
Abstract
Purpose of Review
We review pathophysiology and clinical features of mitochondrial disorders manifesting with cardiomyopathy.
Recent Findings
Mechanistic studies have shed light into the underpinnings of mitochondrial disorders, providing novel insights into mitochondrial physiology and identifying new therapeutic targets.
Summary
Mitochondrial disorders are a group of rare genetic diseases that are caused by mutations in mitochondrial DNA (mtDNA) or in nuclear genes that are essential to mitochondrial function. The clinical picture is extremely heterogeneous, the onset can occur at any age, and virtually, any organ or tissue can be involved. Since the heart relies primarily on mitochondrial oxidative metabolism to fuel contraction and relaxation, cardiac involvement is common in mitochondrial disorders and often represents a major determinant of their prognosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mitochondrial disorders are rare genetic diseases, with an estimated prevalence of 10 to 15 cases per 100,000 persons [1], that are characterized by defective mitochondrial oxidative metabolism [2]. Affected genes encode for components of the respiratory chain or proteins involved in mitochondrial DNA replication, mitochondrial dynamics, oxidative metabolism, or the provision of enzyme cofactors. Pathogenic gene variants occur either in mitochondrial or nuclear DNA (mtDNA and nDNA, respectively) and therefore can have any pattern of inheritance — maternal for mtDNA mutations and autosomal or X-linked for nDNA variants. The involvement of certain sets of genes in the development of mitochondrial disorders, including genes encoding fatty acid oxidation enzymes, is currently a matter of debate [3, 4••, 5, 6] [7].
The clinical picture of mitochondrial disorders is extremely heterogeneous, the onset can occur at any age, and any organ or tissue can be involved. Mitochondrial disorders can manifest with a severe multisystemic involvement early in life, often characterized by nonspecific clinical features such as hypotonia, failure to thrive, seizures, and encephalopathy. Alternatively, the disease can present later, from teenage years to adulthood, with a milder, sometimes progressive single-organ or multiorgan involvement. Typical features are exercise intolerance and fatigue, sensorineural hearing loss, and endocrinopathies such as diabetes mellitus. Physiologic stressors such as fever can precipitate cardiac dysfunction and metabolic crisis. The heterogenous clinical picture often makes it difficult to categorize the patient in one definite syndrome. Mutations in the same gene can even cause different disease phenotypes: mutations in the gene encoding the mitochondrial DNA polymerase γ (POLG), the polymerase that is responsible for replication and repair of mtDNA, can cause a wide range of phenotypes from early-onset hepatocerebral disease, juvenile epilepsy, or adult ataxia-neuropathy syndrome [8, 9].
Organs that rely primarily on oxidative phosphorylation for adenosine triphosphate (ATP) production, such as the heart and the central nervous system, are frequently involved. Cardiac involvement in mitochondrial disorders is common, and its phenotype and severity are variable [10••]. Both hypertrophic and dilated cardiomyopathy can occur, and the clinical expression ranges from asymptomatic systolic dysfunction to end-stage heart failure requiring heart transplantation in infancy. Left ventricular (LV) non-compaction, an abnormality characterized by the persistence of a prominent trabecular meshwork in the ventricular wall, has been often associated with mitochondrial disorders and can be accompanied by LV dilatation or hypertrophy [11]. Non-compaction probably results from an abnormal morphogenesis of the endomyocardial layer, and its occurrence in mitochondrial disorders might reflect the important role played by mitochondria in cardiac development. Conduction abnormalities have also been associated with mitochondrial disease and are particularly common with certain syndromes, such as Kearns-Sayre.
In this review, we discuss mechanisms and manifestations of cardiac involvement in mitochondrial disorders. We focus on the most common syndromes and on those disorders characterized by a high frequency and severity of cardiac involvement, with a special focus on disorders caused by altered cardiolipin remodelling.
Pathophysiology of Mitochondrial Disorders
Mitochondrial DNA
Mitochondria originated from aerobic bacteria that were engulfed by- and evolved in symbiosis with one ancestral anaerobic cell. Mitochondria retain some genes as vestiges of their bacterial progenitors encoded on their mtDNA and machineries for gene transcription and protein translation [12]. The mtDNA is maternally inherited and features a circular DNA formed by two strands, one heavy, guanine-rich strand (H) and one light strand (L). It contains the genetic information for 13 core components of the respiratory chain complexes, 22 transfer RNAs (mt-tRNA), and 2 ribosomal RNAs (mt-rRNA) [13,14,15]. Therefore, of > 1500 proteins contained in human mitochondria, only 13 are encoded by mtDNA genes, while the remaining are found encoded by the nuclear DNA. Due to the coexistence of 500 or more mtDNA molecules per cell, a phenomenon termed heteroplasmy, mitochondrial genetics operate on population-based (instead of Mendelian) principles [16, 17•]. Mitochondrial genes are particular vulnerable to mutations due to the close proximity of mtDNA to sites of reactive oxygen species (ROS) production and lack of protective histones and poor DNA repair mechanisms [13]. Interestingly, the frequency of mitochondrial mutations exceeds by far the incidence of mitochondrial disease, indicating that observable phenotypes only occur when a mutation reaches a certain threshold [18]. While the mechanisms governing mitotic segregation of mtDNA are poorly understood, this process might not result uniquely from random genetic drift — on the contrary, experimental evidence demonstrates the occurrence of tissue-specific and age-related directional selection for certain mtDNA genotypes in the same organism [19]. Moreover, in circulating blood cells, a selective recognition of mtDNA by the innate immune system has been observed [20]. As a result of these factors, the wild type-to-mutant mtDNA ratio varies from tissue to tissue and even from cell to cell [21, 22•]. The threshold at which one mtDNA mutation results in cellular defects depends on the mutation itself and the cell type. The high reliance of the heart and central nervous system on aerobic metabolism might decrease the proportion of mutant mtDNA required for disease manifestation to arise [7].
ATP and Reactive Oxygen Species Production at the Respiratory Chain
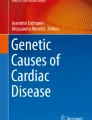
One central function of mitochondria is the production of adenosine triphosphate (ATP) via oxidative phosphorylation. This process entails the transfer of electrons across a series of protein complexes embedded in the inner mitochondrial membrane, the electron transport chain complexes (ETC), which harness the energy derived from sequential oxidation steps to pump protons from the mitochondrial matrix to the intermembrane space (Fig. 1). The resulting chemical and electrical potential, termed the protonmotive force, is used by the F1-Fo ATP synthase to catalyse ADP phosphorylation and drives many essential mitochondrial functions such as metabolite, ion, and protein transport across the inner mitochondrial membrane [24, 25]. Organs with a very high ATP demand, such as the heart and the central nervous system, mainly rely on oxidative phosphorylation to maintain their function, and the failure to generate sufficient ATP is considered the primary driver of disorders caused by mutations in the mtDNA or in nuclear genes encoding respiratory chain components [26].

Mechanisms of mitochondrial dysfunction in inherited mitochondrial disorders. Created with BioRender.com. Abbreviations: AGK, acylglycerol kinase; ANT1, adenine nucleotide translocator 1; CACT, carnitine-acylcarnitine translocase; CL, cardiolipin; CPT1/2, carnitine palmitoyltransferase 1/2; DCMA, dilated cardiomyopahty with ataxia; ETC, electron transport chain; FA-CoA, fatty acyl-CoA; FXN, frataxin; LHON, Leber’s hereditary optic neuropathy; OXPHOS, oxidative phosphorylation; TAZ, tafazzin
Molecular oxygen (O2) is the final acceptor of electrons at the respiratory chain. The high affinity of O2 for electrons explains the large amount of energy released by the process of electron transfer at the ETC. Incomplete reduction of O2, however, can lead to the production of the highly reactive superoxide radical (O2−), which has a strong tendency to subtract electrons from proteins, lipids, and nucleic acids. To protect the cell from the potentially devastating consequences of mitochondrial oxidative stress, mitochondria are equipped with an efficient antioxidant machinery [27]. First, superoxide is converted to hydrogen peroxide (H2O2) by the manganese-dependent superoxide dismutase (Mn-SOD). Subsequently, H2O2 is reduced to H2O by matrix peroxidases, including peroxiredoxin (Prx) and glutathione peroxidases (Gpx). The reducing equivalents required for H2O2 elimination by Prx and Gpx derive from a cascade of redox reactions that are replenished by the activity of the Krebs cycle [28]. Therefore, mitochondrial oxidative metabolism is essential both for ATP production at the ETC and protect the cell from mitochondrial ROS-induced damage. As mitochondrial ROS play a role as a signalling molecule, changes in ROS can also affect signalling pathways to control metabolism, proliferation, and differentiation [29]. Therefore, a tight control of ROS is important to maintain cellular and organismal homeostasis. Oxidative stress has been implicated in the pathophysiology of many mitochondrial disorders, a notion that has been mostly supported by in vitro models of disease [30]. In principle, any mutation affecting the structure and function of the ETC can increase mitochondrial superoxide production at the respiratory chain, overwhelming mitochondrial antioxidant systems.
