
Abstract
Purpose
As Internet technology evolves, electronic health (e-health) literacy gradually becomes a key factor in healthy behaviors and health-related decision-making. However, little is known about the influencing factors of e-health literacy among cancer survivors. Thus, the objective of this study was to systematically review the status quo, assessment tools, and influencing factors of e-health literacy in cancer patients.
Methods
We conducted a comprehensive search in several databases, including PubMed, MEDLINE, Embase, CINAHL, PsycInfo, Cochrane Library, China National Knowledge Infrastructure, Wanfang Database, Chinese BioMedical Literature Database, and Chinese Science and Technology Journal Database between January 2000 and December 2021.
Results
A total of nine articles were included in this review, all of which were cross-sectional studies. Following the JBI critical appraisal tool, seven of them were rated as high quality. The e-Health Literacy Scale (eHEALS) was the most commonly used measurement for e-health literacy in cancer patients. The level of e-health literacy in cancer survivors was not high, which was associated with a variable of factors. The behavioral model of health services use was adopted to summarize related influencing factors. From an individual’s perspective, predisposing characteristics and enabling resources were the most significant factors, without factors related to needs characteristics.
Conclusion
The study has identified the influencing factors of e-health literacy among cancer survivors, including age, gender, domicile place, education level, information-seeking behavior, and social support. In the future, e-health literacy lectures need to be carried out for elderly cancer patients, especially those who live in rural areas and have no access to the Internet. Families and friends of cancer survivors should also be encouraged to offer them more support.
Implications for Cancer Survivors
These findings of this review provide novel insights for both family members and medical workers to improve e-health literacy in cancer patients. Further research is required to develop easy-to-use electronic health information acquisition devices and establish propagable e-health literacy intervention programs for cancer survivors.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
With the great change in the disease spectrum, cancer has become a central issue in medical health care worldwide. Given the advances and development, cancer has become a chronic disease that can be regulated, treated, and even cured. According to the report published by the International Agency for Research on Cancer (IARC) [1], the number of globally new cancer cases was about 19.3 million and deaths from cancer were almost 10.0 million. Among 112 countries analyzed in the report, cancer had become one of the leading causes of mortality in the world.
As Internet technology and electronic devices develop, e-resources (electronic resources) have become closely related to daily life. Previous research has shown that a large proportion of cancer patients is prone to seek health-related information through the Internet [2,3,4]. Social media also plays a significant role in providing communication platforms and emotional support for cancer patients [5,6,7]. After the outbreak of COVID-19, advantages and promises of telemedicine have been shown to support cancer care [8, 9]. E-resource has become the main access to health care and cancer-related information in the post-pandemic era. However, besides reliable health-related information, the Internet is also crammed with misleading information, particularly during the COVID-19 pandemic [10], which poses great challenges to older patients and influences their trust in online information [11, 12]. Therefore, it is essential to pay attention to cancer patients’ ability to retrieve and use online health information, which is termed as e-health literacy.
According to Norman and Skinner [13], e-health literacy can be defined as the capacity to search for, access, and analyze health information from electronic resources in order to address health issues. Recently, a substantial literature has grown up around the theme of e-health literacy. A bibliometric analysis reported that the research on e-health literacy covers a wide range of topics, including the elderly, students, and patients with various conditions [14]. Among the elderly in China, the status quo of e-health literacy was low and the influencing factors include age, gender, educational level, marital status, and cultural barriers [15]. Research in Turkey has shown that the mean score of e-health literacy in high school students was high and the association between family structure, knowing the importance of health, easy access to the Internet, highly educated parents, and e-health literacy, was found [16]. According to a study by David Ka-Ki Wong et al., e-health literacy among primary care patients in Hong Kong can be predicted by a variety of demographic and behavioral factors, including age, better self-rated health, more frequent Internet use, more frequent online health information seeking, and a wider variety of health information websites [17].
Even though some scholars have started to attach importance to the e-health literacy of cancer patients, there are few studies on the influencing factors of e-health literacy among cancer patients. Therefore, to provide a reference on the development of e-health literacy promotion interventions for cancer patients, we conducted a comprehensive systematic review of multiple databases.
The behavioral model of health services use is one of the most classical models used in the health service care field. This model was set up in 1968 by Dr. Andersen, a professor at the University of Chicago [18]. After the fifth revision and evolvement, now the model is composed of contextual characteristics, individual characteristics, health behavior, and health outcomes [19]. In this model, the dimension of contextual characteristics and individual characteristics, as factors influencing health behavior, has the same indicator structure and path relations, including predisposing characteristics, enabling characteristics, and needs characteristics. In this review, we adopted the three variables in the individual characteristics of this model to summarize the influencing factors.
The purpose of this review set out to (1) better understand the status quo of cancer patients, (2) identify the evaluating tools used in patients living with cancer, and (3) explore the factors influencing e-health literacy in adult cancer patients under the guidance of the behavioral model of health services use.
Methods
This systematic review was performed in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. The protocol of this review was registered in the International Prospective Register of Systematic Reviews (registration number: CRD42021292673).
