
Abstract
Context
Diabetes is a leading metabolic disorder with a substantial cost burden, especially in inpatient settings. The complexity of inpatient glycemic management has led to the emergence of inpatient diabetes management service (IDMS), a multidisciplinary team approach to glycemic management.
Objective
To review recent literature on the financial and clinical impact of IDMS in hospital settings.
Methods
We searched PubMed using a combination of controlled vocabulary and keyword terms to describe the concept of IDMS and combined the search terms with a comparative effectiveness filter for costs and cost analysis developed by the National Library of Medicine.
Findings
In addition to several improved clinical endpoints such as glycemic management outcomes, IDMS implementation is associated with hospital cost savings through decreased length of stay, preventing hospital readmissions, hypoglycemia reduction, and optimizing resource allocation. There are other downstream potential cost savings in long-term patient health outcomes and avoidance of litigation related to suboptimal glycemic management.
Conclusion
IDMS may play an important role in helping both academic and community hospitals to improve the quality of diabetes care and reduce costs. Clinicians and policymakers can utilize existing literature to build a compelling business case for IDMS to hospital administrations and state legislatures in the era of value-based healthcare.
Similar content being viewed by others

Introduction
Diabetes mellitus is a leading metabolic disorder that affects at least 34.2 million individuals in the USA as of 2018 [1]. People living with diabetes are three times more likely to be hospitalized than individuals without a chronic condition [2]. The annual cost of diabetes mellitus in the USA is $327 billion, $97 billion of which was spent in the inpatient setting [3]. The per capita healthcare expenditures for hospital care in 2017 was estimated to be $4966 for patients with diabetes and $1202 for individuals without diabetes. The largest cost contributors to diabetes care are inpatient hospital care (30% of total cost) and prescription medications for chronic complications of diabetes (30%) [3].
Patients with diabetes often experience fluctuating glucose levels during hospitalization due to the stress of acute illness, decreased level of activity, and possibly hospital diet [4]. It has been estimated that one-third of all patients and 46% of those in the intensive care unit (ICU) experience hyperglycemia at some point in their hospital stay [5]. Patients who experience hyperglycemia during their hospital course and are discharged with one of the six diagnoses under the Centers for Medicare and Medicaid Hospital Readmissions Reduction Program may have a higher 30-day readmission rate (30DR) [6]. Similarly, hypoglycemia adversely impacts drivers of hospital cost. In a study of nearly 44,000 hospitalizations in 2015–2016 within the Florida Health System, it was found that patients experiencing normoglycemia had an average length of stay (LOS) of 7.8 days and $11,039 average cost of stay compared to those experiencing severe hypoglycemia, who had an average LOS of 14.4 days and $21,444 average cost per stay [7].
While a growing stream of research supports the call for health systems to readily address a patient’s inpatient glycemic status from the standpoint of outcomes and cost [8], some care teams (e.g., hospitalists) may not be in a position to optimize glycemia for all patients. Authors speculate the main reason is that most hospitalized patients with diabetes are admitted with a different (non-diabetes) primary diagnosis. As such, managing the patient’s glycemia may not be a priority for some healthcare providers [9].
Patients living with diabetes tend to have a complex outpatient medication regimen, consisting of multiple oral and/or injectable diabetes medications. The American Diabetes Association recommends that all oral anti-diabetes medications be withheld upon hospitalization and for insulin to be used as the main therapy for glycemic management [10]. However, due to the fragmented healthcare system in the USA, inpatient providers may be hesitant to significantly alter a patient’s outpatient diabetes regimen upon admission [8]. Moreover, providers are often reticent to adjust insulin doses during a hospitalization stay, even in the face of persistent hyper- or hypoglycemia [11]. We speculate that inpatient providers may experience therapeutic inertia with diabetes care since they may not be as knowledgeable and/or comfortable with glycemic management, especially initiating and intensifying insulin therapy in the setting of acute illness, high-dose steroid treatment, and enteral feedings. Without coordinated inpatient care for diabetes patients, there may be difficulty in optimizing the diabetes medication regimen for the transition back to the outpatient setting, educating patients and their family members on managing personal health, and instituting consistent protocols for blood glucose monitoring [12].
Inpatient Diabetes Management Service Team Model
To improve inpatient glycemic management, many hospitals have instituted an inpatient diabetes management service (IDMS) team, which takes an interdisciplinary, interprofessional approach to diabetes patient care. While variations of the IDMS exist across institutions, the team is generally physician-led and consists of an endocrinologist, diabetes nurse practitioner or physician assistant, diabetes care and education specialist (formerly, diabetes educator), pharmacist, dietitian, registered nurses, and discharge/transition coordinators [13, 14]. Other ad hoc members may play additional roles (Fig. 1).

