
Abstract
Summary
This study assessed all fractures occurring in pregnancy at a tertiary referral centre over a 17-year period. Most fractures were due to minimal trauma, and those involving the ankle were the most common. Women tended to fracture during their second and third trimesters and most required surgical intervention during pregnancy.
Purpose
To characterise fractures in pregnancy over a 17-year period at a tertiary referral health service.
Methods
Medical records at the Monash Health in Australia were examined from 2000–2016 for fractures in pregnancy using the birthing outcome system database and the tenth revision of the International Statistical Classification of Diseases and Related Health Problems coding. Site, mechanism, investigations, management and outcomes were documented.
Results
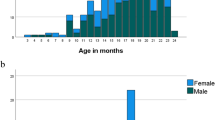
Of the 114,673 live births during this period, 33 women (mean age 30.3 ± 1.9 years) were identified with fracture in pregnancy (~ 2.9 maternal fractures/10,000 live births). Minimal-trauma fractures (MTFs) occurred in 28 women whilst 5 were due to motor vehicle accidents. Of the MTF, 2/28 (7.1%), 13/28 (46.4%) and 13/28 (46.4%) occurred in the first, second and third trimesters, respectively. MTF involved the lower limb (60.7%), upper limb (25.0%), ribs (10.7%) and clavicle (3.6%). The ankle was involved in 39.3% of MTFs. Diabetes (14.3%), asthma (10.7%) and thyroid dysfunction (7.1%) affected these women with MTF; vitamin D levels were not routinely measured. Surgical interventions requiring anaesthesia were required in 57.1% with MTF: 50.0% during their second, 31.3% in their third and 12.5% in their first trimesters; 6.3% had surgery post partum. Pre-term birth and emergency caesarean section complicated 6/28 (21.4%) of MTF pregnancies. One patient received post-partum bisphosphonate therapy; only two 2/32 (6.25%) received medical follow-up.
Conclusions
Fractures in pregnancy are uncommon. Lower limb fractures are frequently due to minimal trauma, and surgical intervention is often required. The low rate of medical follow-up in MTF is of concern and reinforces the need for greater recognition of potential osteoporosis in this population.


Similar content being viewed by others


References
Albright F, Reifenstein EC (1949) The parathyroid glands and metabolic bone disease. Selected studies. Am J Med 7:844
Nordin BE, Roper A (1955) Post-pregnancy osteoporosis: a syndrome? Lancet 268:431–434
Kovacs CS, Ralston SH (2015) Presentation and management of osteoporosis presenting in association with pregnancy or lactation. Osteoporos Int 26(9):2223–2241
Maliha G, Morgan J, Vrahas M (2012) Transient osteoporosis of pregnancy. Injury, Int J Care Injured 43:1237–1241
Cakmak B, Ribeiro AP, Inanir A (2016) Postural balance and the risk of falling during pregnancy. J Matern Fetal Neonatal Med 29(10):1623–1625
McCrory JL, Chambers AJ, Daftary A, Redfern MS (2010) Dynamic postural stability during advancing pregnancy. J Biomech 43:2434–2439
Sanz-Salvador L, Garcia-Perez MA, Tarin JJ, Cano A (2015) Bone metabolic changes during pregnancy: a period of vulnerability to osteoporosis and fracture. Eur J Endocrinol 172(2):R53–R65
More C, Bettembuk P, Bhattoa HP, Balogh A (2001) The effects of pregnancy and lactation on bone mineral density. Osteoporos Int 12(9):732–737
Chatterjee S, Kotelchuck M, Sambamoorthi U (2008) Prevalence of chronic illness in pregnancy, access to care, and health care costs: implications for interconception care. Womens Health Issues 18(6):107–116
Mendez-Figueroa H, Dahlke JD, Vrees RA, Rouse DJ (2013) Trauma in pregnancy: an updated systematic review. Am J Obstet Gynecol 209(1):1–10
Hadji P, Boekhoff J, Hahn M, Hellmeyer L, Hars O, Kyvernitakis I (2017) Pregnancy-associated osteoporosis: a case-control study. Osteoporos Int 28(4):1393–1399
Kovacs C (2016) Maternal mineral and bone metabolism during pregnancy, lactation and post-weaning recovery. Physiol Rev 96(2):449–547
Schiff MA (2008) Pregnancy outcomes following hospitalisation for a fall in Washington state from 1987–2004. BJOG 115:1648–1654
Cannada LK, Pan P, Casey BM, McIntire DD, Shafi S, Leveno KJ (2010) Pregnancy outcomes after orthopedic trauma. J Trauma 69:694–698
Dunning K, LeMasters G, Bhattacharya A (2010) A major public health issue: the high incidence of falls during pregnancy. Matern Child Health J 14:720–725