Search and study selection
Two reviewers (YZ and PRX) conducted a comprehensive search in MEDLINE, CINAHL, PubMed, Embase, PsycInfo, Cochrane Library, China National Knowledge Infrastructure, WanFang Database, China Science and Technology Journal Database (VIP), and Chinese BioMedical Literature Database (SinoMed). Considering that e-health literacy was a concept developed in the early 2000s, we searched the relevant literature published from January 2000 to December 2021 [13]. The following combinations of MeSH terms and free terms were used: (Cancer survivors) OR (Cancer survivor) OR (Survivors, Cancer) OR (Long-term cancer survivors) OR (Cancer survivors, Long-term) OR (Cancer survivor, Long-term) OR (Long term cancer survivors) OR (Long-term Cancer survivor) OR (Survivor, Long-Term Cancer) OR (Survivors, Long-Term Cancer) OR (cancer patients) OR (cancer patient) OR (oncology patient) OR (oncology patients) OR (patients with cancer) OR (patient with cancer) OR [Cancer survivors] explode all trees AND (e-health literacy) OR (eHealth literacy) OR (e-health literacies) OR (eHealth literacies) OR (digital literacy) OR (digital literacies) OR (electronic literacy) OR (electronic literacies). In the process of literature screening, all the articles selected from electronic databases were imported to Rayyan (a website for intelligent systematic review). The identification and exclusion of duplicates were also completed on this website. Two researchers (YZ and PRX) conducted preliminary screening according to the title and abstract of the articles. Then the secondary filter was independently performed by full-text reading. The screening results were cross-checked after that. Additionally, the bibliographies of included papers were carefully searched for subsequent publication. If there was no consensus, a third researcher would determine the dispute.
Inclusion and exclusion criteria
The following criteria were used to include related articles: (1) patients ≥ 18 years old; (2) patients diagnosed with cancer, regardless of the cancer stage and whether they received any form of treatment; (3) original studies. Studies were excluded if (1) not related to the research topic; (2) not relevant to cancer patients; (3) the study was a meta-analysis, abstract, systematic review, case report, conference report, qualitative research, or intervention study; (4) written in a language other than English and Chinese.
Quality assessment
The quality of included articles was assessed by Joanna Briggs Institute (JBI) critical appraisal tool for cross-sectional studies. This appraisal tool consists of 8 items, evaluating the overall quality from the perspective of the study subject, diseases, measurement of influencing factors, confounding factors, and data analysis. Each item would be classified into yes, no, unclear, and not applicable [20]. Articles with more than 5 entries “yes,” 3–5 entries of “yes,” and less than 3 entries of “yes” are respectively ranked as high, moderate, and low quality [21]. Two reviewers (YZ and PRX) individually evaluated the quality of each study and conflicts would be resolved by a third researcher.
Data extraction and synthesis
YZ and PRX separately completed data extraction and reached an agreement through discussion. The extracted data included the first author, year, country, study design, study setting, study population, e-health literacy measure, e-health literacy status, results, and influencing factors. The results of the included research were summarized using descriptive and narrative syntheses. We did not conduct a meta-analysis because of the heterogeneity of studies included.
Results
Search results
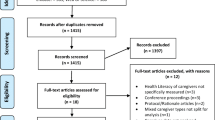
Figure 1 shows the PRISMA flow diagram of the searching and selection process. A total of 933 studies were initially screened from ten electronic databases and 5 additional articles were identified through bibliographies. A total of 229 duplicates were removed, and 709 records were retained. After preliminary screening according to the title and abstract, 10 studies were eligible for full-text screening. A total of nine articles were eventually included in this review, with one being excluded because of foreign language.

PRISMA flow diagram of the study selection process
The characteristics and quality of the included studies
Included nine papers were all cross-sectional studies. Four of the studies [22,23,24,25] were conducted in China, two [26, 27] of them were from Germany, and the rest [28,29,30] were from the USA, England, and Canada. Sample sizes ranged from 83 to 2009 and a total of 3243 cancer patients were included in this review. Six studies [22, 24,25,26,27,28] focused on mixed cancer types, with three [23, 29, 30] articles focusing on one specific type of cancer. Breast cancer, colorectal cancer, and lung cancer were the most commonly studied in all the papers. Detailed information on the features of the studies included is provided in Table 1. Quality assessment results had indicated that based on the JBI critical appraisal tool, most of the studies [22,23,24,25, 28,29,30] were of high quality, with two [26, 27] being ranked as moderate quality. Table 2 provides the results of the quality evaluation.
Measurement of e-health literacy
As for the assessment tool of e-health literacy, almost all the studies (7 of 9) used the same measurement: the e-Health Literacy Scale (eHEALS) [13]. Four studies employed the Chinese version of the eHEALS Scale, which has been tested to have reasonable reliability and validity among the Chinese population [31]. Only two studies used the modified version of the eHEALS scale [26, 27].
Status quo of e-health literacy among cancer patients
Most of the studies in the nine articles included found that e-health literacy among cancer patients still needs to be improved. The total score of eHEALS is 40, and a score of 32 or above is considered qualified e-health literacy [32, 33]. Among the seven studies adopting the eHEALS scale as an evaluation tool, the majority of articles showed that e-health literacy was less than 32 scores, which did not meet the qualified standard. Concerning the five-question scale, the total score is 25, with an average score of 14.7. Heiman et.al. used average scores as the dividing line, with 58.5% of patients scoring above average and 41.5% below average, and below average is considered a low e-health literacy score [26]. In regard to the modified 8-item eHEALS scale, Likert 10-level scoring method was used in this scale, with a total score of 80 points, and no classification criteria were provided. The author only provided the average score of each item, not mentioning the total scores. In the article, each item is compared with each other to determine the score level. For example, compared with the item with average score of 6.1, the item with less than 5 points was considered as low score. Of the 8 items, 3 items averaged more than 6 points and 5 items averaged less than 5 points [27].