Simplified structure of inpatient diabetes management service
Clinical Benefits of IDMS
The IDMS model has gained significant popularity in the USA because it has been shown to improve clinical outcomes. Institution of IDMS is associated with reduced rates of both hypo- and hyperglycemia [15, 16]. Koproski et al., for example, found that 75% of patients under the care of an IDMS vs 46% in the control group achieved target glycemic management [17], while another study found that the mean inpatient blood glucose level among IDMS-treated patients was on average 17 mg/dL lower than in the “usual care” control group [18]. “Virtual” IDMS, where diabetes specialists view patient glucose values remotely and enter recommendations into the electronic health record, has also been shown to reduce hypo- and hyperglycemia as well as glycemic variability [19, 20].
Of note, inpatient glycemic outcomes are particularly important in cardiac and surgical patients, as poor management has been associated with increased complications and mortality [21,22,23]. In addition to classic IDMS team models [24], both pharmacist and nurse practitioner-led teams have demonstrated significant improvements in glycemic outcomes in patients undergoing cardiac surgery [25,26,27]. Improvements in inpatient glycemia due to IDMS intervention have been associated with reductions in infections [15, 25] and a non-significant trend towards decreased in-hospital mortality [28].
The financial impact of IDMS has been previously studied. While improved patient management may decrease cost in a multitude of ways, there are four broad, interrelated categories of cost savings through IDMS: decreased LOS, reduced number of readmissions, improved resource allocation, and improved long-term health. Table 1 displays clinical outcomes relevant to costs with associated cost savings in previous research. The purpose of this review is to provide an updated view of the clinical literature on how IDMS impacts patient outcomes and healthcare spending, followed by a discussion of limitations in measuring the financial impact of IDMS and potential future research opportunities.
Methods
The authors searched PubMed (MEDLINE database) using a combination of controlled vocabulary and keyword terms to describe the concept of inpatient diabetes management teams and combined them with a comparative effectiveness filter on the PubMed website for costs and cost analysis developed by the National Library of Medicine. The search term was: “inpatient diabetes care” OR “inpatient diabetes team” OR “inpatient diabetes teams” OR “inpatient diabetes management teams” OR “inpatient diabetes management team” AND (cost[tw] OR costs[tw] OR costs and cost analysis[mh] OR ec[sh]).
Financial Benefits of IDMS
Length of Stay
IDMS plays a pivotal role in cost savings through decreased patient LOS. Patients with diabetes can account for up to a quarter of occupied beds in an acute hospital at any given moment [13]. Adigopula et al. found that persistent hyperglycemia in patients admitted for congestive heart failure had longer stays (8.1 days compared to 5.2 days for patients without hyperglycemia) and a median total hospital bill of $8940 compared to $6892 for other patients in the study [33]; 46% of these patients with a prolonged hospital stay (greater than 7 days) had a total cost of at least $10,000. On the other end of the glucose spectrum, each additional recorded day with hypoglycemia is associated with an additional 2.5 day LOS for patients with diabetes on general wards [34].
The earliest study attempting to assess the impact of a multidisciplinary diabetes team on LOS was from 1995 and compared the hospital stays of consecutive patients with diabetes (43 received an individual endocrinologist consult, 27 were seen by an internist alone, and 34 were also managed by the diabetes team) [30]. The average LOS for patients seen by the diabetes team was 3.6 days, which was 35% shorter than patients receiving the traditional endocrine consult (5.5 days) and 56% shorter than those without a consultation (8.2 days).
In a more recent study, implementing an inpatient team consisting of five diabetes specialty nurses with the support of a diabetologist was associated with a decreased average LOS from 8.3 to 7.7 days. Interestingly, a significant reduction was found for medical admissions, but not for surgical admissions [31]. Several other studies of IDMS have found a significant reduction in LOS. Levetan et al. found that while both the single endocrinologist and multidisciplinary IDMS models reduced LOS as compared to routine care, the team model also significantly outperformed the solo endocrinology consultant model [30]. It was also shown that the earlier the IDMS consultation was placed during the hospitalization, the shorter the LOS [30]. A study of patients receiving coronary artery bypass surgery uncovered an association between each 50 mg/dL increase in serum glucose, an additional 0.76 day LOS and $1769 hospitalization cost [35]. Additionally, LOS was shorter (4.7 days compared to 6.1 days) when the patient received an IDMS consultation on the first day of admission versus later in the hospitalization in a cost-effectiveness study of IDMS versus a primary service team [28]. Lastly, a retrospective quality improvement study at the author’s institution (Suburban Hospital, a community hospital in the Johns Hopkins Health System) found that patients co-managed by IDMS had 27% lower average LOS associated with a cost-saving of $953,578 during the study period [13, 14].
A possible decreased LOS in a pediatric type 1 diabetes population has also been noted. The implementation of an Inpatient Diabetes Care Process Team at one pediatric hospital consisting of both physicians and nurses of multiple specialties along with pharmacists led to 94% of patients with diabetic ketoacidosis (DKA) being assigned to a specialized diabetes care unit with a subsequent 44% decrease in LOS (3.8 to 2.1 days) [36]. The shorter stay was attributed to quicker recognition of diabetes ketoacidosis with decreasing variation in care, implementing evidence-supported order sets, and mitigating care inefficiencies.