Besides their role in energy and redox homeostasis, mitochondria also play a central role in synthesizing amino acids, enzyme cofactors such as heme, and iron-sulphur clusters, and are central players in cellular ion handling [31]. Mitochondria are essential modulators of Ca2+ dynamics as membrane-bound Ca2+ pumps are ATP- and ROS-dependent [32]. In turn, Ca2+ concentrations in the mitochondrial matrix modulate oxidative metabolism by regulating the activity of the rate-limiting enzymes of the Krebs cycle [28, 33].
Disorders Caused by mt-tRNA Mutations
MELAS and MERRF
Mitochondrial encephalopathy, lactic acidosis, and stroke-like episodes (MELAS) and myoclonic epilepsy with ragged red fibres (MERRF) are predominantly caused by pathogenic mutations in genes encoding for mt-tRNA, albeit rare cases associated with mutations in mt-rRNA genes were described. The most common (~ 80%) pathogenic mutation found in patients with MELAS involves the transition from adenine to guanine at position 3243 (m.3243A > G), which disrupts the mitochondrial leucyl-tRNA gene, MT-TL1. The consequent defect in mitochondrial oxidative metabolism uncouples glycolysis from oxidation of pyruvate, which is therefore converted into lactate leading to lactic acidosis [34,35,36]. Mutations in the mitochondrial lysil-tRNA gene MT‐TK account for more than 90% of MERFF cases [37]. Both MELAS and MERFF are polygenic disorders, and mutations causing MELAS can also give rise to different phenotypes, such as Leigh syndrome and chronic progressive external ophthalmoplegia [22•].
Three key features are deemed necessary for the diagnosis of MELAS: (i) stroke-like episodes before the age of 40; (ii) encephalopathy characterized by seizures, dementia, or both; and (iii) lactic acidosis, presence of ragged-red fibres, or both [38]. The spectrum of central and peripheral nervous system involvement is wide and includes cognitive impairment in infancy, visual or auditory sensual deficiencies, and peripheral neuropathy. Furthermore, endocrine manifestations such as diabetes mellitus, renal involvement in the form of Fanconi disease, and gastrointestinal abnormalities have been associated with MELAS [39].
Cardiac involvement in MELAS occurs in ~ 55% of patients and manifests with cardiomyopathy and/or conduction defects [40•]. Hypertrophic cardiomyopathy is more common than dilated cardiomyopathy, and both phenotypes can present in association with LV non-compaction. Conduction defects include ventricular pre-excitation and atrio-ventricular block. A meta-analysis assessing the frequency of cardiac involvement in mitochondrial myopathies found that patients with MELAS have the highest prevalence of EKG and echocardiographic abnormalities compared with other mitochondrial disorders, and cardiac manifestations in infancy portend a more severe phenotype with an increased mortality rate [40•, 41••].
MERFF is a neuromuscular disorder with multisystemic involvement varying from myoclonus, cerebellar ataxia, dementia, and muscle weakness to peripheral neuropathy, respiratory dysfunction, cardiomyopathy, and lipomas [42]. Cardiac involvement occurs in 44–57% of MERFF cases [43, 44], and hypertrophic and dilated cardiomyopathy appear to be equally common [45]. Prevalence of arrhythmic events seems to be lower than in MELAS, the most common being Wolff-Parkinson-White syndrome [44].
Disorders Caused by Defects in the Electron Transport Chain
Leigh Syndrome
Leigh syndrome or subacute necrotizing encephalopathy is the most common presentation of a mitochondrial disease in infancy and typically caused by mutations in at least 75 different mtDNA and nDNA genes. Mutations in mtDNA account for 20–25% of Leigh syndrome cases and affect the function of either complex I or complex V of the respiratory chain, while the remaining 75–80% result from nDNA mutations, the majority of which lead to decreased protein levels and/or activity of cytochrome c oxidase (complex IV) [46].
Mice lacking the complex I subunit Ndufs4 (Ndufs4−/− mice) exhibit an extensive remodelling of metabolic pathways driven by the activation of the metabolic sensor mechanistic target of rapamycin (mTOR). Inhibition of mTOR with rapamycin delayed disease progression in Ndufs4−/− mice [47, 48]. In addition, loss of complex I activity leads to accumulation of NADH, resulting in an increased NADH/NAD+ ratio. Because deacetylation is a NAD+-dependent process, the shift in the NADH/NAD+ ratio results in hyperacetylation and consequent functional changes in numerous proteins, including the cardiac sodium channel NaV1.5. On these grounds, supplementation with the NAD precursor nicotinamide riboside (NR) was proposed as a therapeutic strategy to prevent arrhythmia in Leigh syndrome [49].
Leigh syndrome is characterized by progressive cognitive decline, hypotonia, psychomotor disability, ataxia, and high levels of lactate detectable both in blood and cerebrospinal fluid [50, 51]. Disease onset is usually at 2 years of age, reaching peak mortality towards the age of 3. Neurogenic muscle weakness, ataxia, and retinitis pigmentosa (NARP), a disorder characterized by a later onset and dominated by ataxia and peripheral neuropathy, is considered a clinical continuum with maternally inherited Leigh syndrome. The latter, however, is far more severe and lethal, a difference that might be explained by the higher proportion of mutant mtDNA observed in NARP [51, 52].
Cardiac involvement represents the most common non-neurological manifestation of the disease [53]. In a multi-centric study involving 96 patients with Leigh syndrome, cardiac involvement in the form of cardiomyopathy, arrhythmia, conduction defects, or valve disease was identified in 18 patients. Cardiomyopathy, both hypertrophic and dilated, was diagnosed in 10% of the cohort and more frequent among patients carrying mtDNA mutations than in those with nDNA mutations [54•].
Leber’s Hereditary Optic Neuropathy
Leber’s hereditary optic neuropathy (LHON) is a maternally inherited disorder that in 95% of cases is caused by one of three mutations in mtDNA genes encoding subunits of complex I of the respiratory chain [55]. Complex I dysfunction leads to increased ROS emission and defective ATP production, which are considered the main drivers of disease progression. Oxidative stress and bioenergetic deficit cause cell death by triggering the opening of a large pore in the mitochondrial membranes, the permeability transition pore, which irreversibly dissipates the proton-motive force and releases proapoptotic factors into the cytosol [55, 56, 57].
For yet unknown reasons, the penetrance of LHON is higher in men than in women (45% vs 10%, respectively). Environmental factors, such as smoking and alcohol consumption, appear to double the risk of disease manifestation [58•, 59]. The typical presentation is subacute, one-sided loss of vision occurring in the absence of pain, starting with a centrally located scotoma that progressively involves the entire visual field [55, 56, 60]. Although single-organ involvement is common, cardiac and myopathic manifestations have also been reported. Among cardiac manifestations, arrhythmias and conduction defects have the highest prevalence (15–50% of the cases) [60, 61].