Influencing factors
In this review, influencing factors were categorized into predisposing factors, enabling factors, and need factors using the behavioral model of health services use (seen in Fig. 2).

Influencing factors in the theoretical framework
Predisposing factors of e-health literacy
Predisposing characteristics consist of demographics, social structure, and health beliefs. In this systematic review, predisposing factors include age, sex, education level, and domicile place. Eight of nine studies reported factors that can be divided into predisposing variables [22,23,24,25, 27,28,29,30]. Among the eight articles, six showed that age is a significant factor impacting the e-health literacy of cancer patients [23,24,25, 27,28,29]. Elderly cancer patients had a lower level of trust in locating and recognizing meaningful health information on the Internet and had a lower e-health literacy score [28]. The results of 5 studies [22, 23, 25, 29, 30] found that education level was positively correlated with e-health literacy of cancer patients, which indicated that the higher the education level patients received, the higher their score of e-health literacy. Gender was reported to be associated with e-health literacy by Zhou et al. [22], which found female cancer patients had a higher level of e-health literacy than male patients. Besides, one study also identified domicile place was the influencing factor of e-health literacy [24]. The e-health literacy score of cancer patients living in urban areas was higher than that of rural cancer patients.
Enabling factors of e-health literacy
Enabling variables refer to the quantity and distribution of labor and capital, education, and development of health care personnel and infrastructure. Enabling factors in this review involved having access to a mobile service, health knowledge-seeking, access to e-resources, frequency of searching for online health information, whether willing to use the Internet to find health information, types of websites preferred to search for health information, the number of Internet tools, frequency of discussion with family members about using the Internet to find health resources, health knowledge contribution, and emotional support behavior. Six articles have indicated that accesses and behaviors of online information seeking were factors influencing eHealth literacy in cancer patients [22,23,24, 26, 29, 30]. Results of Moon et al. and Milne et al. [29, 30] showed that having easy access to e-resources via smartphones or other mobile devices was a predictor of higher e-health literacy. Frequent search for online health information was also reported to be significantly correlated with e-health literacy [23, 26]. Zhou et al. [22] found that health knowledge-seeking, health knowledge contribution, and emotion support behaviors were positively associated with eHealth literacy. Frequency of discussing with family members about using the Internet to find health resources was identified as a predictor of e-health literacy, indicating that the more frequently they discussed with family members about how to find online health information, the higher the e-health literacy among cancer patients [24]. In addition, whether willing to use the Internet to find health information and websites preferred to search for health information were shown to be influencing factors [23]. Patients willing to use the Internet for information seeking scored higher in e-health literacy. And the e-health literacy score of patients who preferred official disease websites was higher than those who preferred non-official health websites.
Need factors of e-health literacy
Perception needs and assessment needs are included in need characteristics. In this review, none of the influencing factors synthesized matched the definition of need factors.
In addition, several factors that measured were not associated with e-health literacy among cancer patients. These factors included deprivation level, rural/urban classification, living situation, overall health, histology, overall quality of life, marital status, type of health insurance, and the number of chemotherapy, tumor type, tumor stage, and BMI. Moon et.al. found that deprivation level and rural or urban classification were not associated with e-health literacy in cancer patients [29]. Living situation and histology were reported to be irrelevant with e-health literacy. Self-perceived health status, such as overall health and overall quality of life, was also found to be not correlated with e-health literacy [30]. Kang et.al. found no significant difference between marital status and BMI in e-health literacy among cancer patients [24]. Similarly, disease characteristics like time of diagnosis, tumor type, tumor stage, and number of chemotherapy treatments were not reported to be significantly associated with eHealth literacy among cancer patients [24, 25].
Discussion
A number of studies have noted that cancer patients increasingly rely on the Internet for their source of health information [34, 35]. The ability to correctly search for and use health information acquired from the e-resources, which is termed as e-health literacy, was reported to promote the development of healthy behaviors and contribute to health-related decision-making [36, 37]. In recent years, there has been worldwide recognition of the importance of e-health literacy. However, few research examined the e-health literacy of cancer patients. The objective of this research was to examine the evidence for the current status, measurements, and variables impacting e-health literacy among cancer patients. This study identified nine relevant papers, finding that the e-health literacy in cancer patients was not high and still needs to be improved. According to the individual characteristics in the behavioral model of health services use [19], we classified the factors synthesized into predisposing factors and enabling factors. However, the results showed that there was no factor in line with the criteria of need factors, indicating that more research is needed in the future to focus on the correlation between eHealth literacy of cancer patients and need factors such as perceived needs and assessed needs.
