, et al. Long-term outcomes after valve replacement for low-gradient aortic stenosis: impact of prosthesis–patient mismatch. Circulation. 2006;114:553–8.
Piazza N, de Jaegere P, Schultz C, et al. Anatomy of the aortic valvar complex and its implications for transcatheter implantation of the aortic valve. Circ Cardiovasc Interv. 2008;1:74–81.
Ng AC, Delgado V, van der Kley F, et al. Comparison of aortic root dimensions and geometries before and after transcatheter aortic valve implantation by 2- and 3 dimensional transesophageal echocardiography and multislice computed tomography. Circ Cardiovasc Imaging. 2010;3:94–102.
Nakai H, Takeuchi M, Yoshitani H, et al. Pitfalls of anatomical aortic valve area measurements using two-dimensional transoesophageal echocardiography and the potential of three-dimensional transoesophageal echocardiography. Eur J Echocardiogr. 2010;11:369–76.
Saikrishnan N, Kumar G, Sawaya FJ, et al. Accurate assessment of aortic stenosis: a review of diagnostic modalities and hemodynamics. Circulation. 2014;129:53. A comprehensive review of the hemodynamic concepts associated with AS and the various modalities and indices that can be used to evaluate hemodynamic severity.
Clavel MA, Messika-Zeitoun D, Pibarot P, et al. The complex nature of discordant severe calcified aortic valve disease grading: new insights from combination Doppler echocardiographic and computed tomographic study. J Am Coll Cardiol. 2013;62:2329–38. At least half of patients with severe LG AS with preserved LVEF have an AVC score similar to that observed in patients with severe HG AS. An AVC score ≥2065 AU in men and ≥1274 AU in women is strongly suggestive of severe AS.
Burwash IG. Low flow, low gradient aortic stenosis: From evaluation to treatment. Curr Opin Cardiol. 2007;22:84–91.
Burwash IG, Dickinson A, Teskey RJ, et al. Aortic valve area discrepancy by Gorlin equation and Doppler echocardiography continuity equation: relationship to flow in patients with valvular aortic stenosis. Can J Cardiol. 2000;16:985–92.
Saito T, Muro T, Takeda H, et al. Prognostic value of aortic valve area index in asymptomatic patients with severe aortic stenosis. Am J Cardiol. 2012;110:93–7.
Jander N, Gohlke-Baerwold C, Kaufmann BA, et al. Indexing aortic valve area by body surface area increases the prevalence of severe aortic stenosis. Heart. 2014;100:28–33. Indexing AVA by body surface area increases the prevalence of severe AS, but did not improve the prediction of aortic valve events in the SEAS trial.
Minners J, Gohlke-Baerwold C, Kaufmann BA, et al. Adjusting parameters of aortic valve stenosis by body size. Heart. 2014;100:1024–30.
Neilan TF, Pradhan AD, Weyman AE. Derivation of a size-independent variable for scaling of cardiac dimensions in a normal adult population. J Am Soc Echocardiogr. 2008;21:779–85.
Gorlin R, Gorlin SG. Hydraulic formula for calculation of the area of the stenotic mitral valve, other cardiac valves, and central circulatory shunts. Am Heart J. 1951;41:1–29.
Carabello BA. Aortic stenosis. N Engl J Med. 2002;346:677–82.
Pibarot P, Dumesnil JG. Low-flow, low-gradient aortic stenosis with normal and depressed left ventricular ejection fraction. J Am Coll Cardiol. 2012;60:1845–53.
Hachicha Z, Dumesnil J, Bogaty P, Pibarot P. Paradoxical low-flow, low-gradient severe aortic stenosis despite preserved ejection fraction is associated with higher afterload and reduced survival. Circulation. 2007;115:2856–64.
Clavel MA, Fuchs C, Burwash IG, et al. Predictors of outcomes in low-flow, low gradient aortic stenosis: results of the multicenter TOPAS Study. Circulation. 2008;118(14suppl):S234–42.
Minners J, Allgeier M, Gohlke-Baerwolf, et al. Heart. 2010;96:1463–8.
Adda J, Mielot C, Giorgi R, et al. Low-flow, low-gradient severe aortic stenosis despite normal ejection fraction is associated with severe left ventricular dysfunction as assessed by speckle-tracking echocardiography: a multicenter study. Circ Cardiovasc Imaging. 2012;5:27–35.