Kearns-Sayre Syndrome
Kearns-Sayre syndrome (KSS) is caused by large mtDNA deletions that give rise to progressive external ophthalmoplegia and retinitis pigmentosa before 20 years of age. In addition to these two features, at least one between cardiac conduction defects, cerebellar ataxia, or increased protein levels in the cerebrospinal fluid (> 100 mg/dL) is required to establish diagnosis [62]. KSS involves the heart in ~ 50% of cases and primarily affects the cardiac conduction system [63]. Conduction abnormalities usually occur after the onset of ocular involvement and can present with syncope or sudden cardiac death. Severe forms of dilated cardiomyopathy have also been described in KSS [64,65,66].
Disorders Caused by Defective Cardiolipin Remodelling
Cardiolipin Function
The inner mitochondrial membrane (IMM) has the highest density of embedded proteins among cellular membranes. The integrity, fluidity, and phospholipid composition of the IMM is pivotal to maintain the architecture and function of membrane-embedded protein complexes, including the ETC. Cardiolipin (CL) is a phospholipid that is almost exclusively found in the IMM, where it plays a role in numerous key mitochondrial processes by interacting with several IMM protein complexes. For instance, CL stabilizes the ETC in larger macromolecular complexes termed “respirasomes,” facilitating the electron transfer process and thereby, maintaining respiratory efficiency or “coupling.” Furthermore, CL is abundant near the tips of the mitochondrial cristae, where it contributes to the curvature of the IMM and favours ATP synthase dimerization to maximize ATP synthesis [67]. CL is formed by a polar glycerol head to which four fatty acyl chains are attached. After biosynthesis, CL undergoes a process known as remodelling, which involves the substitution of the saturated acyl chains of “premature” CL with polyunsaturated acyl species. The different CL composition might account for a more or less condensed architecture of mitochondrial cristae in different tissues [70, 71•]. Furthermore, the process of CL remodelling is pivotal to allow the interaction of CL with proteins and the crowding of proteins in the IMM.
Mitochondrial disorders caused by abnormal CL composition are caused by nDNA mutations in genes encoding enzymes involved in CL biosynthesis and remodelling. This group of disorders includes at least three syndromes, i.e., Sengers syndrome, dilative cardiomyopathy with ataxia (DCMA), and Barth syndrome, whose dominant features are cardiomyopathy and skeletal myopathy. These disorders were initially classified together with inborn errors of metabolism characterized by increased urinary 3-methylglutaconic acid excretion, which is also observed in a minority of patients with other disorders of oxidative phosphorylation, but is especially common in Barth syndrome and DCMA. Overall, cardiomyopathy is a hallmark of disorders caused by defective CL remodelling, demonstrating the pivotal role of this phospholipid for mitochondrial function in the heart [68•, 69].
Barth Syndrome
Barth syndrome is caused by mutations in the gene encoding tafazzin [72], a mitochondrial transacylase ubiquitously expressed in human tissues which catalyses the final step in the remodelling of CL [73]. In Barth syndrome, abnormal CL remodelling alters CL-protein interaction, causing the accumulation of more saturated CL species and accelerating CL turnover [74].
Barth syndrome is characterized by the infantile onset of cardiomyopathy, skeletal myopathy, recurrent neutropenia, and retarded growth [75]. The most common cause of death in Barth syndrome is cardiomyopathy, which can manifest as hypertrophic or dilated cardiomyopathy, often (50%) associated with LV noncompaction. Cardiac involvement can present with severe LV dysfunction and heart failure in the first years of life [76]. A sizable proportion of Barth syndrome patients, however, develop a milder form of cardiomyopathy, with preserved (i.e., > 50%) or only mildly reduced (40–50%) LV ejection fraction (LVEF) and impaired LV relaxation. Overall, patients developing a reduced LVEF are more prone to cardiovascular events, including arrhythmias and sudden cardiac death, whereas those with preserved LVEF are mainly symptomatic because of exercise intolerance and fatigue [76, 77]. These symptoms have been attributed to the marked reduction in cardiac contractile reserve and impaired skeletal muscle oxidative metabolism in Barth syndrome [78].
Mechanistic insights into the pathophysiology of Barth syndrome cardiomyopathy were obtained by two different mouse models of the disease, the tafazzin-knockdown (Taz-KD) and -knockout (Taz-KO) models. While Taz-KO mice are characterized by embryonic lethality, impaired growth, and dilated cardiomyopathy with severe systolic dysfunction [79], Taz-KD exhibit only a mild reduction in LVEF and a limited inotropic reserve, recapitulating the phenotype of those Barth syndrome patients who do not develop (or recover from) severe HF during infancy [80••].
In the Taz-KD model, we discovered that altered CL remodelling causes not only changes in the respiratory chain but also alters the structural organization of the mitochondrial Ca2+ uniporter, a Ca2+ channel embedded in the IMM [80••]. These structural changes hinder mitochondrial calcium (Ca2+) uptake. Under physiological conditions, Ca2+ accumulation in the mitochondrial matrix stimulates the Krebs cycle dehydrogenases, thereby accelerating ATP production when an elevation in cardiac workload increases ATP consumption in the cytosol [81]. In Barth syndrome, the Ca2+-dependent stimulation of mitochondrial oxidative metabolism is lost, contributing to the reduced contractile reserve and the consequent exercise intolerance (Fig. 2). In addition, Taz-KD mice also exhibit elevated myofilament Ca2+ affinity and slowed cross-bridge cycling, which hinders myocardial relaxation and imposes an additional ATP demand during diastole. Although evidence of diastolic dysfunction in patients is scant, these results indicate that impaired myocardial relaxation might contribute to the manifestation of cardiomyopathy in Barth syndrome [80••].

Defects in cardiac excitation–contraction coupling and cellular calcium handling in Barth syndrome. Created with BioRender.com. Abbreviations: ETC, electron transport chain; MCU, mitochondrial calcium uniporter; TAZ, tafazzin
Investigations in rodent models of the disease have also revealed two distinct and possibly complementary mechanisms explaining the increased susceptibility to arrhythmias and sudden cardiac death in Barth syndrome [82]. First, the defect in mitochondrial Ca2+ uptake may contribute to this risk by causing mitochondrial oxidation that triggers arrhythmias in isolated cardiac myocytes and slows conduction in whole hearts [80••]. Furthermore, in the Taz-KO model, high levels of mitochondrial ROS activate the Ca2+/calmodulin-dependent protein kinase II (CaMKII), which phosphorylates the ryanodine receptor 2 (RyR2), i.e., the Ca2+ channel that mediates Ca2+ efflux from the sarcoplasmic reticulum. RyR2 phosphorylation leads to spontaneous Ca2+ release events from the sarcoplasmic reticulum, altering cellular Ca2+ handling and causing afterdepolarization events that represent a trigger for ventricular arrhythmias [83].
One unresolved issue concerns the role of oxidative stress in the pathogenesis of Barth syndrome cardiomyopathy. In vitro studies implicated ROS production at the ETC as one key driver of the disease [84, 85], which is in line with observations in the Taz-KO model. In contrast, Taz-KD mice do not display signs of oxidative stress in the heart, and genetic or pharmacological interventions targeting ROS production did not rescue cardiac dysfunction in this model [80••, 86]. In Barth syndrome patients, treatment with the small peptide elamipretide (also known as SS-31, MTP-131 or Bendavia), which prevents ROS formation at the ETC by selectively targeting CL, did not meet the primary endpoint in a 4-week, double-blind, placebo-controlled crossover trial, but it did improve physical performance in the trial open-label extension [87].
Overall, the Taz-KD and Taz-KO models exhibit remarkable differences in their cardiac phenotype that might reflect the heterogeneity of disease manifestations and mechanisms at play in Barth syndrome cardiomyopathy. Future investigations should be aimed at addressing the underpinnings of this heterogeneity, which probably involves interactions of tafazzin mutations with the genetic background of the patients.