Hospital Readmissions
Implementing an IDMS also has the potential to reduce costs and financial penalties stemming from excess readmission rates of patients living with diabetes. A retrospective cohort study of adult patients with diabetes found that blood glucose on admission was not a significant predictor of cost, but that there was a $43 increase in healthcare cost associated with each 10 mg/dL increase in blood glucose upon hospital discharge [37]. Additionally, patients who experience persistent hyperglycemia throughout their hospitalization are more likely to be readmitted within six months of discharge than patients whose average blood glucose remained below 140 mg/dL (51% vs 37%) [33]. A study of over one million hospital admissions found that individuals with diabetes who have high glucose variability on the last day of their hospital stay are at increased risk for 30DR [38].
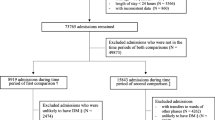
Effects of an IDMS on readmission rates have been mixed. Several studies have demonstrated reductions in readmission rates between 10 and 17% [13, 17, 28], while other studies found no effect [18, 34, 39]. For example, Ostling et al., found that IDMS reduced 30-day repeat visits to the emergency department or readmission to observation status, but had no effect on inpatient readmission rate [40]. However, Mandel and colleagues found that patients co-managed by the IDMS team had a mean 30DR that decreased over time from 25% to 14.29%, and these patients had a lower median 30D than patients not co-managed by the IDMS team [13, 14]. In another study, hospitalized patients with diabetes were randomly assigned either to usual care (94 patients) or supplemented with the diabetes team (85 patients), consisting of an endocrinologist and diabetes specialty nurse. They observed a 15% 3-month readmission rate for patients receiving IDMS as compared to 32% for the control group [29]. The difference in readmission rate persisted at 6 months, even though both groups were similar in terms of co-morbidities and expected LOS during initial hospital admission.
Another cost-effectiveness study of IDMS versus a primary service team retrospectively evaluated 392 patients for readmission rate and frequency, length of stay, and hospital costs [28]. Despite the IDMS team facing a significantly higher rate of patients with in-hospital complications and increased diabetes complexity, the 30-day readmission rate to medical services for patients receiving IDMS care was 30.5% lower than without supplemental care. It should be noted that the 30DR to surgical services was 5% higher in the IDMS group relative to the primary service team group. Authors speculated that higher 30DR may be attributed to the surgical team being “slightly more inclined to consider late consultations” to the IDMS team. Additionally, surgical units used routine discharge process, while medical units utilized a comprehensive discharge pathway based on risk category.
Hypoglycemia Reduction Cost Savings
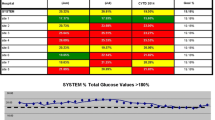
A cost analysis performed in Italy estimates that a 20% reduction in the rates of hypoglycemia can lead to savings of €47,769 per 100,000 individuals [41]. There is mixed evidence on the implementation of glucose management programs and a corresponding reduction in severe or non-severe hypoglycemia. A multidisciplinary glycemic management team implemented at the Johns Hopkins Hospital led to a 19% reduction in the frequency of hypoglycemia among adults in the non-ICU setting between 2006 and 2009 [42]. On the other hand, implementing the IDMS program in another hospital resulted in a reduction of the monthly average glucose value in the ICU setting from a mean of 169.4 to 123.5 mg/dL with a marginal change (decrease of 0.01%) in the prevalence of severe hypoglycemia (<40 mg/dL) despite 7.98% of glucose readings showing hypoglycemia (<70 mg/dL) [15]. The difficulty in interpreting the impact of the program in this regard may be attributed to the types of patients assigned to the IDMS. For example, another intervention study notes that increased hypoglycemia and hyperglycemia frequency in the IDMS group was unsurprising because “[their] patients tend to be younger, usually on insulin pumps, treated with complex insulin regimens and [had] higher blood glucose variability” [28].
Legal Costs Associated with Litigation Due to Hypoglycemia
Suboptimal glycemic management leading to a severe outcome or diabetes-related complication such as hypoglycemia can be a source of medical litigation against the hospital or individual physicians. For example, a 42-year old female with a known history of severe hypoglycemic episodes suffered a hypoglycemia event that led to a coma and permanent brain damage in 2004 [43]. Notably, the notation on the patient’s chart regarding her hypoglycemia after taking a beta-blocker previously said, “Thanks. We’re watching closely.” This legal case was settled for $4 million. An even larger payout occurred in an unfortunate case of a 59-year-old woman who died after being discharged with an insulin prescription order that was mistakenly written for eighty insulin units instead of eight [44]. The jury awarded the victim’s family $140 million. We speculate that IDMS expertise may help prevent/reduce severe glycemic events and diabetes-related complications, and therefore prevent litigation, leading to further cost savings. Other strategies include prescriber and nurse education around safe insulin dosing and administration, computerized insulin dosing systems and structured insulin order sets in the electronic health record.