Mehrotra P, Jansen K, Flynn AW, et al. Differential left ventricular remodeling and longitudinal function distinguishes low flow from normal-flow preserved ejection fraction low-gradient severe aortic stenosis. Eur Heart J. 2013;34:1906–14.
Herrmann S, Störk S, Niemann M, et al. Low-gradient aortic valve stenosis myocardial fibrosis and its influence on function and outcome. J Am Coll Cardiol. 2011;58:402–12.
Eleid MF, Nishimura RA, Borlaug BA, Sorajja P. Invasive measures of afterload in low gradient severe aortic stenosis with preserved ejection fraction. Circ Heart Fail. 2013;6(4):703–10.
Sato K, Seo Y, Ishizu T et al. Prognostic value of global longitudinal strain in paradoxical low-flow, low-gradient severe aortic stenosis with preserved ejection fraction. Circ J 2014;78:2750–9. In patients with severe LF-LG AS with preserved LVEF, a GLS<-17% was associated with a significantly better 2 year event free survival compared to patients with GLS >-17%, and comparable to patients with severe NF-LG AS.
Lancellotti P, Magne J, Donal E, et al. Clinical outcome in asymptomatic severe aortic stenosis. Insights from the new proposed aortic stenosis grading classification. J Am Coll Cardiol. 2012;59:235–43.
Burwash IG, Hay KM, Chan KL. Hemodynamic stability of valve area, valve resistance and stroke work loss in aortic stenosis: a comparative analysis. J Am Soc Echocardiogr. 2002;15:814–22.
Fougeres E, Tribouilloy C, Monchi M, et al. Outcomes of pseudosevere aortic stenosis under conservative treatment. Eur Heart J. 2012;33:2426–33.
Nishimura RA, Grantham JA, Connolly HM, et al. Low-output, low-gradient aortic stenosis in patients with depressed left ventricular systolic function: the clinical utility of the dobutamine challenge in the catheterization laboratory. Circulation. 2002;106:809–13.
Monin JL, Quere JP, Monchi M, et al. Low-gradient aortic stenosis: operative risk stratification and predictors for long-term outcome: a multicenter study using dobutamine stress hemodynamics. Circulation. 2003;108:319–24.
DeFilippi CR, Willett DL, Brickner ME, et al. Usefulness of dobutamine echocardiography in distinguishing severe from non-severe valvular aortic stenosis in patients with depressed left ventricular function and low transvalvular gradients. Am J Cardiol. 1995;75:191–4.
Schwammenthal E, Vered Z, Moshkowitz Y, et al. Dobutamine echocardiography in patients with aortic stenosis and left ventricular dysfunction: predicting outcome as a function of management strategy. Chest. 2001;119:1766–7.
Blais C, Burwash IG, Mundigler G, et al. Projected valve area at normal flow rate improves the assessment of stenosis severity in patients with low-flow, low-gradient aortic stenosis. The multicentre TOPAS (True or Pseudo-severe aortic stenosis) study. Circulation. 2006;113:711–21.
Clavel MA, Burwash IG, Mundigler G, et al. Validation of conventional and simplified methods to calculate projected valve area at normal flow rate in patients with low flow, low gradient aortic stenosis: the multicentre TOPAS (True or Pseudo Severe Aortic Stenosis) study. J Am Soc Echocardiogr. 2010;23:380–6.
Cueff C, Serfaty JM, Cimadevilla C, et al. Measurement of aortic valve calcification using multislice computed tomography: correlation with hemodynamic severity of aortic stenosis and clinical implication for patients with low ejection fraction. Heart. 2011;97:721–6.
Burwash IG, Lortie M, Pibarot P, et al. Myocardial blood flow in patients with low flow, low gradient aortic stenosis: differences between true and pseudo-severe aortic stenosis. Heart. 2008;94:1627–33.
Tribouilloy C, Levy F, Rusinaru D, et al. Outcome after aortic valve replacement for low-flow/low-gradient aortic stenosis without contractile reserve on dobutamine stress echocardiography. J Am Coll Cardiol. 2009;53:1865–73.
Pai RG, Varadarajan P, Razzouk A. Survival benefit of aortic valve replacement in patients with severe aortic stenosis with low ejection fraction and low gradient with normal ejection fraction. Ann Thorac Surg. 2008;86:1781–9.
Levy F, Laurent M, Monin JL, et al. Aortic valve replacement for low-flow/low-gradient aortic stenosis operative risk stratification and long-term outcome: a European Multicenter Study. J Am Coll Cardiol. 2008;51:1466–72.