Sengers Syndrome
Sengers syndrome is an autosomal recessive disorder caused by mutations in the gene encoding acylglycerol kinase (AGK) [88]. AGK is located within the IMM and has two known functions: it is a phospholipid kinase that synthesizes phosphatidic acid, a precursor of CL, and a component of the membrane translocase complex TIM22, which mediates the import of mitochondrial membrane proteins that are synthesized in the cytosol. This moonlight function of AGK might explain the wide spectrum of mitochondrial abnormalities observed in Sengers syndrome [89, 90]. One prominent defect is decreased activity of the mitochondrial adenine nucleotide translocator (ANT1), which was initially considered the primary cause of the disease.
The clinical picture of Sengers syndrome is characterized by congenital cataracts, hypertrophic cardiomyopathy, skeletal myopathy, and lactic acidosis [88]. Similar to Barth syndrome, Sengers syndrome can present with an extremely severe form of hypertrophic cardiomyopathy in newborns, which portends an extremely poor prognosis, or as a late-onset, milder form with a life expectancy exceeding the fifth decade of life [91,92,93].
Dilated Cardiomyopathy with Ataxia
DCMA is an autosomal recessive monogenic disorder caused by variants in the DNAJC19 gene, which were identified and are especially frequent in the Canadian Dariusleut Hutterite population [94, 95]. Most pathogenic variants in DNAJC19 are truncating, and thus result in a shorter version of the protein [94, 96, 97]. DNAJC19 is a component of the presequence protein translocase and shows sequence similarity with the yeast J domain protein Pam18/Tim14 [98•, 99]. Besides its role in mitochondrial protein transport, DNAJC19 was also found to interact with membrane proteins of the prohibitin family [100]. Prohibitins form a large complex in the inner membrane, which serves as a structural scaffold involved in CL metabolism. DNAJC19-deficient cells show altered CL levels [100]. Therefore, akin to Barth syndrome, the clinical picture of DCMA arises from abnormalities in the CL composition in the IMM [100, 101].
DCMA manifests with early-onset dilated cardiomyopathy, conduction defects, growth failure, ataxia, male genital anomalies, and developmental defects. LV non-compaction and oculomotor apraxia have also been associated with DCMA [102]. Cardiac involvement is often severe, with a reported 50% mortality due to congestive heart failure or arrhythmias at the mean age of 22 months [103].
Disorders Caused by Defective Fatty Acid Oxidation
Fatty acid oxidation disorders comprise defects in fatty acid import in the mitochondrial matrix via the carnitine shuttle and abnormalities in mitochondrial β-oxidation (Fig. 1). Disease manifestations are attributed to defective mitochondrial ATP production, and therefore, certain features recapitulate those of other mitochondrial disorders [104,105,106,107,108]. Moreover, defects in fatty acid oxidation can induce extensive metabolic remodelling causing increased systemic demand for pyruvate and trigger stress responses due to altered amino acid metabolism [109]. However, one additional pathogenic mechanism that is specific for fatty acid oxidation disorders is the accumulation of toxic long-chain CoA-esters or their free long-chain fatty acids, which perturb cellular function by lowering cytosolic pH, suppressing intermediary metabolism, or causing oxidative stress via lipid peroxidation [110••, 111].
Cardiomyopathy and metabolic crisis secondary to liver failure are among the most severe and precocious manifestations of these disorders, whereas exercise intolerance and rhabdomyolysis may appear later in infancy [106]. Disease onset might be abrupt and can be elicited by a variety of stressors. Late-onset CPT2 deficiency is the most common genetic cause of rhabdomyolysis in adults, and exercise is the most frequent trigger of rhabdomyolysis in these patients. Other triggers of metabolic decompensation include viral infections, fasting, colds, general anaesthesia, and sleep deprivation [112].
Friedreich’s Ataxia
Friedreich’s ataxia (FRDA) is the most prevalent cause of hereditary ataxia among individuals of European descent, affecting around 1 in 40,000 subjects. FRDA is an autosomal recessive disorder that usually manifests between 10 and 15 years of age. Its symptoms include progressive ataxia, dysarthria, vision and hearing loss, muscle weakness, musculo-skeletal abnormalities such as scoliosis [113], diabetes mellitus, and hypertrophic cardiomyopathy [114]. The cause is a homozygous GAA triplet repeat in the first intron of the FXN gene, which encodes for the mitochondrial protein frataxin [115]. FXN alleles contain > 70 GAA repeats that interfere with gene transcription by heterochromatin silencing, leading to loss of frataxin protein.
Frataxin is a mitochondrial iron-binding protein that is crucially involved in the assembly and repair of iron-sulphur clusters which operate as cofactors in a number of fundamental cellular processes, including oxidative phosphorylation, the Krebs cycle, and enzymes such as aconitase [116]. Accordingly, endomyocardial biopsies of FRDA patients demonstrated a reduced activity of mitochondrial respiratory chain complexes I, II and III. It has been proposed that the ferroxidase activity of frataxin might help reduce the concentration of chelatable iron and prevent this metal from producing ROS [117]. Deregulation of the antioxidant transcription factor nuclear factor-E2-related factor-2 (NRF2) and reduced expression of peroxiredoxins, glutaredoxins, and glutathione S-transferase causes depletion of antioxidants and, consequently, an increase in lipid peroxidation[118, 119]. Lipid peroxidation resulting from iron accumulation and depletion of antioxidant systems are crucial triggers of ferroptosis, a type of programmed cell death [120]. In fact, fibroblasts derived from FRDA patients and from FRDA mouse models are hypersensitive to drug-induced ferroptosis and rescued by specific ferroptosis inhibitors [121].
Although central nervous system involvement dominates the clinical presentation of FRDA, cardiovascular involvement dictates its prognosis, accounting for ~ 59% of deaths among FRDA patients [122]. The prognosis is particularly poor for those with progressive LV systolic dysfunction [123]. Cardiac involvement in FRDA is characterized by concentric LV hypertrophy occurring without outflow tract obstruction and with an end-diastolic wall thickness < 15 mm in the majority of cases [124, 125•].
One longitudinal study with a 10-year follow-up period described two distinct cardiac trajectories in FRDA patients: a larger low-risk group with normal LV systolic function at baseline, which slightly decreased over time but remained within normal range, and a smaller high-risk group exhibiting a progressive decline in LVEF. Of note, there was a positive correlation between the size of the expanded GAA repeat and the risk of cardiac complications [126]. Over time, wall thickness tends to decrease and LV dilatation ensues, and ultimately ~ 20% exhibit a reduced LVEF [127]. In advanced stages of the disease, the onset of atrial fibrillation can additionally deteriorate systolic function and lead to heart failure [122].
Late-onset (LOFA, onset > 25 years) and very late-onset FRDA (VLOFA, onset > 40 years) were described as rare variants of the disease. FRDA cases with delayed onset exhibit a milder phenotype, a slower rate of disease progression, and a more diverse spectrum of signs and symptoms. Akin to “typical” FRDA, the most frequent presenting signs are gait and limb ataxia, but dysarthria often appears later and spasticity is more common, while the prevalence of non-neurologic symptoms such as cardiomyopathy or diabetes mellitus is lower [128]. At the other end of the spectrum, patients with early onset of FRDA (< 5 years of age) exhibit a more severe phenotype and a poorer prognosis. Again, the size of the expanded GAA repeat correlates with the onset and severity of the clinical presentation [129].
Conclusions
Cardiac involvement in mitochondrial disorders is common and often severe. In spite of the advances in the understanding of the mechanism of disease, many of these disorders are orphan of treatment and their prognosis remains poor. Only few therapeutic agents are approved for the treatment of mitochondrial diseases [130]. This unmet medical need has stimulated research for novel disease mechanism and novel therapeutic options. Development of zinc-finger nucleases (ZFNs), transcription activator-like effector nuclease (TALENS), and Crispr-Cas9 allows manipulation of the mitochondrial genome [131, 132]. More research is necessary for the development of innovative treatments for rare mitochondrial disorders.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Chinnery PF, Turnbull DM. Epidemiology and treatment of mitochondrial disorders. Am J Med Genet. 2001;106(1):94–101.