Resource Allocation during a Hospital Stay
Patients living with diabetes with suboptimal glycemic management are at increased risk of delayed wound healing, neurological ischemia, infection, and poorer outcomes related to the reason for admission [45]. It is thus expected that a reduced LOS has a multiplier cost savings effect by also obviating the additional resources a patient with diabetes may require for a new complication arising during a prolonged hospital stay. The fewer the complications that arise, the fewer additional procedures and subspecialty consultations will be required for the patient. For example, the longer a patient remains on a ventilator, the greater the risk of acquiring an infection.
A study of the National Hospital Discharge Survey from 2004 of 370,785 inpatient records found that the hospital cost of uncontrolled diabetes without complications was $552 million ($52,294 per admission), but this skyrocketed to $1821 billion ($124,510 per admission) for patients with a diagnosis of uncontrolled diabetes with ketoacidosis [46]. Additionally, there was an increased cost for other complications such as hyperosmolarity ($14,572) and diabetic coma ($4948) per hospitalization.
The IDMS initiative has not only been shown to decrease the resources allocated to multi-morbid diabetes patients but to also improve more appropriate use of resources. In Texas Children’s Hospital, implementing a program led to a relative 17% increase in patients receiving an evidence-based diabetes evaluation [36]. There was also a 19% increase in these patients receiving intravenous insulin within 1 h of the order being placed and a 50% increase in transitioning to subcutaneous insulin within 4 h of being indicated.
Long-Term Cost Savings
Keeping appointments and following the recommended therapy after a hospital admission presents another area of financial benefit as a result of IDMS implementation. One study found that patients seen by the IDMS team were more likely to keep up with post-discharge primary-care/surgery appointments (87.8% versus 69.5% for the primary services team) and/or endocrinology appointments (32.8% vs. 2.3% for the primary services team) [28]. Patients participating in a pediatric diabetes case management program were able to have more telephone contact with the educator (or endocrinologist if needed) and kept up more with follow-up appointments than nonparticipants, yielding $1350 in savings per patient based on averted future hospitalizations and emergency department visits [47].
While more research is needed to measure the long-term cost savings from IDMS once a patient is discharged, improvements in the transition of care can have a profound effect. Decreasing the number of diabetes-related complications over time that require hospitalization such as stroke, ischemic heart disease, amputation/ulceration, and end-stage renal disease would lead to further reductions in cost and resource utilization [48].
Challenges of IDMS-Related Research
As described above, the current body of evidence suggests that the implementation of multi-disciplinary IDMS teams is associated with reductions in the main drivers of cost of hospitalization: LOS and 30DR. However, these studies frequently suffer from limitations in their methodology. For example, studies of 30DR often describe discharge and readmission to a single hospital. However, patients may be readmitted to a different hospital than the one from which they are discharged. Depending on the payor model for a particular state or health system, this cost of re-hospitalization may not be properly accounted for in single-hospital studies.
Next, few studies are prospective and such studies have small numbers of subjects making generalization of results challenging. Most studies of LOS and 30DR are retrospective. Consequently, such studies may be biased, since IDMS consultations are likely to be requested for more complex patients. Therefore, comparing LOS and 30DR for patients in whom IDMS was co-managing patients as compared to those in which IDMS was not involved is difficult to do unless a proper control group is chosen. Also, some studies focus on a particular patient populations (e.g., post-cardiac surgery or critically ill patients), limiting the generalizability of results.
While major medical societies have suggested glycemic targets for inpatient glycemic management, there are no national benchmarks for targets to which hospital systems are held accountable. This situation makes it less likely for hospitals to invest in glucose management programs as compared to programs that directly impact reportable conditions. From a research perspective, studies often describe different thresholds at which interventions occur and different thresholds for determining LOS and 30DR. Standardization of glycemic targets would allow studies to be compared and increase the generalizability of results.
Finally, the modeling cost of hospitalization is not uniform across different studies and it may be difficult to estimate or compare certain costs (e.g., intravenous insulin treatment, catheter-associated line infections, or antibiotic treatments). In a similar vein, the payor model is different across health systems. For example, making cost estimates in a nationalized health system is different from those in a fee-for-service model.
As a result of the above challenges, readers are advised to integrate a variety of studies and arrive at an educated determination for their particular patient population and health system.
Approaching Cost-Benefit Analyses of IDMS
It is important to garner the attention of stakeholders in “building a business case” for IDMS [14]. Given the start-up costs that a hospital may need in initiating an IDMS program, a long-term explanation of the program’s benefits and cost savings should be clear to hospital administration.