As stated in the results, the current status of cancer patients’ e-health literacy was not high. In the articles adopting the eHEALS, the mean score was around 24 to 28 on the premise that the total score is 40. Compared with four studies conducted in China [22,23,24,25], researchers in England and the USA found that cancer patients in their countries scored higher in e-health literacy, though still lower than younger people [28, 29]. Chinese people were exposed to the Internet and mobile healthcare late in comparison to western developed countries, especially in middle-aged and elderly people living with cancer, which may help explain the disparity between the studies. Another included study from Germany also reported similar results, with 58.5% of patients were above the average score. A study from Spain on diabetes found that elderly diabetes patients had a lower degree of e-health literacy, with a mean score of 22.35 [38]. Stellefson et al. reported that individuals with chronic obstructive pulmonary disease had a high degree of e-health literacy, finding that the average score was 29.11 [39]. Our results suggest that in general, cancer patients’ eHealth literacy is not high, which was parallel to the results of other chronic diseases. However, cancer patients still face a number of challenges when searching for health information and using the Internet to solve their health problems. In particular, they often have problems identifying websites that are reliable sources of health information [40]. Therefore, in the future, medical staff should pay more attention to the information needs and information search behavior of cancer patients and provide more reliable mobile platforms for cancer-related information.
Another finding of this review was that most studies included adopted the e-Health Literacy Scale (eHEALS), which has been translated into more than ten languages all around the world [41,42,43,44,45,46,47,48,49,50,51]. Since Norman et al. were the first to define eHealth literacy, which was the most widely cited, the majority of researchers tended to select the eHEALS or its translation as the evaluation tool for e-health literacy. Only two articles from Germany chose to use self-modified scales as their assessment tools. However, the sample of the two adapted scales was only targeted at participants who took part in a lecture program in Germany and were not representative. Future studies using these two measurements may require reliability and validity tests in their study population. Although a variety of measuring tools has been developed [52,53,54], the eHEALS remains the most commonly used scale for e-health literacy. Nevertheless, with the development of mobile healthcare and the evolution of web 2.0, there has shown several shortcomings in the eHEALS [55]. Further research on e-health literacy should focus more on developing interactive and targeted measurements.
In the predisposing characteristics, age, gender, education level, and domicile place were the main factors. With getting older, the body functions gradually aging, resulting in the decrease of old people’s acceptance, understanding, memory, and learning ability of new things, which may lead to a low score of e-health literacy [56]. The association between gender and e-health literacy has not reached a consensus yet. A study conducted in China [22] found that Chinese female cancer patients had a higher level of e-health literacy than male patients. However, the findings of Zibrik L et al. showed that female participants in British Columbia’s immigrant Chinese were less skilled at online health information seeking and evaluation than male participants while the results were reversed among Punjabi participants [57]. Cam Escoffery et al. did not observe a significant association between gender and e-health literacy in American adults [58]. The differences between the results may be explained by cultural diversity. In the future, more study is needed to clarify the unique association between genders and e-health literacy in various cultures. Several studies reported that people who received more education scored higher in e-health literacy [29, 30, 59, 60]. Well-educated people were more likely to have higher ability of information seeking and screening and can better obtain and use health information in their health-related decision. Domicile place was found to be significantly correlated with e-health literacy [61], which could be argued that the economic and infrastructure differences between urban and rural areas make it easier for urban residents to access social resources and information channels, which enables them to know how to get more health information online and master more skills on information discrimination [24]. Thus, it is critical to give importance to the information needs of older cancer patients in rural areas, particularly those with low levels of education.
At the enabling characteristics, preference, attitude, frequency, and access to online health knowledge-seeking were explored to be the main influencing factors. Our findings showed that having access to the Internet or a mobile device plays a crucial role in the ability to acquire and evaluate health-related information, which has been reported by a number of studies [16, 29, 30]. Recently, smartphones have become the main device to access the Internet, which allows participants to look for health symptoms and health-related factors at any time and to have a higher level of e-health literacy [62]. The positive association with frequency of looking for health information on the Internet and e-health literacy was also found in college students and patients in the primary clinic [17, 63]. This finding could be explained by that frequent online search improves the ability to judge whether a website is reliable and to identify the correct health information. Besides, the type of websites people used for seeking health information was also a predictor of e-health literacy [23]. The impact of cancer patients’ attitudes towards online health information on e-health literacy also cannot be ignored [22]. Several studies have indicated that even though most people mastered the skills to seek health information online, they were skeptical of the information they found and did not feel confident about using it to make health decisions [64, 65]. Adults with a positive attitude towards online health information were reported to have a higher score of e-health literacy [66]. This difference may be partly explained by KAP model (knowledge, attitude, practice) as knowledge and attitudes are motivations of behavior change [67]. In a word, efforts should be made to make e-resources more accessible to individuals, and lectures should be carried out to remove barriers to online information seeking. In addition, this review found that support from families and friends could help improve e-health literacy in cancer patients, which was consistent with previous studies [22, 24, 59]. Patients with diabetes were also reported to usually ask family and friends for help in the acquisition of online health information, which emphasized the significance of information support from relatives and friends [68]. Therefore, medical workers need to encourage family members and friends of cancer patients to attach more importance to communication with them, not only to care about their health status and treatment process, but also to take their information needs into account.
In this review, there were no factors belonging to the need characteristics, which could have implications for us. There may be a relationship between predisposing characteristics and enabling characteristics that influence e-health literacy, and in the future, consideration should be given on how to improve e-health literacy for aging rural cancer patients who are less educated and have less access to e-resources. One study found no correlation between perceived needs and e-health literacy in cancer patients while other studies did not include these need factors, making the findings less reliable and requiring more evidence [30]. Thus, we were also inspired by the fact that very few studies had evaluated the perceived needs and evaluation needs of cancer patients in terms of e-health literacy. There is a need to explore the association between patient-reported health status, mental health status, health-related objective indicators, and e-health literacy in cancer patients. In addition, two included studies in our review found no significant correlation between disease-related factors such as diagnosis time, tumor type, tumor stage, and e-health literacy of cancer patients [24, 25]. One possible reason is that the concept of e-health literacy is relatively new and few studies focus on the impact of different cancer treatments and treatment-related adverse effect on e-health literacy. There is abundant room for further progress in determining the association between e-health literacy and cancer-related characteristics.