DiMauro S, Schon EA. Mitochondrial respiratory-chain diseases. N Engl J Med. 2003;348(26):2656–68.
Frazier AE, Thorburn DR, Compton AG. Mitochondrial energy generation disorders: genes, mechanisms, and clues to pathology. J Biol Chem. 2019;294(14):5386–95.
Gorman GS, Chinnery PF, DiMauro S, Hirano M, Koga Y, McFarland R, et al. Mitochondrial diseases. Nat Rev Dis Prim. 2016;2(1):1–22.
Rahman S. Mitochondrial disease in children. J Intern Med. 2020;287(6):609–33.
Stenton SL, Prokisch H. Genetics of mitochondrial diseases: identifying mutations to help diagnosis. EBioMedicine. 2020;56:102784.
Schlieben LD, Prokisch H. The dimensions of primary mitochondrial disorders. Front Cell Dev Biol. 2020;8:600079.
Hakonen AH, Heiskanen S, Juvonen V, Lappalainen I, Luoma PT, Rantamäki M, et al. Mitochondrial DNA polymerase W748S mutation: a common cause of autosomal recessive ataxia with ancient European origin. Am J Hum Genet. 2005;77(3):430–41.
Van Goethem G, Dermaut B, Löfgren A, Martin J-J, Van Broeckhoven C. Mutation of POLG is associated with progressive external ophthalmoplegia characterized by mtDNA deletions. Nat Genet. 2001;28(3):211–2.
Meyers DE, Basha HI, Koenig MK. Mitochondrial cardiomyopathy: pathophysiology, diagnosis, and management. Tex Heart Inst J. 2013;40(4):385–94.
Towbin JA, Ballweg J, Johnson J. Chapter 20 - Left Ventricular Noncompaction Cardiomyopathy, editors. John L. Jefferies, Anthony C. Chang, Joseph W. Rossano, Robert E. Shaddy, Jeffrey A. Towbin, Heart Failure in the Child and Young Adult, Academic Press, 2018. pp. 269–90. https://doi.org/10.1016/B978-0-12-802393-8.00020-X.
Schleiff E, Becker T. Common ground for protein translocation: access control for mitochondria and chloroplasts. Nat Rev Mol Cell Biol. 2011;12(1):48–59.
Kazuhito T, Wei FY. Posttranscriptional modifications in mitochondrial tRNA and its implication in mitochondrial translation and disease. J Biochem. 2020;168(5):435–44.
Sharma P, Sampath H. Mitochondrial DNA integrity: role in health and disease. Cells. 2019;8(2):100.
Yan C, Duanmu X, Zeng L, Liu B, Song Z. Mitochondrial DNA: distribution, mutations, and elimination. Cells. 2019;1:1–15.
Satoh M, Kuroiwa T. Organization of multiple nucleoids and DNA molecules in mitochondria of a human cell. Exp Cell Res. 1991;196(1):137–40.
DiMauro S, Schon EA, Carelli V, Hirano M. The clinical maze of mitochondrial neurology. Nat Rev Neurol. 2013;9(8):429–44.
Schon EA, DiMauro S, Hirano M. Human mitochondrial DNA: roles of inherited and somatic mutations. Nat Rev Genet. 2012;13(12):878–90.
Jenuth JP, Peterson AC, Shoubridge EA. Tissue-specific selection for different mtDNA genotypes in heteroplasmic mice. Nat Genet. 1997;16(1):93–5.
Ishikawa K, Toyama-Sorimachi N, Nakada K, Morimoto M, Imanishi H, Yoshizaki M, et al. The innate immune system in host mice targets cells with allogenic mitochondrial DNA. J Exp Med. 2010;207(11):2297–305.
Gustafsson CM, Falkenberg M, Larsson NG. Maintenance and Expression of Mammalian Mitochondrial DNA. Annu Rev Biochem. 2016;85:133–60.
Sproule DM, Kaufmann P. Mitochondrial encephalopathy, lactic acidosis, and strokelike episodes: Basic concepts, clinical phenotype, and therapeutic management of MELAS syndrome. Ann N Y Acad Sci. 2008;1142:133–58.
Moreira JD, Gopal DM, Kotton DN, Fetterman JL. Gaining insight into mitochondrial genetic variation and downstream pathophysiology: What can i(pscs) do? Genes (Basel). 2021;12(11):1668.
Neupert W, Herrmann JM. Translocation of proteins into mitochondria. Annu Rev Biochem. 2007;76(1):723–49.
Mitchell P. Coupling of phosphorylation to electron and hydrogen transfer by a chemi-osmotic type of mechanism. Nature. 1961;191(4784):144–8.
Lemieux H, Bulteau AL, Friguet B, Tardif J-C, Blier PU. Dietary fatty acids and oxidative stress in the heart mitochondria. Mitochondrion. 2011;11(1):97–103.
Balaban RS, Nemoto S, Finkel T. Mitochondria, oxidants, and aging. Cell. 2005;120(4):483–95.
Bertero E, Maack C. Calcium signaling and reactive oxygen species in mitochondria. Circ Res. 2018;122(10):1460–78.
Shadel GS, Horvath TL. Mitochondrial ROS signaling in organismal homeostasis. Cell. 2015;163(3):560–9.
Wu SB, Ma YS, Wu YT, Chen YC, Wei YH. Mitochondrial DNA mutation-elicited oxidative stress, oxidative damage, and altered gene expression in cultured cells of patients with MERRF syndrome. Mol Neurobiol. 2010;41(2–3):256–66.
Nunnari J, Suomalainen A. Mitochondria: in sickness and in health. Cell. 2012;148(6):1145–59.
Bayeva M, Sawicki KT, Butler J, Gheorghiade M, Ardehali H. Molecular and cellular basis of viable dysfunctional myocardium. Circ Hear Fail. 2014;7(4):680–91.
O’Rourke B, Kass DA, Tomaselli GF, Kääb S, Tunin R, Marbán E. Mechanisms of altered excitation-contraction coupling in canine tachycardia-induced heart failure, I: experimental studies. Circ Res. 1999;84(5):562–70.
Ciafaloni E, Ricci E, Shanske S, Moraes CT, Silvestri G, Hirano M, et al. MELAS: clinical features, biochemistry, and molecular genetics. Ann Neurol Off J Am Neurol Assoc Child Neurol Soc. 1992;31(4):391–8.
Koga Y, Nonaka I, Kobayashi M, Tojyo M, Nihei K. Findings in muscle in complex I (NADH coenzyme Q reductase) deficiency. Ann Neurol Off J Am Neurol Assoc Child Neurol Soc. 1988;24(6):749–56.
Pavlakis SG, Phillips PC, DiMauro S, De Vivo DC, Rowland LP. Mitochondrial myopathy, encephalopathy, lactic acidosis, and strokelike episodes: a distinctive clinical syndrome. Ann Neurol Off J Am Neurol Assoc Child Neurol Soc. 1984;16(4):481–8.
So N, Berkovic S, Andermann F, Kuzniecky R, Gendron D, Quesney LF. Myoclonus Epilepsy and Ragged-Red Fibres (Merrf). Brain. 1989;112(5):1261–76.
Hirano M, Ricci E, Koenigsberger MR, Defendini R, Pavlakis SG, DeVivo DC, et al. MELAS: an original case and clinical criteria for diagnosis. Neuromuscul Disord. 1992;2(2):125–35.
Finsterer J, Scorza F. Renal manifestations of primary mitochondrial disorders. Biomed Reports. 2017;6(5):487–94.
Brambilla A, Favilli S, Olivotto I, Calabri GB, Porcedda G, De Simone L, et al. Clinical profile and outcome of cardiac involvement in MELAS syndrome. Int J Cardiol [Internet]. 2019;276:14–9. https://doi.org/10.1016/j.ijcard.2018.10.051.
Quadir A, Pontifex CS, Lee Robertson H, Labos C, Pfeffer G. Systematic review and meta- analysis of cardiac involvement in mitochondrial myopathy. Neurol Genet. 2019;5(4):e339. https://doi.org/10.1212/NXG.0000000000000339.