One of the issues in building a robust business case for IDMS is the heterogeneity of IDMS programs when applied to various healthcare institutions and patient populations. Shortening the length of stay by 1 day for ICU patients with diabetes in an urban county hospital will not be the same as providing similar services in a non-intensive care setting in a rural hospital. While the reduced length of stay has been observed for patients with medical admissions, it has not been consistently shown for patients with surgical admissions [31]. The cost savings may also vary based on whether the IDMS is consulted early or later in the patient’s hospital course, and if the consultation is reactive (i.e., after the primary team is unable to manage the patient’s glycemia) or proactive (i.e., patient with increased risk for glycemic complications flagged for IDMS consult upon admission). Evidence-based methodologies for measuring and reporting cost savings are needed.
Two ways of conceptualizing the cost-benefit analysis include cost aversion and throughput. Cost aversion refers to fewer resources being spent on the patient due to improved glycemic outcomes, and the savings here are especially seen for shorter LOS for a predetermined reimbursement tied to a diagnostic-related group [15]. This can be seen as the opportunity cost of improved management from the IDMS relative to the primary care team. Even when the management decision by IDMS is to more intensively manage a patient’s glucose levels, this is likely to result in cost savings. For example, intravenous insulin therapy is costlier than a subcutaneous regimen, but improved glycemic outcomes will decrease rates of central line infection, which range in cost from $3700 to $56,167 per occurrence [49, 50].
When patients are discharged earlier, the increased bed availability enables the hospital to admit more patients with a billable diagnostic code. This cost-benefit is known as “throughput” [15]. Table 2 presents different examples of how cost savings have been reported and discussed in the literature.
IDMS and the COVID-19 Pandemic
In the era of the global COVID-19 pandemic, factors such as the postponement of elective procedures and decreased number of surgical admissions put hospitals across the USA into challenging financial straits. An analysis of rural hospital sustainability found that a quarter of rural hospitals in the USA are at a high risk of shutting down unless improvements are seen in their financial situation [51]. Joblessness during the pandemic will also affect insurance rates across the country, placing further strain on Medicaid programs and making patients less likely to seek health services [52].
Multiple studies have suggested that diabetes is associated with a greater risk of increased morbidity and mortality from COVID-19 infection [52,53,54,55,56], which may be related to glycemic outcomes [56], although a causal association has not yet been shown. IDMS and inpatient glycemia management may be more important now than ever; although simultaneous pressures exist to reduce consultations during the current pandemic. Infection control teams may place a priority on conserving personal protective equipment and reducing the number of provider-patient interactions to minimize the spread of disease within the hospital. Inpatient diabetes telehealth services during the COVID-19 crisis has been successfully implemented across the Johns Hopkins Health System, which allows the hospitals to preserve personal protective equipment and limit physical exposure between patient and provider while increasing access to specialized diabetes care [57]. As noted above, IDMS programs may offer cost savings and can still be deployed efficiently by providing synchronous telehealth visits or asynchronous data review even during the pandemic.
Future IDMS Research Opportunities
Future research can further elucidate whether resources invested in diabetes management programs return both cost and clinical benefits. In a randomized controlled trial of patients receiving IDMS consultation versus patients whose glycemic management is managed solely by the primary team, researchers will be able to control for patient characteristics and compare the impact of an early versus late IDMS referral based on trial design. Controlling for baseline characteristics between both trial groups is expected to amplify the observed benefits of an IDMS team, as patients who are assigned to IDMS in real life tend to be sicker or have more complex glycemic management needs. There is also a need to standardize definitions to better understand the cost savings of IDMS, such as classifying length of stay by 24-h intervals or number of different days the patient remained in the hospital.
Other areas of potential research in glycemic management methods include prospective cohort studies to better understand the impact of IDMS in younger patient populations with type 1 diabetes and resulting prevention of diabetes ketoacidosis-related complications during the inpatient stay. Given the variety of forms a multi-professional diabetes care team can take, more research should be performed to understand the optimal model for healthcare institutions based upon available resources and patient populations. Additionally, studying how IDMS varies across states which have varying penalties for hospital readmissions and under various payment models such as bundled payments is also important.
Conclusion
In this review, we summarized the clinical and financial benefits of IDMS, a hospital program for intensive glycemic management that has been increasingly studied in recent years.
Due to the challenging financial climate in healthcare and the COVID-19 crisis affecting people with diabetes more seriously, the cost-saving aspects of IDMS related to the length of stay, hospital readmissions, hypoglycemia, litigation, resource allocation, and other long-term outcomes will be even more beneficial to hospitals and patients. Most hospitalized patients with diabetes are admitted to community hospitals in the USA (due to a significantly larger number of community hospitals). Although IDMS are commonly established at large academic centers, we have shown that the cost-benefits may translate to the community hospital setting despite differences in staffing models and resources. Further research is needed in the area of the clinical and financial benefit of IDMS, as previous studies are limited by their retrospective methodology and the lack of well-designed prospective studies and control groups.
Data Availability
Not applicable.