Compared with studies in other populations, studies on e-health literacy in cancer patients focus more on the enabling factors, especially the access and use of the Internet, such as health knowledge seeking, access to e-resources, and the types of websites preferred to search for health information. Scholars’ research on e-health literacy among adolescents, college students, and residents mostly pays attention to the predisposing characteristics. For example, a survey of residents over the age of 15 in Shandong Province, China, showed that age, education level, residence place, employment status, household income, incidence of chronic diseases, type of medical insurance, and social support were the main influencing factors for e-health literacy of residents [69]. A cluster survey of 1300 primary and secondary school students in Shaanxi Province, China, found that age, grade, father’s education level, parents’ addiction to mobile phones, and general self-efficacy were the predictors of electronic health literacy among them [70]. Some studies also discussed the correlation between e-health literacy and enabling factors. For instance, Zhang et.al. found that caregiver’s e-health literacy was the main influencing factor of stroke patients’ electronic health literacy, which were not measured in studies of cancer patients [71]. Future research should pay more attention to the impact of caregivers and families of cancer patients on patients’ e-health literacy. The correlation between need factors and e-health literacy was also measured in other populations. A study of 1115 female nursing college students found that e-health literacy was positively associated with depressive symptoms [72]. Similarly, another systematic review showed that physical and mental conditions were important influencing factors of electronic health literacy among the elderly [15]. A further study with more focus on the psychological status on the e-health literacy of cancer patients is therefore suggested.
Limitations
There also exist some limitations in this review. Firstly, we only included English and Chinese articles, which may result in the exclusion of relevant studies. Secondly, all the included papers are cross-sectional studies. Intervention studies and qualitative studies were not included, which could lead to the incompleteness of the findings. Further research expanding the study types included would be worthwhile. Besides, two studies included adopted different evaluation tools, which would give rise to the increase of heterogeneity of the results.
Conclusion
This review has shown that the e-health literacy of cancer patients is not very high and influenced by various factors. Factors summarized are divided into predisposing factors and enabling factors in the light of the behavioral model of health services use. The new understanding could shed light on e-health literacy interventions for cancer patients. For instance, it is necessary for medical workers to attach importance to health education of health knowledge-seeking in cancer patients. Also, the development of easy-to-use and highly accessible cancer-related information online platforms and mobile applications is needed. Furthermore, family members and caregivers of cancer patients should enhance communication and discussion with them on utilization and acquisition of e-resources. In the future, more research needs to be carried out to explore specific and practical intervention projects for the improvement of e-health literacy in cancer patients.
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–49. https://doi.org/10.3322/caac.21660.
Soto-Perez-de-Celis E, Perez-Montessoro V, Rojo-Castillo P, Chavarri-Guerra Y. Health-related information-seeking behaviors and preferences among mexican patients with cancer. J Cancer Educ. 2018;33(3):505–9. https://doi.org/10.1007/s13187-018-1334-8.
Chua GP, Tan HK, Gandhi M. Information sources and online information seeking behaviours of cancer patients in Singapore. Ecancermedicalscience. 2018;12:880. https://doi.org/10.3332/ecancer.2018.880.
Inglehart RC, Taberna M, Pickard RK, Hoff M, Fakhry C, Ozer E, et al. HPV knowledge gaps and information seeking by oral cancer patients. Oral Oncol. 2016;63:23–9. https://doi.org/10.1016/j.oraloncology.2016.10.021.
Stiles BM, Mynard JN. Social media and your cancer patient. semin thorac cardiovasc surg. 2021;33(2):517–21. https://doi.org/10.1053/j.semtcvs.2020.12.014.
Falisi AL, Wiseman KP, Gaysynsky A, Scheideler JK, Ramin DA, Chou WS. Social media for breast cancer survivors: a literature review. J Cancer Surviv. 2017;11(6):808–21. https://doi.org/10.1007/s11764-017-0620-5.
Braun LA, Zomorodbakhsch B, Keinki C, Huebner J. Information needs, communication and usage of social media by cancer patients and their relatives. J Cancer Res Clin Oncol. 2019;145(7):1865–75. https://doi.org/10.1007/s00432-019-02929-9.
Shirke MM, Shaikh SA, Harky A. Implications of telemedicine in oncology during the COVID-19 pandemic. Acta Biomed. 2020;91(3):e2020022. https://doi.org/10.23750/abm.v91i3.9849.
Lloyd J, Lee CJ. Use of telemedicine in care of hematologic malignancy patients: challenges and opportunities. Curr Hematol Malig Rep. 2022:1–6. https://doi.org/10.1007/s11899-021-00642-4.
Rathore FA, Farooq F. Information overload and infodemic in the COVID-19 pandemic. J Pak Med Assoc. 2020;70((Suppl 3) (5)):S162-s5. https://doi.org/10.5455/jpma.38.
Kummervold PE, Chronaki CE, Lausen B, Prokosch HU, Rasmussen J, Santana S, et al. eHealth trends in Europe 2005–2007: a population-based survey. J Med Internet Res. 2008;10(4):e42. https://doi.org/10.2196/jmir.1023.