DiMauro S, Hirano M, Kaufmann P, Tanji K, Sano M, Shungu DC. Clinical features and genetics of myoclonic epilepsy with ragged red fibers. Adv Neurol. 2002;89:217–29.
Catteruccia M, Sauchelli D, Della Marca G, Primiano G, Cuccagna C, Bernardo D, et al. “Myo-cardiomyopathy” is commonly associated with the A8344G “MERRF” mutation. J Neurol. 2015;262(3):701–10.
Wahbi K, Larue S, Jardel C, Meune C, Stojkovic T, Ziegler F, et al. Cardiac involvement is frequent in patients with the m.8344A>G mutation of mitochondrial DNA. Neurology. 2010;74(8):674–7.
Anan R, Nakagawa M, Miyata M, Higuchi I, Nakao S, Suehara M, et al. Cardiac involvement in mitochondrial diseases: a study on 17 patients with documented mitochondrial DNA defects. Circulation. 1995;91(4):955–61.
Lake NJ, Compton AG, Rahman S, Thorburn DR. Leigh syndrome: one disorder, more than 75 monogenic causes. Ann Neurol. 2016;79(2):190–203.
Johnson SC, Yanos ME, Kayser E-B, Quintana A, Sangesland M, Castanza A, et al. mTOR inhibition alleviates mitochondrial disease in a mouse model of Leigh syndrome. Science (80-). 2013;342(6165):1524–8.
Martin-Perez M, Grillo AS, Ito TK, Valente AS, Han J, Entwisle SW, et al. PKC downregulation upon rapamycin treatment attenuates mitochondrial disease. Nat Metab. 2020;2(12):1472–81.
Yoon J-Y, Daneshgar N, Chu Y, Chen B, Hefti M, Irani K, et al. Metabolic rescue ameliorates mitochondrial encephalo-cardiomyopathy in murine and human iPSC models of Leigh syndrome. BioRxiv. 2022;141(3):70.
Inak G, Rybak-Wolf A, Lisowski P, Pentimalli TM, Jüttner R, Glažar P, et al. Defective metabolic programming impairs early neuronal morphogenesis in neural cultures and an organoid model of Leigh syndrome. Nat Commun. 2021;12:1929. https://doi.org/10.1038/s41467-021-22117-z.
Orsucci D, Ienco EC, Rossi A, Siciliano G, Mancuso M. Mitochondrial syndromes revisited. J Clin Med. 2021;10(6):1–18.
Filosto M, Mancuso M. Mitochondrial diseases: a nosological update. Acta Neurol Scand. 2007;115(4):211–21.
Lee JS, Kim H, Lim BC, Hwang H, Choi J, Kim KJ, et al. Leigh syndrome in childhood: Neurologic progression and functional outcome. J Clin Neurol. 2016;12(2):181–7.
Sofou K, De Coo IFM, Ostergaard E, Isohanni P, Naess K, De Meirleir L, et al. Phenotype-genotype correlations in leigh syndrome: new insights from a multicentre study of 96 patients. J Med Genet. 2018;55(1):21–7.
Sadun AA, La MC, Carelli V. Leber’s hereditary optic neuropathy. Curr Treat Options Neurol. 2011;13(1):109–17.
Carelli V, Ross-Cisneros FN, Sadun AA. Mitochondrial dysfunction as a cause of optic neuropathies. Prog Retin Eye Res. 2004;23(1):53–89.
Fraser JA, Biousse V, Newman NJ. The neuro-ophthalmology of mitochondrial disease. Surv Ophthalmol. 2010;55(4):299–34. https://doi.org/10.1016/j.survophthal.2009.10.002. Epub 2010 May 14.
Sadun AA, Carelli V, Salomao SR, Berezovsky A, Quiros P, Sadun F, et al. A very large Brazilian pedigree with 11778 Leber’s hereditary optic neuropathy. Trans Am Ophthalmol Soc. 2002;100:169–79.
Sadun AA, Carelli V, Salomao SR, Berezovsky A, Quiros PA, Sadun F, et al. Extensive investigation of a large Brazilian pedigree of 11778/haplogroup J Leber hereditary optic neuropathy. Am J Ophthalmol. 2003;136(2):231–8.
Orssaud C. Cardiac disorders in patients with Leber hereditary optic neuropathy. J Neuro-Ophthalmol. 2018;38(4):466–9.
Sorajja P, Sweeney MG, Chalmers R, Sachdev B, Syrris P, Hanna M, et al. Cardiac abnormalities in patients with Leber’s hereditary optic neuropathy. Heart. 2003;89(7):791–2.
Khambatta S, Nguyen DL, Beckman TJ, Wittich CM. Kearns-Sayre syndrome: a case series of 35 adults and children. Int J Gen Med. 2014;7:325–32.
Kabunga P, Lau AK, Phan K, Puranik R, Liang C, Davis RL, et al. Systematic review of cardiac electrical disease in Kearns-Sayre syndrome and mitochondrial cytopathy. Int J Cardiol [Internet]. 2015;181:303–10. https://doi.org/10.1016/j.ijcard.2014.12.038.
Channer KS, Channer JL, Campbell MJ, Rees JR. Cardiomyopathy in the Kearns-Sayre syndrome. Br Heart J. 1988;59(4):486–90. https://doi.org/10.1136/hrt.59.4.486.
Wang J, Wilhelmsson H, Graff C, Li H, Oldfors A, Rustin P, et al. Dilated cardiomyopathy and atrioventricular conduction blocks induced by heart-specific inactivation of mitochondrial DNA gene expression. Nat Genet. 1999;21(1):133–7.
Sehgal S, Choudhry S, Debelenko L, L’Ecuyer T. Dilated cardiomyopathy with cardiogenic shock in a child with Kearns-Sayre syndrome. BMJ Case Rep. 2016;2016:2–5.
Gasanoff ES, Yaguzhinsky LS, Garab G. Cardiolipin, non-bilayer structures and mitochondrial bioenergetics: Relevance to cardiovascular disease. Cells. 2021;10(7):1–24.
Chatfield KC, Sparagna GC, Sucharov CC, Miyamoto SD, Grudis JE, Sobus RD, et al. Dysregulation of cardiolipin biosynthesis in pediatric heart failure. J Mol Cell Cardiol. 2014;74:251–9.
Saini-Chohan HK, Holmes MG, Chicco AJ, Taylor WA, Moore RL, McCune SA, et al. Cardiolipin biosynthesis and remodeling enzymes are altered during development of heart failure. J Lipid Res. 2009;50(8):1600–8.
Schlame M, Shanske S, Doty S, König T, Sculco T, DiMauro S, et al. Microanalysis of cardiolipin in small biopsies including skeletal muscle from patients with mitochondrial disease. J Lipid Res. 1999;40(9):1585–92.
Bertero E, Kutschka I, Maack C, Dudek J. Cardiolipin remodeling in Barth syndrome and other hereditary cardiomyopathies. Biochim Biophys Acta - Mol Basis Dis [Internet]. 2020;1866(8):165803. https://doi.org/10.1016/j.bbadis.2020.165803.
Bione S, D’Adamo P, Maestrini E, Gedeon AK, Bolhuis PA, Toniolo D. A novel X-linked gene, G4. 5. is responsible for Barth syndrome. Nat Genet. 1996;12(4):385–9.
Houtkooper RH, Turkenburg M, Poll-The BT, Karall D, Perez-Cerdá C, Morrone A, et al. The enigmatic role of tafazzin in cardiolipin metabolism. Biochim Biophys Acta Biomembranes. 2009;1788(10):2003–14.
Xu Y, Phoon CKL, Berno B, D’Souza K, Hoedt E, Zhang G, et al. Loss of protein association causes cardiolipin degradation in Barth syndrome. Nat Chem Biol. 2016;12(8):641–7.
