
Abstract
Purpose
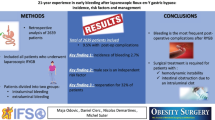
Roux-en-Y gastric bypass is a common bariatric procedure. Its configuration creates an excluded gastric remnant, which is subject to potential acute complications such as bleeding, perforation, and necrosis.
Material and Methods
A retrospective analysis of a prospective database including all patients presenting between 2007 and 2019 to our institution with acute gastric remnant complications after RYGB was performed.
Results
Seven patients were included, including 3 hemorrhages, two of which were treated with double-balloon enteroscopy, as well as 3 perforations and 1 necrosis, all of which required emergent surgery. Overall gastric remnant complication rate was 0.3% in this series.
Conclusion
Acute gastric remnant complications after RYGB are infrequent, but their diagnosis and management can be challenging. Double-balloon enteroscopy has diagnostic and therapeutic value for selected patients. Emergent surgery remains the standard of care for unstable patients and should not be delayed.

Similar content being viewed by others


References
NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. 2017;390(10113):2627–42.
Buchwald H, Consensus Conference Panel. Consensus conference statement bariatric surgery for morbid obesity: health implications for patients, health professionals, and third-party payers. Surg Obes Relat Dis. 2005;1(3):371–81.
American Society for Metabolic and Bariatric Surgery (ASMBS) estimate of bariatric surgery numbers 2011–2017, available at https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers.
Mala T. The gastric remnant in Roux-en-Y gastric bypass: challenges and possibilities. J Clin Gastroenterol. 2016;50(7):527–31.
Heneghan HM, Meron-Eldar S, Yenumula P, et al. Incidence and management of bleeding complications after gastric bypass surgery in the morbidly obese. Surg Obes Relat Dis. 2012;8(6):729–35.
Cave DR. Obscure gastrointestinal bleeding: the role of the tagged red blood cell scan, enteroscopy, and capsule endoscopy. Clin Gastroenterol Hepatol. 3:959–63.
Mehdizadeh S, Ross A, Gerson L, et al. What is the learning curve associated with double-balloon enteroscopy? Technical details and early experience in 6 U.S. tertiary care centers. Gastrointest Endosc. 2006;64(5):740–50.
Kitamura RK, Lee J, Katz LB. The management of GI bleeding after gastric bypass surgery. Int J Surg Res Pract. 2015;2:026.
Roberts KE, Panait L, Duffy AJ, et al. Laparoscopic-assisted transgastric endoscopy: current indications and future implications. JSLS. 2008;12(1):30–6.
Tornese S, Aiolfi A, Bonitta G, et al. Remnant gastric cancer after Roux-en-Y gastric bypass: narrative review of the literature. Obes Surg. 2019;29(8):2609–13.
Ohira M, Toyokawa T, Sakurai K, et al. Current status in remnant gastric cancer after distal gastrectomy. World J Gastroenterol. 2016;22(8):2424–33.
ASGE STANDARDS OF PRACTICE COMMITTEE, Evans JA, Muthusamy VR, et al. The role of endoscopy in the bariatric surgery patient. Surg Obes Relat Dis. 2015;11(3):507–17.
Sauerland S, Angrisani L, Belachew M, et al. Obesity surgery: evidence-based guidelines of the European Association for Endoscopic Surgery (EAES). Surg Endosc. 2005;19(2):200–21.
Raghavendra RS, Kini D. Benign, premalignant, and malignant lesions encountered in bariatric surgery. JSLS. 2012;16(3):360–72.
Watkins BJ, Blackmun S, Kuehner ME. Gastric adenocarcinoma after Roux-en-Y gastric bypass: access and evaluation of excluded stomach. Surg Obes Relat Dis. 2007;3:644–7.
Loewen M, Giovanni J, Barba C. Screening endoscopy before bariatric surgery: a series of 448 patients. Surg Obes Relat Dis. 2008;4:709–12.
Peromaa-Haavisto P, Victorzon M. Is routine preoperative upper GI endoscopy needed prior to gastric bypass? Obes Surg. 2013;23:736–9.
de Moura Almeida A, Cotrim HP, Santos AS, et al. Preoperative upper gastrointestinal endoscopy in obese patients undergoing bariatric surgery: is it necessary? Surg Obes Relat Dis. 2008;4:144–9.
Corsini DA, Simoneti CA, Moreira G, et al. Cancer in the excluded stomach 4 years after gastric bypass. Obes Surg. 2006;16:932–4.
Hu X, Tian DY, Cao L, et al. Progression and prognosis of gastric stump cancer. J Surg Oncol. 2009;100(6):472–6.
Lee SB, Kim JH, Kim DH, et al. Clinicopathological characteristics and prognosis of remnant gastric cancer. J Gastric Cancer. 2010;10(4):219–25.
Hata T, Sakata N, Kudoh K, et al. The best surgical approach for perforated gastric cancer: one-stage vs. two-stage gastrectomy. Gastric Cancer. 2014;17(3):578–87.
Kennedy TL. Gastric carcinoma and acute perforation. Br Med J. 1951;2(2):1489–92.
Lehnert T, Buhl K, Dueck M, et al. Two-stage radical gastrectomy for perforated gastric cancer. Eur J Surg Oncol. 2000;26(8):780–4.
Yuu K, Kawashima H, Toyoda S, et al. Perforated carcinoma in the gastric remnant: a case of conservative treatment prior to successful curative R0 resection. Case Rep Surg. 2016;2016:4091952.
Tey J, Soon YY, Koh WY, et al. Palliative radiotherapy for gastric cancer: a systematic review and meta-analysis. Oncotarget. 2017;8(15):25797–805.
Satoh K, Yoshino J, Akamatsu T, et al. Evidence-based clinical practice guidelines for peptic ulcer disease 2015. J Gastroenterol. 2016;51(3):177–94.
Cho M, Kaidar-Person O, Szomstein S, et al. Laparoscopic remnant gastrectomy: a novel approach to gastrogastric fistula after Roux-en-Y gastric bypass for morbid obesity. J Am Coll Surg. 2007;204(4):617–24.
Voellinger DC, Inabnet WB. Laparoscopic Roux-en-Y gastric bypass with remnant gastrectomy for focal intestinal metaplasia of the gastric antrum. Obes Surg. 2002;12(5):695–8.
Greenstein AJ, O’Rourke RW. Abdominal pain after gastric bypass: suspects and solutions. Am J Surg. 2011;201(6):819–27.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Pouya Iranmanesh, MD – no conflict of interest.
Naveen V. Manisundaran, MD – no conflict of interest.
Kulvinder S. Bajwa, MD – no conflict of interest.
Nirav C. Thosani, MD – no conflict of interest.
Melissa M. Felinski, DO – no conflict of interest.
Erik B. Wilson, MD – Teaching honoraria from Intuitive Surgical, Olympus, Gore, Apollo, and Ethicon.
Shinil K. Shah, DO – Honoraria from Gore and C-SATS; Research grant funding from Medigus and Intuitive Surgical (these grants were not used in any way during this study).
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Iranmanesh, P., Manisundaran, N.V., Bajwa, K.S. et al. Management of Acute Gastric Remnant Complications After Roux-en-Y Gastric Bypass: a Single-Center Case Series. OBES SURG 30, 2637–2641 (2020). https://doi.org/10.1007/s11695-020-04537-w
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-020-04537-w