Lange L, Peikert ML, Bleich C, Schulz H. The extent to which cancer patients trust in cancer-related online information: a systematic review. PeerJ. 2019;7:e7634. https://doi.org/10.7717/peerj.7634.
Norman CD, Skinner HA. eHealth literacy: essential skills for consumer health in a networked world. J Med Internet Res. 2006;8(2):e9. https://doi.org/10.2196/jmir.8.2.e9.
Wang C, Wu X, Qi H. A comprehensive analysis of e-health literacy research focuses and trends. Healthcare (Basel). 2021;10(1). https://doi.org/10.3390/healthcare10010066.
Shi Y, Ma D, Zhang J, Chen B. In the digital age: a systematic literature review of the e-health literacy and influencing factors among Chinese older adults. Z Gesundh Wiss. 2021:1–9. https://doi.org/10.1007/s10389-021-01604-z.
Tümer A, Sümen A. E-health literacy levels of high school students in Turkey: results of a cross-sectional study. Health Promot Int. 2021. https://doi.org/10.1093/heapro/daab174.
Wong DK, Cheung MK. Online health information seeking and eHealth literacy among patients attending a primary care clinic in Hong Kong: a cross-sectional survey. J Med Internet Res. 2019;21(3):e10831. https://doi.org/10.2196/10831.
Andersen R. A behavioral model of families' use of health services. A behavioral model of families' use of health services. 1968(25).
Andersen RM, Davidson PL, Baumeister SE. Improving access to care in America. Changing the US health care system: key issues in health services policy and management 3a edición San Francisco: Jossey-Bass. 2007:3–31.
Moola S MZ, Tufanaru C, Aromataris E, Sears K, Sfetcu R, Currie M, Qureshi R, Mattis P, Lisy K, Mu P-F. Chapter 7: systematic reviews of etiology and risk [M/OL]. JBI Manual for Evidence Synthesis, 2020[https://synthesismanual.jbi.global.
Liberali R, Del Castanhel F, Kupek E, Assis MAA. Latent class analysis of lifestyle risk factors and association with overweight and/or obesity in children and adolescents: systematic review. Child Obes. 2021;17(1):2–15. https://doi.org/10.1089/chi.2020.0115.
Zhou J, Wang C. Improving cancer survivors’ e-health literacy via online health communities (OHCs): a social support perspective. J Cancer Surviv. 2020;14(2):244–52. https://doi.org/10.1007/s11764-019-00833-2.
Zhao Y, Wang J, Wu T, Zhang R. Analysis of current situation and influencing factors of eHealth literacy in patients with enterostomy. J Nurs Adm. 2021;21(11):805–9+18.
Kang D, Lu Y, Wang Y. Current situation and influencing factors of eHealth literacy in tumor patients. Chin J Mod Nurs. 2020;26(22):2998–3004.
Zhang L. Research on status and influencing factors of electronic health literacy in cancer patients. Chin J Prim Med Pharm. 2018;25(20):2689–92.
Heiman H, Keinki C, Huebner J. EHealth literacy in patients with cancer and their usage of web-based information. J Cancer Res Clin Oncol. 2018;144(9):1843–50. https://doi.org/10.1007/s00432-018-2703-8.
Halwas N, Griebel L, Huebner J. eHealth literacy, Internet and eHealth service usage: a survey among cancer patients and their relatives. J Cancer Res Clin Oncol. 2017;143(11):2291–9. https://doi.org/10.1007/s00432-017-2475-6.
Hoogland AI, Mansfield J, Lafranchise EA, Bulls HW, Johnstone PA, Jim HSL. eHealth literacy in older adults with cancer. J Geriatr Oncol. 2020;11(6):1020–2. https://doi.org/10.1016/j.jgo.2019.12.015.
Moon Z, Zuchowski M, Moss-Morris R, Hunter MS, Norton S, Hughes LD. Disparities in access to mobile devices and e-health literacy among breast cancer survivors. Support Care Cancer. 2022;30(1):117–26. https://doi.org/10.1007/s00520-021-06407-2.
Milne RA, Puts MT, Papadakos J, Le LW, Milne VC, Hope AJ, et al. Predictors of high eHealth literacy in primary lung cancer survivors. J Cancer Educ. 2015;30(4):685–92. https://doi.org/10.1007/s13187-014-0744-5.
Guo S, Yu X, Sun Y, Nie D, Li X, Wang L. Adaptation and evaluation of Chinese version of eHEALS and its usage among senior high school students. Chin J Health Educ. 2013;29(02):106–8+23. https://doi.org/10.16168/j.cnki.issn.1002-9982.2013.02.019.
Meng S, Shen C. Current situation of eHealth literacy and health behaviors of college students in Nanjing. Chin J Health Educ. 2018;34(03):254–7.
Li S, Xu H, Cui G. Analysis of eHealth literacy and its influencing factors among the elderly. Chin J Dis Control Prev. 2019;23(11):1318–22. https://doi.org/10.16462/j.cnki.zhjbkz.2019.11.004.
Keinki C, Seilacher E, Ebel M, Ruetters D, Kessler I, Stellamanns J, et al. Information needs of cancer patients and perception of impact of the disease, of self-efficacy, and locus of control. J Cancer Educ. 2016;31(3):610–6. https://doi.org/10.1007/s13187-015-0860-x.