Barth PG, Scholte HR, Berden JA, der Klei-Van Moorsel JM, Luyt-Houwen IEM, Veer-Korthof ETV, et al. An X-linked mitochondrial disease affecting cardiac muscle, skeletal muscle and neutrophil leucocytes. J Neurol Sci. 1983;62(1–3):327–55.
Spencer CT, Bryant RM, Day J, Gonzalez IL, Colan SD, Thompson WR, et al. Cardiac and clinical phenotype in Barth syndrome. Pediatrics. 2006;118(2):e337–46.
Chowdhury S, Jackson L, Byrne BJ, Bryant RM, Cade WT, Churchill TL, et al. Longitudinal observational study of cardiac outcome risk factor prediction in children, adolescents, and adults with Barth syndrome. Pediatr Cardiol. 2022;43:1–13.
Spencer CT, Byrne BJ, Bryant RM, Margossian R, Maisenbacher M, Breitenger P, et al. Impaired cardiac reserve and severely diminished skeletal muscle O2 utilization mediate exercise intolerance in Barth syndrome. Am J Physiol Circ Physiol. 2011;301(5):H2122–9.
Wang S, Li Y, Xu Y, Ma Q, Lin Z, Schlame M, et al. AAV gene therapy prevents and reverses heart failure in a murine knockout model of Barth syndrome. Circ Res. 2020;126(8):1024–39.
Bertero E, Nickel A, Kohlhaas M, Hohl M, Sequeira V, Brune C, et al. Loss of mitochondrial Ca2+ uniporter limits inotropic reserve and provides trigger and substrate for arrhythmias in Barth syndrome cardiomyopathy. Circulation. 2021;144(21):1694–713.
Brandes R, Bers DM. Intracellular Ca2+ increases the mitochondrial NADH concentration during elevated work in intact cardiac muscle. Circ Res. 1997;80(1):82–7.
Spencer CT, Byrne BJ, Gewitz MH, Wechsler SB, Kao AC, Gerstenfeld EP, et al. Ventricular arrhythmia in the X-linked cardiomyopathy Barth syndrome. Pediatr Cardiol. 2005;26(5):632–7.
Liu X, Wang S, Guo X, Li Y, Ogurlu R, Lu F, et al. Increased reactive oxygen species–mediated Ca2+/calmodulin-dependent protein kinase II activation contributes to calcium handling abnormalities and impaired contraction in Barth syndrome. Circulation. 2021;143(19):1894–911.
Petit PX, Ardilla-Osorio H, Penalvia L, Rainey NE. Tafazzin mutation affecting cardiolipin leads to increased mitochondrial superoxide anions and mitophagy inhibition in Barth syndrome. Cells. 2020;9(10):2333.
Wang G, McCain ML, Yang L, He A, Pasqualini FS, Agarwal A, et al. Modeling the mitochondrial cardiomyopathy of Barth syndrome with induced pluripotent stem cell and heart-on-chip technologies. Nat Med. 2014;20(6):616–23.
Johnson JM, Ferrara PJ, Verkerke ARP, Coleman CB, Wentzler EJ, Neufer PD, et al. Targeted overexpression of catalase to mitochondria does not prevent cardioskeletal myopathy in Barth syndrome. J Mol Cell Cardiol. 2018;121:94–102.
Thompson WR, Hornby B, Manuel R, Bradley E, Laux J, Carr J, et al. A phase 2/3 randomized clinical trial followed by an open-label extension to evaluate the effectiveness of elamipretide in Barth syndrome, a genetic disorder of mitochondrial cardiolipin metabolism. Genet Med. 2021;23(3):471–8.
Mayr JA, Haack TB, Graf E, Zimmermann FA, Wieland T, Haberberger B, et al. Lack of the mitochondrial protein acylglycerol kinase causes sengers syndrome. Am J Hum Genet [Internet]. 2012;90(2):314–20. https://doi.org/10.1016/j.ajhg.2011.12.005.
Chu B, Hong Z, Zheng X. Acylglycerol kinase-targeted therapies in oncology. Front Cell Dev Biol. 2021;9(July):1–12.
Jiang H, Yu Z, Ding N, Yang M, Zhang L, Fan X, et al. The role of AGK in thrombocytopoiesis and possible therapeutic strategies. Blood [Internet]. 2020;136(1):119–29. https://doi.org/10.1182/blood.2019003851.
Haghighi A, Haack TB, Atiq M, Mottaghi H, Haghighi-Kakhki H, Bashir RA, et al. Sengers syndrome: six novel AGK mutations in seven new families and review of the phenotypic and mutational spectrum of 29 patients. Orphanet J Rare Dis. 2014;9:119. https://doi.org/10.1186/s13023-014-0119-3.
van Ekeren GJ, Stadhouders AM, Smeitink JAM, Sengers RCA. A retrospective study of patients with the hereditary syndrome of congenital cataract, mitochondrial myopathy of heart and skeletal muscle and lactic acidosis. Eur J Pediatr. 1993;152(3):255–9.
Morava E, Sengers R, Ter Laak H, Van Den Heuvel L, Janssen A, Trijbels F, et al. Congenital hypertrophic cardiomyopathy, cataract, mitochondrial myopathy and defective oxidative phosphorylation in two siblings with Sengers-like syndrome. Eur J Pediatr. 2004;163(8):467–71.
Ojala T, Polinati P, Manninen T, Hiippala A, Rajantie J, Karikoski R, et al. New mutation of mitochondrial DNAJC19 causing dilated and noncompaction cardiomyopathy, anemia, ataxia, and male genital anomalies. Pediatr Res. 2012;72(4):432–7.
Al Tuwaijri A, Alyafee Y, Alharbi M, Ballow M, Aldrees M, Alam Q, et al. Novel homozygous pathogenic mitochondrial DNAJC19 variant in a patient with dilated cardiomyopathy and global developmental delay. Mol Genet Genomic Med. 2022;10(8):e1969. https://doi.org/10.1002/mgg3.1969. Epub 2022 May 25.
Davey KM, Parboosingh JS, McLeod DR, Chan A, Casey R, Ferreira P, et al. Mutation of DNAJC19, a human homologue of yeast inner mitochondrial membrane co-chaperones, causes DCMA syndrome, a novel autosomal recessive Barth syndrome-like condition. J Med Genet. 2006;43(5):385–93.
Janz A, Chen R, Regensburger M, Ueda Y, Rost S, Klopocki E, et al. Generation of two patient-derived iPSC lines from siblings (LIBUCi001-A and LIBUCi002-A) and a genetically modified iPSC line (JMUi001-A-1) to mimic dilated cardiomyopathy with ataxia (DCMA) caused by a homozygous DNAJC19 mutation. Stem Cell Res. 2020;46:101856. https://doi.org/10.1016/j.scr.2020.101856.
Jackson TD, Hock DH, Fujihara KM, Palmer CS, Frazier AE, Low YC, et al. The TIM22 complex mediates the import of sideroflexins and is required for efficient mitochondrial one-carbon metabolism. Mol Biol Cell. 2021;32(6):475–91.
Sinha D, Srivastava S, D’Silva P. Functional diversity of human mitochondrial J-proteins is independent of their association with the inner membrane presequence translocase. J Biol Chem. 2016;291(33):17345–59.
Richter-Dennerlein R, Korwitz A, Haag M, Tatsuta T, Dargazanli S, Baker M, et al. DNAJC19, a mitochondrial cochaperone associated with cardiomyopathy, forms a complex with prohibitins to regulate cardiolipin remodeling. Cell Metab [Internet]. 2014;20(1):158–71. https://doi.org/10.1016/j.cmet.2014.04.016.
Machiraju P, Degtiarev V, Patel D, Hazari H, Lowry RB, Bedard T, et al. Phenotype and pathology of the dilated cardiomyopathy with ataxia syndrome in children. J Inherit Metab Dis. 2022;45(2):366–76.
Benson MD, Ferreira P, MacDonald IM. Oculomotor apraxia and dilated cardiomyopathy with ataxia syndrome: a case report. Ophthalmic Genet. 2017;38(1):88–90.