Eastell R, Reid DM, Compston J, Cooper C, Fogelman I, Francis RM, Hay SM, Hosking DJ, Purdie DW, Ralston SH, Reeve J, Russell RGG, Stevenson JC (2001) Secondary prevention of osteoporosis: when should a non-vertebral fracture be a trigger for action? Q J Med 94:575–597
Pritchard JM, Giangregorio LM, Ioannidis G, Papaioannou A, Adachi JD, Leslie WD (2012) Ankle fractures do not predict osteoporotic fractures in women with or without fractures. Osteoporos Int 23:957–962
Biver E, Durosier C, Chevalley T, Hermann FR, Ferrari S, Rizzoli R (2015) Prior ankle fractures in postmenopausal women are associated with low areal bone mineral density and bone microstructure alterations. Osteoporos Int 26:2147–2155
Stein EM, Liu XS, Nickolas TL, Cohen A, Thomas V, McMahon DJ, Zhang C, Cosman F, Nieves J, Greisberg J, Guo XE, Shane E (2011) Abnormal microarchitecture and stiffness in postmenopausal women with ankle fractures. J Clin Endocrinol Metabol 96(7):2041–2048
Shahtaheri SM, Aaron JE, Johnson DR, Purdie DW (1999) Changes in trabecular bone architecture in women during pregnancy. Br J Obstet Gynaecol 106(5):432–438
Wisser J, Florio I, Neff M, Konig V, Huch R, Huch A, Mandach UV (2005) Changes in bone density and metabolism in pregnancy. Acta Obstet Gynecol Scand 84:349–354
Ulrich U, Miller PB, Eyre DR, Chesnut CH, Schlebusch H, Soues MR (2003) Bone remodelling and bone mineral density during pregnancy. Arch Gynecol Obstet 268:309–316
Styczynska H, Lis K, Sobanska I, Pater A, Pollak J, Mankowska A (2009) Bone turnover markers and osteoprotegerin in uncomplicated pregnancy. Electron J Int Fed Clin Chem Lab Med 19(4):193–202
Dieguez M, Herrero A, Avello N, Suarez P, Delgado E, Menendez E (2016) Prevalence of thyroid dysfunction in women in early pregnancy: does it increase with maternal age? Clin Endocrinol 84(1):121–126
Negro R, H MJ (2011) Thyroid disease in pregnancy. Best Pract Res Clin Endocrinol Metab 25(6):927–943
Walsh JP (2016) Managing thyroid disease in general practice. Med J Aust 205(4):179–184
World Health Organization (2016) Diabetes country profiles 2016—Australia, Geneva
Australian Bureau of Statistics (2015) National health survey: first results, 2014–15. Cat. No. 4363.0.55.001;. ABS, Canberra
Templeton M, Pieris-Caldwell I (2008) Gestational diabetes mellitus in Australia, 2005-06. Cat. no. CVD 44. Australian Institute of Health and Welfare
Australian Institute of Health and Welfare (2016) Australia’s mothers and babies 2014: in brief. Perinatal statistics series no. 32 Cat no. PER 87. AIHW, Canberra
Greenfield DM, Eastell R (2001) Risk factors for ankle fracture. Osteoporos Int 12:97–103
Baldwin EA, Borowski KS, Brost BC, Rose CH (2015) Antepartum nonobstetrical surgery at >/= 23 weeks’ gestation and risk for preterm delivery. Am J Obstet Gynecol 212(232):e1–e5
Bhattee G, Rahman MS, Rahman J (2009) Open reduction and internal fixation of an acetabular fracture in pregnancy: a case report. Curr Orthop Pract 20(3):329–330
American College of Obstetricians and Gynecologists (2017) Nonobstetric surgery during pregnancy. Committee Opinion No. 696. Obstet Gynecol 129:777–778
Phillips AJ, Ostlere SJ, Smith R (2000) Pregnancy-associated osteoporosis: does the skeleton recover? Osteoporos Int 11:449–454
Salles JP (2016) Bone metabolism during pregnancy. Ann Endocrinol 77:163–168
Pediatrics AAo (2012) Breastfeeding and the use of human milk. Pediatrics 129(3):e827–e841
Patlas N, Golomb G, Yaffe P, Pinto T, Breuer E, Ornoy A (1999) Transplacental effects of bisphosphonates on fetal skeletal ossification and mineralization in rats. Teratology 60:68–73
Funding
A.T. is supported by a Royal Australasian College of Physicians/Osteoporosis Australia research grant. F.M. and P.W. are supported by an Osteoporosis Australia/Australia and New Zealand Bone and Mineral Society clinical grant. Hudson Institute is supported by the Victorian government’s Operational Infrastructure Support program.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval was obtained from the Monash Health Human Research Ethics Committee.
Statement of human and animal rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. For this type of study, formal consent is not required.
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Herath, M., Wong, P., Trinh, A. et al. Minimal-trauma ankle fractures predominate during pregnancy: a 17-year retrospective study. Arch Osteoporos 12, 86 (2017). https://doi.org/10.1007/s11657-017-0380-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-017-0380-x