Ebel MD, Stellamanns J, Keinki C, Rudolph I, Huebner J. Cancer patients and the Internet: a survey among German cancer patients. J Cancer Educ. 2017;32(3):503–8. https://doi.org/10.1007/s13187-015-0945-6.
Becker D, Grapendorf J, Greving H, Sassenberg K. Perceived threat and Internet use predict intentions to get bowel cancer screening (Colonoscopy): longitudinal questionnaire study. J Med Internet Res. 2018;20(2):e46. https://doi.org/10.2196/jmir.9144.
Mitsutake S, Shibata A, Ishii K, Oka K. Associations of eHealth literacy with health behavior among adult Internet users. J Med Internet Res. 2016;18(7):e192. https://doi.org/10.2196/jmir.5413.
Aponte J, Nokes KM. Electronic health literacy of older Hispanics with diabetes. Health Promot Int. 2017;32(3):482–9. https://doi.org/10.1093/heapro/dav112.
Stellefson ML, Shuster JJ, Chaney BH, Paige SR, Alber JM, Chaney JD, et al. Web-based health information seeking and eHealth literacy among patients living with chronic obstructive pulmonary disease (COPD). Health Commun. 2018;33(12):1410–24. https://doi.org/10.1080/10410236.2017.1353868.
Lange-Drenth L, Schulz H, Endsin G, Bleich C. Patients with cancer searching for cancer- or health-specific web-based information: performance test analysis. J Med Internet Res. 2021;23(8):e23367. https://doi.org/10.2196/23367.
Wångdahl J, Dahlberg K, Jaensson M, Nilsson U. Arabic version of the electronic health literacy scale in Arabic-speaking individuals in sweden: prospective psychometric evaluation study. J Med Internet Res. 2021;23(3):e24466. https://doi.org/10.2196/24466.
van der Vaart R, van Deursen AJ, Drossaert CH, Taal E, van Dijk JA, van de Laar MA. Does the eHealth literacy scale (eHEALS) measure what it intends to measure? Validation of a Dutch version of the eHEALS in two adult populations. J Med Internet Res. 2011;13(4): e86. https://doi.org/10.2196/jmir.1840.
Soellner, Renate, Huber, Stefan, Reder, Maren. The concept of eHealth literacy and its measurement: German translation of the eHEALS. Journal of Media Psychology: Theories. 2014.
Efthymiou A, Middleton N, Charalambous A, Papastavrou E. Adapting the eHealth literacy scale for carers of people with chronic diseases (eHeals-Carer) in a sample of Greek and cypriot carers of people with dementia: reliability and validation study. J Med Internet Res. 2019;21(11):e12504. https://doi.org/10.2196/12504.
Diviani N, Dima AL, Schulz PJ. A psychometric analysis of the Italian version of the eHealth literacy scale using item response and classical test theory methods. J Med Internet Res. 2017;19(4):e114. https://doi.org/10.2196/jmir.6749.
Mitsutake S, Shibata A, Ishii K, Okazaki K, Oka K. Developing Japanese version of the eHealth Literacy Scale (eHEALS). Nihon Koshu Eisei Zasshi. 2011;58(5):361–71.
Chung S, Park BK, Nahm ES. The Korean eHealth literacy scale (K-eHEALS): reliability and validity testing in younger adults recruited online. J Med Internet Res. 2018;20(4):e138. https://doi.org/10.2196/jmir.8759.
Brors G, entzel-Larsen TW, Dalen H, Hansen TB, Norman CD, Wahl A, et al. Validity and reliability of the Norwegian version of the eHealth literacy scale (eHEALS) among patients after percutaneous coronary intervention. European Journal of Cardiovascular Nursing. 2021(Supplement_1):Supplement_1.
Duplaga M, Sobecka K, Wójcik S. The reliability and validity of the telephone-based and online polish eHealth literacy scale based on two nationally representative samples. Int J Environ Res Public Health. 2019;16(17). https://doi.org/10.3390/ijerph16173216.
Tomás CC, Oliveira E, Sousa D, Uba-Chupel M, Furtado G, Rocha C, et al. Proceedings of the 3rd IPLeiria’s International Health Congress: Leiria, Portugal. 6–7 May 2016. BMC Health Serv Res. 2016;16 Suppl 3(Suppl 3):200. https://doi.org/10.1186/s12913-016-1423-5.
Paramio Pérez G, Almagro BJ, Hernando Gómez Á, Aguaded Gómez JI. Validation of the eHealth literacy scale (eHEALS) in Spanish university students. Rev Esp Salud Publica. 2015;89(3):329–38. https://doi.org/10.4321/s1135-57272015000300010.
Seçkin G, Yeatts D, Hughes S, Hudson C, Bell V. Being an informed consumer of health information and assessment of electronic health literacy in a national sample of Internet users: validity and reliability of the e-HLS instrument. J Med Internet Res. 2016;18(7):e161. https://doi.org/10.2196/jmir.5496.
van der Vaart R, Drossaert C. Development of the digital health literacy instrument: measuring a broad spectrum of health 1.0 and health 2.0 skills. J Med Internet Res. 2017;19(1):e27. https://doi.org/10.2196/jmir.6709.
Karnoe A, Furstrand D, Christensen KB, Norgaard O, Kayser L. Assessing competencies needed to engage with digital health services: development of the eHealth literacy assessment toolkit. J Med Internet Res. 2018;20(5):e178. https://doi.org/10.2196/jmir.8347.