Abbreviations
- 30DR:
-
30-day readmission
- ICU:
-
Intensive care unit
- IDMS:
-
Inpatient diabetes management service
- LOS:
-
Length of stay
References
American Diabetes Association. Statistics About Diabetes. 2018. https://www.diabetes.org/resources/statistics/statistics-about-diabetes. Accessed April 13 2020.
Corsino L, Dhatariya K, Umpierrez G. Endotext. 2017.
Association AD. Economic costs of diabetes in the U.S. in 2017. Diabetes Care. 2018;43(4). https://doi.org/10.2337/dci18-0007.
Corl D, Thompson R, Suhr L, Wisse B. Efficacy of diabetes nurse expert team program to improve nursing confidence and expertise in caring for hospitalized patients with diabetes mellitus. J Nurses Prof Dev. 2014;30(3):134–42. https://doi.org/10.1097/NND.0000000000000068.
Levetan C, Passaro M, Jablonski K, Kass M, Ratner R. Unrecognized diabetes among hospitalized patients. Diabetes Care. 1998;21(2):246–9.
Gaines MPR. Impact of hyperglycemia on 30-day readmission rates. Diabetes. 2018;67:Supplement 1. https://doi.org/10.2337/db18-1332-P.
BusinessWire. At a cost of $10,405 per patient stay, hypoglycemia in the hospital cannot be ignored. Glytec. 2019. https://glytecsystems.com/news/at-a-cost-of-10-405-per-patient-stay-hypoglycemia-in-the-hospital-cannot-be-ignored/. Accessed April 26 2020.
Monarch Medical Technologies. Why Inpatient Glycemic Management Matters Monarch Medical Technologies. https://monarchmedtech.com/why-it-matters/. Accessed April 10 2020.
Drincic AT, Akkireddy P, Knezevich JT. Common models used for inpatient diabetes management. Curr Diab Rep. 2018;18(10). https://doi.org/10.1007/s11892-018-0972-x.
American Diabetes Association. 15. Diabetes care in the hospital: standards of medical care in diabetes—2020. Diabetes Care. 2020;43:S193–202.
Schnipper JL, Barsky EE, Shaykevich S, Fitzmaurice G, Pendergrass ML. Inpatient management of diabetes and hyperglycemia among general medicine patients at a large teaching hospital. J Hosp Med. 2006;1(3):145–50. https://doi.org/10.1002/jhm.96.
Rogers S. Inpatient care coordination for patients with diabetes. Diabetes Spectr. 2008;21(4):272–5. https://doi.org/10.2337/diaspect.21.4.272.
Mandel S, Langan S, Mathioudakis N, et al. Retrospective study of inpatient diabetes management service, length of stay and 30-day readmission rate of patients with diabetes at a community hospital. J Community Hosp Intern Med Perspect. 2019;9(2):64–73.
Sidhaye A, Mathioudakis N, Bashura H, Sarkar S, Zilbermint M, Golden S. Building a business case for inpatient diabetes management teams: lessons from our center. Endocr Pract. 2019;25(6):612–5. https://doi.org/10.4158/EP-2018-0471.
Newton CA, Young S. Financial implications of glycemic control: results of an inpatient diabetes management program. Endocr Pract. 2006;12(Suppl 3):43–8. https://doi.org/10.4158/EP.12.S3.43.
Apsey HA, Coan KE, Castro JC, Jameson KA, Schlinkert RT, Cook CB. Overcoming clinical inertia in the management of postoperative patients with diabetes. Endocr Pract. 2014;20(4):320–8. https://doi.org/10.4158/EP13366.OR.
Koproski J, Pretto Z, Poretsky L. Effects of an intervention by a diabetes team in hospitalized patients with diabetes. Diabetes Care. 1997;20:1553–5. https://doi.org/10.2337/diacare.20.10.1553.
Wexler DJ, Beauharnais CC, Regan S, Nathan DM, Cagliero E, Larkin ME. Impact of inpatient diabetes management, education, and improved discharge transition on glycemic control 12 months after discharge. Diabetes Res Clin Pract. 2012;98(2):249–56. https://doi.org/10.1016/j.diabres.2012.09.016.
Mendez CE, Ata A, Rourke JM, Stain SC, Umpierrez G. Daily inpatient glycemic survey (dings): a process to remotely identify and assist in the management of hospitalized patients with diabetes and hyperglycemia. Endocr Pract. 2015;21(8):927–35. https://doi.org/10.4158/EP14577.OR.
Rushakoff R, Sullivan M, MacMaster H, Shah A, Rajkomar A, Glidden D, et al. Association between a virtual glucose management service and glycemic control in hospitalized adult patients: an observational study. Ann Intern Med. 2017;166:621–7.
Dungan KM, Binkley P, Nagaraja HN, Schuster D, Osei K. The effect of glycaemic control and glycaemic variability on mortality in patients hospitalized with congestive heart failure. Diabetes Metab Res Rev. 2011;27(1):85–93. https://doi.org/10.1002/dmrr.1155.