Bartko PE, Heinze G, Clavel MA, et al. Two-dimensional strain for the assessment of left ventricular function in low-flow, low-gradient aortic stenosis, relationship to hemodynamics and outcome: a substudy of the multicentre TOPAS study. Circ Cardiovasc Imaging. 2013;6:268–76. DSE peak global longitudinal strain rate was a strong predictor of overall survival in classical LF-LG AS and adds incremental prognostic information beyond DSE peak LVEF.
Bergler-Klein J, Mundigler G, Pibarot P, et al. B-type natriuretic peptide in low-flow, low-gradient aortic stenosis: relationship to hemodynamics and clinical outcome. Circulation. 2007;115:2848–55.
Aksoy O, Cam A, Agarwal S, et al. Significance of aortic valve calcification in patients with low-gradient, low-flow aortic stenosis. Clin Cardiol. 2014;37(1):26–31. Patients with classical LF-LG severe AS with an AVC score > 2027 AU had a significantly worse survival compared to patients with an AVC score below this threshold.
Hayek S, Pibarot P, Harzand A. Dobutamine stress echocardiography for risk stratification of patients with low-gradient severe aortic stenosis undergoing TAVR. JACC Cardiovasc Imaging 2015;8(3):380-382. In 49 patients with severe LG AS undergoing transcatheter AVR (77% with LVEF<50%), the presence of CR predicted a better survival out to 2 years.
Quere JP, Monin JL, Levy F, et al. Influence of preoperative left ventricular contractile reserve on postoperative ejection fraction in low-gradient aortic stenosis. Circulation. 2006;113:1738–44.
O'Sullivan CJ, Stortecky S, Heg D, et al. Clinical outcomes of patients with low-flow, low-gradient, severe aortic stenosis and either preserved or reduced ejection fraction undergoing transcatheter aortic valve implantation. Eur Heart J. 2013;34:3437–50. Patients with severe LF-LG AS with and without reduced LVEF undergoing TAVR had overall mortality rates and symptomatic improvement comparable to patients with severe HG AS.
Herrmann HC, Pibarot P, Hueter I, et al. Predictors of mortality and outcomes of therapy in low-flow severe aortic stenosis: a Placement of Aortic Transcatheter Valves (PARTNER) trial analysis. Circulation. 2013;27:2316–26. In the Partner B trial, patients with severe LF-LG AS with and without reduced LVEF had a better 1 and 2-year survival with TAVR compared to medical therapy. In the randomized Partner A trial, 2-year survival in these two patient groups was similar with surgical AVR and TAVR.
Lauten A, Zahn R, Horack M, et al. Transcatheter aortic valve implantation in patients with low-flow, low-gradient aortic stenosis. JACC Cardiovasc Interv. 2012;5(5):552–9.
Gotzmann M, Lindstaedt M, Bojara W, Ewers A, Mugge A. Clinical outcome of transcatheter aortic valve implantation in patients with low-flow, low gradient aortic stenosis. Catheter Cardiovasc Interv. 2012;79:693–701.
Pibarot P, Weissman NJ, Stewart WJ, et al. Incidence and sequelae of prosthesis–patient mismatch in transcatheter versus surgical valve replacement in high-risk patients with severe aortic stenosis: a PARTNER trial cohort–analysis. J Am Coll Cardiol. 2014;64:1323–34.
Dumesnil JG, Pibarot P, Carabello B. Paradoxical low flow and/or low gradient severe aortic stenosis despite preserved left ventricular ejection fraction: implications for diagnosis and treatment. Eur Heart J. 2010;31:281–9.
Eleid MF, Sorajja P, Michelena HI, et al. Flow-gradient patterns in severe aortic stenosis with preserved ejection fraction: clinical characteristics and predictors of survival. Circulation. 2013;128:1781–9. Patients with severe LG AS with preserved LVEF and a NF-LG pattern were observed to have the highest event free survival, while patients with a LF-LG pattern had the worst outcome.
Maes F, Boulif J, Pierard S, et al. Natural history of paradoxical low gradient “severe” aortic stenosis. Circ Cardiovasc Imaging. 2014;7(4):714–22. The authors observed that 82% of patients with severe LG AS with preserved LVEF had an increase in MG during follow-up and 45% met HG criteria. These findings argue that these patients may not have a more advanced stage of disease, but may be a group progressing to severe HG AS with a potentially worse prognosis for other reasons.