Norman C. eHealth literacy 2.0: problems and opportunities with an evolving concept. J Med Internet Res. 2011;13(4):e125. https://doi.org/10.2196/jmir.2035.
Liu Z, Zhang H, Zhang Y, Du C, Li H, Zhao J, et al. Current situation and influencing factors of e-health literacy among rural older adults in Zhengzhou. Mod Prev Med. 2020;47(02):283–6+309.
Zibrik L, Khan S, Bangar N, Stacy E, Novak Lauscher H, Ho K. Patient and community centered eHealth: exploring eHealth barriers and facilitators for chronic disease self-management within British Columbia’s immigrant Chinese and Punjabi seniors. Health Policy and Technology. 2015;4(4):348–56. https://doi.org/10.1016/j.hlpt.2015.08.002.
Escoffery C. Gender similarities and differences for e-Health behaviors among U.S. adults. Telemed J E Health. 2018;24(5):335–43. https://doi.org/10.1089/tmj.2017.0136.
Song L, Tatum K, Greene G, Chen RC. eHealth literacy and partner involvement in treatment decision making for men with newly diagnosed localized prostate cancer. Oncol Nurs Forum. 2017;44(2):225–33. https://doi.org/10.1011/17.Onf.225-233.
Del Giudice P, Bravo G, Poletto M, De Odorico A, Conte A, Brunelli L, et al. Correlation between eHealth literacy and health literacy using the eHealth literacy scale and real-life experiences in the health sector as a proxy measure of functional health literacy: cross-sectional web-based survey. J Med Internet Res. 2018;20(10):e281. https://doi.org/10.2196/jmir.9401.
Özkan O, Özer Ö, Özmen S, Budak F. Investigation of the perceived coronavirus threat, e-health literacy, and psychological well-being in Turkey. Soc Work Public Health. 2022;37(2):122–34. https://doi.org/10.1080/19371918.2021.1986451.
James DC, Harville C 2nd. eHealth literacy, online help-seeking behavior, and willingness to participate in mHealth chronic disease research among African Americans, Florida, 2014–2015. Prev Chronic Dis. 2016;13:E156. https://doi.org/10.5888/pcd13.160210.
Tariq A, Khan SR, Basharat A. Internet use, eHealth literacy, and dietary supplement use among young adults in Pakistan: cross-sectional study. J Med Internet Res. 2020;22(6):e17014. https://doi.org/10.2196/17014.
Dopelt K, Avni N, Haimov-Sadikov Y, Golan I, Davidovitch N. Telemedicine and eHealth literacy in the Era of COVID-19: a cross-sectional study in a peripheral clinic in Israel. Int J Environ Res Public Health. 2021;18(18). https://doi.org/10.3390/ijerph18189556.
Park H, Lee E. Self-reported eHealth literacy among undergraduate nursing students in South Korea: A pilot study. Nurse Educ Today. 2015;35(2):408–13.
Yang E, Chang SJ, Ryu H, Kim HJ, Jang SJ. Comparing factors associated with eHealth literacy between young and older adults. J Gerontol Nurs. 2020;46(8):46–56. https://doi.org/10.3928/00989134-20200707-02.
Chukmaitov A, Wan TT, Menachemi N, Cashin C. Breast cancer knowledge and attitudes toward mammography as predictors of breast cancer preventive behavior in Kazakh, Korean, and Russian women in Kazakhstan. Int J Public Health. 2008;53(3):123–30. https://doi.org/10.1007/s00038-008-7001-9.
Sjöström A, Hajdarevic S, Hörnsten Å, Öberg U, Isaksson U. Experiences of online COVID-19 information acquisition among persons with type 2 diabetes and varying eHealth literacy. Int J Environ Res Public Health. 2021;18(24). https://doi.org/10.3390/ijerph182413240.
Dong Y, Qin W, Xu L, Zhang J, Gao Z, Hu F, et al. E-health literacy and its influencing factors among residents aged 15 years and above in Tai′an city. Chin J Public Health. 2021;37(09):1319–22.
Xie T, Zhang N, Mao Y, Zhu B. How to predict the electronic health literacy of Chinese primary and secondary school students?: establishment of a model and web nomograms. BMC Public Health. 2022;22(1):1048. https://doi.org/10.1186/s12889-022-13421-4.
Zhang Z, Ren H, Ping Z, Guo Y. Status and influencing factors of e Health literacy in stroke patients. Chin Gen Pract. 2021;24(22):2850–4+65.
Xie C, Li S, Hu J. Association of e-health literacy and social support with depressive symptoms among female nursing students. Chin J School Health. 2020;41(05):716–9. https://doi.org/10.16835/j.cnki.1000-9817.2020.05.022.
Author information
Authors and Affiliations
Contributions
YZ searched the literature and drafted the manuscript; PRX participated in literature screening and quality assessment; SQN, Shantanu Baral, and LJX edited the manuscript and helped screening of the literature; DRW provided theoretical support and revisions. The final manuscript was reviewed and approved by all the authors.
Corresponding author
Ethics declarations
Ethics approval
Any of the writers did not conduct any studies with human participants or animals for this publication.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zhang, Y., Xu, P., Sun, Q. et al. Factors influencing the e-health literacy in cancer patients: a systematic review. J Cancer Surviv 17, 425–440 (2023). https://doi.org/10.1007/s11764-022-01260-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11764-022-01260-6