Sparkes R, Patton D, Bernier F. Cardiac features of a novel autosomal recessive dilated cardiomyopathic syndrome due to defective importation of mitochondrial protein. Cardiol Young. 2007;17(2):215–7.
Kalkhoran S, Benowitz NL, Rigotti NA. Reprint of: Prevention and Treatment of Tobacco Use: JACC Health Promotion Series. J Am Coll Cardiol. 2018;72(23):2964–79. https://doi.org/10.1016/j.jacc.2018.10.020.
Rubio-Gozalbo ME, Bakker JA, Waterham HR, Wanders RJA. Carnitine-acylcarnitine translocase deficiency, clinical, biochemical and genetic aspects. Mol Aspects Med. 2004;25(5–6):521–32.
Jeukendrup AE, Saris WHM, Wagenmakers M. Fat metabolism during exercise: a review — part II: regulation of metabolism and the effects of training. Int J Sports Med. 1998;19:293–302.
Rinaldo P, Matern D, Bennett MJ. Fatty acid oxidation disorders. Annu Rev Physiol. 2002;64(1):477–502.
Byers SL. Infant with cardiomyopathy: when to suspect inborn errors of metabolism? World J Cardiol. 2014;6(11):1149.
Ranea-Robles P, Pavlova NN, Bender A, Pereyra AS, Ellis JM, Stauffer B, et al. A mitochondrial long-chain fatty acid oxidation defect leads to transfer RNA uncharging and activation of the integrated stress response in the mouse heart. Cardiovasc Res. 2022;267(2):36.
El-Gharbawy A, Vockley J. Inborn errors of metabolism with myopathy: defects of fatty acid oxidation and the carnitine shuttle system. Pediatr Clin North Am. 2018;65(2):317–35.
Das AM, Steuerwald U, Illsinger S. Inborn errors of energy metabolism associated with myopathies. J Biomed Biotechnol. 2010;2010:340849. https://doi.org/10.1155/2010/340849. Epub 2010 May 26.
Smith EC, El-gharbawy A, Koeberl DD. Metabolic myopathies: clinical features and diagnostic approach. Rheum Dis Clin North Am. 2011;37:201–17.
Koeppen AH, Becker AB, Qian J, Feustel PJ. Friedreich ataxia: hypoplasia of spinal cord and dorsal root ganglia. J Neuropathol Exp Neurol. 2017;76(2):101–8.
Delatycki MB, Bidichandani SI. Friedreich ataxia- pathogenesis and implications for therapies. Neurobiol Dis [Internet]. 2019;132(June):104606. https://doi.org/10.1016/j.nbd.2019.104606.
Reetz K, Dogan I, Costa AS, Dafotakis M, Fedosov K, Giunti P, et al. Biological and clinical characteristics of the European Friedreich's Ataxia Consortium for Translational Studies (EFACTS) cohort: a cross-sectional analysis of baseline data. Lancet Neurol. 2015;14(2):174–82. https://doi.org/10.1016/S1474-4422(14)70321-7.
Pandey A, Gordon DM, Pain J, Stemmler TL, Dancis A, Pain D. Desulfurase by exposing substrate-binding sites, and a mutant Fe-S cluster scaffold protein with frataxin-bypassing ability acts similarly. J Biol Chem. 2013;288(52):36773–86.
Gakh O, Park S, Liu G, Macomber L, Imlay JA, Ferreira GC, et al. Mitochondrial iron detoxification is a primary function of frataxin that limits oxidative damage and preserves cell longevity. Hum Mol Genet. 2006;15(3):467–79.
Shan Y, Schoenfeld RA, Hayashi G, Napoli E, Akiyama T, Iodi Carstens M, et al. Frataxin deficiency leads to defects in expression of antioxidants and Nrf2 expression in dorsal root ganglia of the Friedreich’s ataxia YG8R mouse model. Antioxidants Redox Signal. 2013;19(13):1481–93.
Abeti R, Parkinson MH, Hargreaves IP, Angelova PR, Sandi C, Pook MA, et al. Mitochondrial energy imbalance and lipid peroxidation cause cell death in friedreich’s ataxia. Cell Death Dis. 2016;7(5):1–11.
Jiang X, Stockwell BR, Conrad M. Ferroptosis: mechanisms, biology and role in disease. Nat Rev Mol Cell Biol. 2021;22(4):266–82.
Cotticelli MG, Xia S, Lin D, Lee T, Terrab L, Wipf P, et al. Ferroptosis as a novel therapeutic target for Friedreich’s ataxia. J Pharmacol Exp Ther. 2019;369(1):47–54.
Tsou AY, Paulsen EK, Lagedrost SJ, Perlman SL, Mathews KD, Wilmot GR, et al. Mortality in Friedreich Ataxia. J Neurol Sci [Internet]. 2011;307(1–2):46–9. https://doi.org/10.1016/j.jns.2011.05.023.
Cook A, Giunti P. Friedreich’s ataxia: clinical features, pathogenesis and management. Br Med Bull. 2017;124(1):19–30.
Weidemann F, Rummey C, Bijnens B, Störk S, Jasaityte R, Dhooge J, et al. Mitochondrial Protection with Idebenone in Cardiac or Neurological Outcome (MICONOS) study group. The heart in Friedreich ataxia: definition of cardiomyopathy, disease severity, and correlation with neurological symptoms. Circulation. 2012;125(13):1626–34. https://doi.org/10.1161/CIRCULATIONAHA.111.059477. Epub 2012 Feb 29.
Liu D, Hu K, Herrmann S, Weidemann F, St S, Ertl G, et al. Cardiomyopathy Friedreich Ataxia. 2013;126:88–93.
Pousset F, Legrand L, Monin ML, Ewenczyk C, Charles P, Komajda M, et al. A 22-year follow-up study of long-term cardiac outcome and predictors of survival in Friedreich ataxia. JAMA Neurol. 2015;72(11):1334–41.
Regner SR, Lagedrost SJ, Plappert T, Paulsen EK, Friedman LS, Snyder ML, et al. Analysis of echocardiograms in a large heterogeneous cohort of patients with Friedreich ataxia. Am J Cardiol [Internet]. 2012;109(3):401–5. https://doi.org/10.1016/j.amjcard.2011.09.025.
Martinez ARM, Moro A, Abrahao A, Faber I, Borges CR, Rezende TJR, et al. Nonneurological involvement in late-onset Friedreich ataxia (LOFA): exploring the phenotypes. Cerebellum. 2017;16(1):253–6.
Anheim M, Mariani LL, Calvas P, Cheuret E, Zagnoli F, Odent S, et al. Exonic deletions of FXN and early-onset Friedreich ataxia. Arch Neurol. 2012;69(7):912–6.
Fsadni MG, Klopstock T, Metz G, Yu-wai-man P, Büchner B, Gallemüller C, et al. Persistence of treatment effect of idebenone in Leber’s hereditary optic neuropathy. Acta Ophthalmol. 2012. 90:249. https://doi.org/10.1111/j.1755-3768.2012.T132.x.
Bacman SR, Kauppila JHK, Pereira CV, Nissanka N, Miranda M, Pinto M, et al. MitoTALEN reduces mutant mtDNA load and restores tRNAAla levels in a mouse model of heteroplasmic mtDNA mutation. Nat Med. 2018;24(11):1696–700.
Gammage PA, Viscomi C, Simard M-L, Costa ASH, Gaude E, Powell CA, et al. Genome editing in mitochondria corrects a pathogenic mtDNA mutation in vivo. Nat Med. 2018;24(11):1691–5.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
There are no studies by any of the writers in this article that used human or animal subjects.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The editors would like to thank Dr. Christiane Angermann for taking the time to handle the review of this manuscript.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Popoiu, TA., Dudek, J., Maack, C. et al. Cardiac Involvement in Mitochondrial Disorders. Curr Heart Fail Rep 20, 76–87 (2023). https://doi.org/10.1007/s11897-023-00592-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11897-023-00592-3