Clavel MA, Dumesnil JG, Capoulade R, et al. Outcome of patients with aortic stenosis, small valve area, and low-flow, low-gradient despite preserved left ventricular ejection fraction. J Am Coll Cardiol. 2012;60:1259–67.
Dumesnil JG, Pibarot P. Letter by Dumesnil and Pibarot regarding article, “Outcome of patients with low-gradient “severe” aortic stenosis and preserved ejection fraction.”. Circulation. 2011;124:e360.
Eleid MF, Sorajja P, Michelena HI, Malouf JF, Scott CG, Pellikka PA. Survival by stroke volume index in patients with low-gradient normal EF severe aortic stenosis. Heart 2015;101(1):23-9. In severe LG AS with preserved LVEF, SVi is a strong predictor of outcome with the highest mortality observed in patients with SVi <35mL/m2. Patients with SVi between 35 and 43mL/m2 were also at increased risk.
Maor E, Beigel R, Grupper A, et al. Relation between stroke volume index to risk of death in patients with low-gradient severe aortic stenosis and preserved left ventricular function. Am J Cardiol. 2014;114(3):449–55.
Clavel MA, Ennezat PV, Maréchaux S, Dumesnil JG, Capoulade R, Hachicha Z, et al. Stress echocardiography to assess stenosis severity and predict outcome in patients with paradoxical low-flow, low-gradient aortic stenosis and preserved LVEF. JACC Cardiovasc Imaging. 2013;6:175–83. In severe LF-LG AS with preserved LVEF, an AVAproj threshold of 1.0 cm2 derived from exercise echocardiography or DSE could accurately distinguish patients with TSAS and PSAS. AVAproj was a strong predictor of AVR or death in follow-up.
Vinco G, Bergamini C, Pighi M, Golia G, Vassanelli C, Biancari F. Meta-analysis of the outcome of patients with low gradient severe aortic stenosis and preserved left ventricular ejection fraction. Int J Cardiol. 2013;168(5):5076–8. In a pooled meta-analysis of ten studies of patients with severe LG AS with preserved LVEF, survival was significantly better in patients undergoing AVR/TAVR compared to medical therapy.
Ozkan A, Hachamovitch R, Kapadia SR, Tuzcu EM, Marwick TH. Impact of aortic valve replacement on outcome of symptomatic patients with severe aortic stenosis with low gradient and preserved left ventricular ejection fraction. Circulation. 2013;128:622–31. AVR is associated with better survival than medical therapy in patients with symptomatic severe LG AS with preserved LVEF with both a NF-LG or LF-LG pattern.
Biner S, Birati EY, Topilsky Y, et al. Outcome of transcatheter aortic valve implantation in patients with low-gradient severe aortic stenosis and preserved left ventricular ejection fraction. Am J Cardiol. 2014;113:348–54. TAVR results in similar hemodynamic and long-term clinical outcomes in high-risk surgical patients with severe LG AS as those with severe HG AS.
Lauten A, Figulla HR, Möllmann H, et al. TAVI for low-flow, low-gradient severe aortic stenosis with preserved or reduced ejection fraction: a subgroup analysis from the German Aortic Valve Registry (GARY). EuroIntervention. 2014;10:850–59. In the German Aortic Valve Registry (GARY), severe LF-LG AS with preserved LVEF had a similar outcome as severe HG AS in the first year following TAVR. In contrast, severe LF-LG AS with reduced LV function was associated with a higher mortality.
Tarantini G, Covolo E, Razzolini R, et al. Valve replacement for severe aortic stenosis with low transvalvular gradient and left ventricular ejection fraction exceeding 0.50. Ann Thorac Surg. 2011;91:1808–15.
Grupper A, Beigel R, Maor E, et al. Survival after intervention in patients with low gradient severe aortic stenosis and preserved left ventricular function. J Thorac Cardiovasc Surg. 2014;148:2823–7. In patients with severe LG AS with preserved LVEF, the presence of a low or normal SVI did not affect the mortality benefit of an aortic valve intervention.
Compliance with Ethics Guidelines
Conflict of Interest
Dr. Katie M. Doucet and Dr. Ian G. Burwash each declare no potential conflicts of interest
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Valvular Heart Disease
Rights and permissions
About this article

Cite this article
Doucet, K.M., Burwash, I.G. Low Gradient Aortic Stenosis. Curr Treat Options Cardio Med 17, 20 (2015). https://doi.org/10.1007/s11936-015-0378-x
Published:
DOI: https://doi.org/10.1007/s11936-015-0378-x