Grey NJ, Perdrizet GA. Reduction of nosocomial infections in the surgical intensive-care unit by strict glycemic control. Endocr Pract. 2004;10(Suppl 2):46–52. https://doi.org/10.4158/EP.10.S2.46.
Golden SH, Peart-Vigilance C, Kao WH, Brancati FL. Perioperative glycemic control and the risk of infectious complications in a cohort of adults with diabetes. Diabetes Care. 1999;22(9):1408–14. https://doi.org/10.2337/diacare.22.9.1408.
Wallia A, Gupta S, Garcia C, Schmidt K, Oakes DJ, Aleppo G, et al. Examination of implementation of intravenous and subcutaneous insulin protocols and glycemic control in heart transplant patients. Endocr Pract. 2014;20(6):527–35. https://doi.org/10.4158/EP13354.OR.
Warrington L, Ayers P, Baldwin AM, Wallace V, Riche KD, Saulters R, et al. Implementation of a pharmacist-led, multidisciplinary diabetes management team. Am J Health Syst Pharm. 2012;69(14):1240–5. https://doi.org/10.2146/ajhp110297.
Kerr L, Kalowes P, Dyo M. Nurse practitioner–led project to achieve euglycemia in cardiac surgery patients. J Nurse Pract. 2017;13(3):e137–e41.
Klinkner G, Murray M. Clinical nurse specialists lead teams to impact glycemic control after cardiac surgery. Clin Nurse Spec. 2014;28(4):240–6. https://doi.org/10.1097/NUR.0000000000000056.
Bansal V, Mottalib A, Pawar T, Abbasakoor N, Chuang E, Chaudhry A, et al. Inpatient diabetes management by specialized diabetes team versus primary service team in non-critical care units: impact on 30-day readmission rate and hospital cost. BMJ Open Diabetes Res Care. 2018;5(6):e000460.
Simmons D, Hartnell S, Watts J, Ward C, Davenport K, Gunn E, et al. Effectiveness of a multidisciplinary team approach to the prevention of readmission for acute glycaemic events. Diabet Med. 2015;32(10):1361–7.
Levetan C, Salas J, Wilets I, Zumoff B. Impact of endocrine and diabetes team consultation on hospital length of stay for patients with diabetes. Am J Med. 1995;99(1):22–8.
Flanagan D, Moore E, Baker S, Wright D, Lynch P. Diabetes care in hospital--the impact of a dedicated inpatient care team. Diabet Med. 2008;25(2):147–51. https://doi.org/10.1111/j.1464-5491.2007.02326.x.
Sampson M, Crowle T, Dhatariya K, et al. Trends in bed occupancy for inpatients with diabetes before and after the introduction of a diabetes inpatient specialist nurse service. Diabet Med. 2006;23:1008–15.
Adigopula S, Feng Y, Babu V, Parperis K, Amoateng-Adjepong Y, Zarich S. Hyperglycemia is associated with increased length of stay and total cost in patients hospitalized for congestive heart failure. World J Cardiovasc Dis. 2013;3:245–9.
Garg R, Schuman B, Bader A, Hurwitz S, Turchin A, Underwood P, et al. Effect of preoperative diabetes management on glycemic control and clinical outcomes after elective surgery. Ann Surg. 2018;267(5):858–62. https://doi.org/10.1097/SLA.0000000000002323.
Carlos A, Estrada M, Young J, et al. Outcomes and perioperative hyperglycemia in patients with or without diabetes mellitus undergoing coronary artery bypass grafting. Ann Thorac Surg. 2011;75:1392–9.
HealthCatalyst. Systematic improvement of diabetes care in the inpatient setting. Health Catalyst. 2017. https://www.healthcatalyst.com/wp-content/uploads/2016/02/Systematic-Improvement-of-Diabetes-Care-in-the-Inpatient-Setting.pdf. Accessed April 5 2020.
Coto J, Yehle K, Foli K. Relationship between standardized glycemic protocols and healthcare cost. Clin Nurs Res. 2014;25(1). https://doi.org/10.1177/1054773814539003.
Spanakis E, Singh L, Siddiqui T, et al. Association of glucose variability at the last day of hospitalization with 30-day readmission in adults with diabetes. BMJ Open Diabetes Res Care. 2020;8:e000990. https://doi.org/10.1136/bmjdrc-2019-000990.
Puig J, Supervia A, Marquez MA, Flores J, Cano JF, Gutierrez J. Diabetes team consultation: impact on length of stay of diabetic patients admitted to a short-stay unit. Diabetes Res Clin Pract. 2007;78(2):211–6. https://doi.org/10.1016/j.diabres.2007.03.010.
Ostling S, Wyckoff J, Ciarkowski SL, Pai C-W, Choe HM, Bahl V, et al. The relationship between diabetes mellitus and 30-day readmission rates. Clin Diabetes Endocrinol. 2017;3(1):3.
