
Abstract
Background
Hypothermia is associated with an increased postoperative morbidity and mortality. Forced-air warming systems are the most effective methods for its prevention. When using a mattress, a reduction in the area of diffusion of warm air by crushing due to excess weight cannot be ruled out.
Methods
We designed a prospective study to compare the efficacy of a forced-air warming mattress (Bair Hugger® 585) to prevent hypothermia (core temperature (CT°) < 36 °C) in morbidly obese (group MO, body mass index (BMI) ≥ 40 kg/m2) and non-obese patients (group NO, BMI < 30 kg/m2).
Results
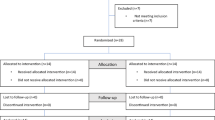
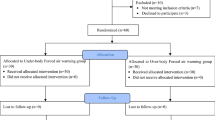
Twenty-six patients were included in group MO (84% bariatric surgery, 96% laparoscopic procedures) and 32 in group NO (37.5% cholecystectomy, 62.5% laparoscopic procedures). The incidence of hypothermia was not different between the two groups 1 h after induction (H1) and at extubation: 22 vs 19% (not significant (NS)) and 23 vs 19% (NS) for the group MO versus group NO. At H1, the mean CT° was not different: 36.3 ± 0.4 °C vs 36.4 ± 0.5 °C (NS), group MO versus group NO. No patient presented severe hypothermia (CT° < 34.9 °C). Dysfunction of the forced-air warming mattress was observed for eight patients (31%) in group MO but for none in group NO.
Conclusion
The forced-air warming mattress is effective in preventing hypothermia in MO patients. However, excess weight is associated with frequent dysfunction of the system, which does not make it a practical system in a context of MO.


Similar content being viewed by others

References
Vaughan MS, Vaughan RW, Cork RC. Postoperative hypothermia in adults: relationship of age, anesthesia, and shivering to rewarming. Anesth Analg. 1981;60(10):746–51.
Reynolds L, Beckmann J, Kurz A. Perioperative complications of hypothermia. Best Pract Res Clin Anaesthesiol. 2008;22(4):645–57. https://doi.org/10.1016/j.bpa.2008.07.005.
Mason DS, Sapala JA, Wood MH, et al. Influence of a forced air warming system on morbidly obese patients undergoing Roux-en-Y gastric bypass. Obes Surg. 1998;8(4):453–60. https://doi.org/10.1381/096089298765554359.
Sessler DI. Perioperative heat balance. Anesthesiology. 2000;92(2):578–96. https://doi.org/10.1097/00000542-200002000-00042.
Hart SR, Bordes B, Hart J, et al. Unintended perioperative hypothermia. Ochsner J. 2011;11(3):259–70.
Sun Z, Honar H, Sessler DI, et al. Intraoperative core temperature patterns, transfusion requirement, and hospital duration in patients warmed with forced air. Anesthesiology. 2015;122(2):276–85. https://doi.org/10.1097/ALN.0000000000000551.
Welch TC. AANA journal course. Update for nurse anesthetists. A common sense approach to hypothermia. AANA Journal. 2002;70(3):227–31.
Karayan J, Thomas D, Lacoste L, et al. Delayed forced air warming prevents hypothermia during abdominal aortic surgery. Br J Anaesth. 1996;76(3):459–60. https://doi.org/10.1093/bja/76.3.459.
Savastano DM, Gorbach AM, Eden HS, et al. Adiposity and human regional body temperature. Am J Clin Nutr. 2009;90(5):1124–31. https://doi.org/10.3945/ajcn.2009.27567.
Nguyen NT, Fleming NW, Singh A, et al. Evaluation of core temperature during laparoscopic and open gastric bypass. Obes Surg. 2001;11(5):570–5. https://doi.org/10.1381/09608920160557039.
Bamgbade OA. Perioperative temperature management in day-case surgical patients. Eur J Anaesthesiol. 2012;29(7):354–5. https://doi.org/10.1097/EJA.0b013e32835132df.
Smith CE, Desai R, Glorioso V, et al. Preventing hypothermia: convective and intravenous fluid warming versus convective warming alone. J Clin Anesth. 1998;10(5):380–5. https://doi.org/10.1016/S0952-8180(98)00049-X.
Kurz A. Thermal care in the perioperative period. Best Pract Res Clin Anaesthesiol. 2008;22(1):39–62. https://doi.org/10.1016/j.bpa.2007.10.004.
Ohtsuka N, Yamakage M, Chen X, et al. Evaluation of four techniques of warming intravenous fluids. J Anesth. 2002;16(2):145–9. https://doi.org/10.1007/s005400200010.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by the ethics committee of the Hôpitaux Universitaires Paris Nord Val de Seine (HUPNVS), Paris 7 University (Institutional Review Board reference 13-001). Informed consent was obtained for all individual participants included in the study.
Conflict of Interest
The authors declare that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Okoué, R., Calabrese, D., Nzé, P. et al. Efficacy of Forced-Air Warming to Prevent Perioperative Hypothermia in Morbidly-Obese Versus Non-obese Patients. OBES SURG 28, 1955–1959 (2018). https://doi.org/10.1007/s11695-017-3108-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-017-3108-5