Parekh W, Streeton S, Baker-Knight J, Montagnoli R, Nicoziani P, Marchesini G. The economic burden of insulin-related hypoglycemia in adults with diabetes: an analysis from the perspective of the Italian healthcare system. Diabetes Ther. 2018;9(3):1037–47.
Munoz M, Pronovost P, Dintzis J, Kemmerer T, Wang N, Chang Y, et al. Implementing and evaluating a multicomponent inpatient diabetes management program: putting research into practice. Jt Comm J Qual Patient Saf. 2012;38(5):195–206.
2008 Trial Lawyers Report. Hypoglycemic event lawsuit settles for $4 million. Lubin & Meyer PC. 2008. http://www.lubinandmeyer.com/cases/hypoglycemic_malpractice.html. Accessed May 1 2020.
Drugwatch. Jury awards $140M after prescription error Leads to woman’s death. Drugwatch. 2012. https://www.drugwatch.com/news/2012/12/19/jury-awards-140-million-prescription-error-death/. Accessed May 5 2020.
Lilley S, Levine G. Management of hospitalized patients with type 2 diabetes mellitus. Am Fam Physician. 1998;57(5):1079–88.
Kim S. Burden of hospitalizations primarily due to uncontrolled diabetes. Diabetes Care. 2007;30(5):1281–2. https://doi.org/10.2337/dc06-2070.
Beck J, Logan K, Hamm R, Sproat S, Musser K, Everhart P, et al. Reimbursement for pediatric diabetes intensive case management: a model for chronic diseases? Pediatrics. 2004;113(1):e47–50. https://doi.org/10.1542/peds.113.1.e47.
Cheng S, Wang C, Ko Y. Costs and length of stay of hospitalizations due to diabetes-related complications. J Diabetes Res. 2019;2019:1–6. https://doi.org/10.1155/2019/2363292.
O’Grady N, Alexander M, Dellinger E, et al. Guidelines for the prevention of intravascular catheter-related infec- tions. Centers for Disease Control and Prevention. MMWR Recomm Rep. 2002;51(RR-10):1–29.
Dimick J, Pelz R, Consunji R, Swoboda S, Hendrix C, Lipsett P. Increased resource use associated with catheter-related bloodstream infection in the surgical intensive care unit. Arch Surg. 2001;136:229–34.
Guan W, Ni Z, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382:1708–20.
Murphy K. COVID-19 recession to increase uninsurance rates, test Medicaid. Healthpayer Intelligence 2020. https://healthpayerintelligence.com/news/covid-19-recession-to-increase-uninsurance-rates-test-medicaid. Accessed April 2 2020.
Dreher M, Kersten A, Bickenbach J, Balfanz P, Hartmann B, Cornelissen C, et al. The characteristics of 50 hospitalized COVID-19 patients with and without ARDS. Dtsch Arztebl Int. 2020;117:271–8.
Goyal P, Choi J, Pinheiro L, et al. Clinical characteristics of Covid-19 in New York City. N Engl J Med. 2020;382:2372–4. https://doi.org/10.1056/NEJMc2010419.
Li B, Yang J, Zhao F, Zhi L, Wang X, Liu L, et al. Prevalence and impact of cardiovascular metabolic diseases on COVID-19 in China. Clin Res Cardiol. 2020;109:531–8.
Klonoff D, Umpierrez G. COVID-19 in patients with diabetes: risk factors that increase morbidity. Metabolism. 2020;108:154224. https://doi.org/10.1016/j.metabol.2020.154224.
Shelton C, Demidowich AP, Zilbermint M. Inpatient diabetes management during the COVID-19 crisis: experiences from two community hospitals. J Diabetes Sci Technol. 0(0):1932296820930268. https://doi.org/10.1177/1932296820930268.
Acknowledgments
We would like to thank Blair Anton, MLIS, MS, AHIP, associate director for Information Services at William H. Welch Medical Library, Johns Hopkins University, for assistance with the literature review.
Author information
Authors and Affiliations
Contributions
W.Z.H. contributed to all sections. A. P. D. contributed to “Clinical Benefits of IDMS” section. A. S. contributed to “Challenges of IDMS-Related Research” section. S.H.G. provided critical guidance and feedback, M. Z. has overseen this manuscript on all stages of writing. All authors reviewed and edited the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
M.Z. declares consulting for Guidepoint, GLG. Other authors have no conflicts of interest.
Code Availability
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Hospital Management of Diabetes
Rights and permissions
About this article

Cite this article
Haque, W.Z., Demidowich, A.P., Sidhaye, A. et al. The Financial Impact of an Inpatient Diabetes Management Service. Curr Diab Rep 21, 5 (2021). https://doi.org/10.1007/s11892-020-01374-0
Accepted:
Published:
DOI: https://doi.org/10.1007/s11892-020-01374-0