
Abstract
Background
Surgical treatment of early rectal cancer T1 is either local excision or total mesorectal excision. The choice of surgery is based on the risk of metastatic lymph node involvement. The most important factor to consider is the degree of submucosal invasion. We present a different way to measure tumoral invasion derived from the measurement of the healthy residual submucosa with its prognosis and therapeutic implications
Methods
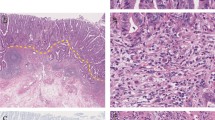
Observational study of tumor submucosal invasion in patients undergoing transanal endoscopic microsurgery was conducted. Parameters evaluated are submucosal invasion, measuring the healthy residual submucosa at the point of maximum invasion; macroscopic morphology of the tumor; presence of muscularis mucosa, muscularis propria, and measurement of submucosa in the tumor area and the healthy area. The classification proposed is compared with the ones previously published.
Results
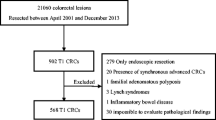
Eighty consecutive patients diagnosed with T1 rectal cancer underwent transanal endoscopic microsurgery. Seventeen tumors (21.3%) were polypoid. En bloc resection was achieved in 77 (96.3%). The muscularis mucosa was present in 28 (35%), and the muscularis propria in 77 (96.3%) (p < 0.001). The healthy residual submucosa in the tumor area measured 2,343 ± 1,869 μm. Agreement was moderate with the Kikuchi classification (kappa 0.58) and very good with the Kudo classification (kappa 0.87).
Conclusions
We describe a method for measuring submucosal invasion in T1 rectal cancer which does not depend on the morphology of the lesion or on the presence of the muscularis mucosa. It can be applied to all T1 classifications of the digestive tract in which the muscularis propria is present.



Similar content being viewed by others

References
Morson BC, Whiteway JE, Jones EA, et al. Histopathology and prognosis of malignant colorectal polyps treated by endoscopic polypectomy. Gut 1984; 25:437-44
Kikuchi R, Takano M, Takagi K, , et al. Management of early invasive colorectal cancer. Risk of recurrence and clinical guidelines. Dis Colon Rectum 1995; 38:1286-95.
Kitajima K, Fujimori T, Fujii S, et al. Correlations between lymph node metastasis and depth of submucosal invasion in submucosal invasive colorectal carcinoma: a Japanese collaborative study. J Gastroenterol 2004; 39:534-43.
Haggitt RC, Glotzbach RE, Soffer EE, Wruble LD. Prognostic factors in colorectal carcinomas arising in adenomas: implications for lesions removed by endoscopic polypectomy. Gastroenterology 198; 89:328-36.
Ueno H, Mochizuki H, Hashiguchi Y, et al. Risk factors for an adverse outcome in early invasive colorectal carcinoma. Gastroenterology 2004; 127:385-94..
Buess G, Theiss R, Günther M, et al. Transanal endoscopic microsurgery. Leber Magen Darm 1985; 15:271-9
Borschitz T, Gockel I, Kiesslich R, Junginger T. Oncological outcome after local excision of rectal carcinomas. Ann Surg Oncol 2008; 15:3101-8.
Toh EW, Brown P, Morris E, et al. Area of submucosal invasion and width of invasion predicts lymph node metastasis in pT1 colorectal cancers. Dis Colon Rectum 2015; 58:393-400.
Serra-Aracil X, Mora-Lopez L, Alcantara-Moral M, , et al. Transanal endoscopic surgery in rectal cancer. World J Gastroenterol 2014; 20:11538-45
Edge SB, Compton CC. The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010; 17:1471-4.
Rocha JJ, Feres O. Transanal endoscopic operation: a new proposal. Acta Cir Bras 2008;23(Suppl 1):93–104.
Kudo S. Endoscopic mucosal resection of flat and depressed types of early colorectal cancer. Endoscopy 1993; 25:455-61
Minamoto T, Mai M, Ogino T, et al. Early invasive colorectal carcinomas metastatic to the lymph node with attention to their nonpolypoid development. Am J Gastroenterol 1993; 88:1035-9.
Stornes T, Wibe A, Nesbakken A, et al. National Early Rectal Cancer Treatment Revisited. Dis Colon Rectum 2016;59:623-9
Debove C, Svrcek M, Dumont S, et al. Is the assessment of submucosal invasion still useful in the management of early rectal cancer? A study of 91 consecutive patients. Colorectal Dis 2017;19:27-37
Acknowledgements
We thank the rest of the members of the Coloproctology Unit for applying the study protocol. We thank Cristina Gomez Vigo for correcting the manuscript and Michael Maudsley for helping with the English.
Author information
Authors and Affiliations
Contributions
-Study conception and design: Alex Casalots, Xavier Serra-Aracil, Laura Mora-Lopez
-Acquisition of data: Alex Casalots, Xavier Serra-Aracil, Laura Mora-Lopez, Albert Albert Garcia-Nalda, Carles Pericay, Joan Carles Ferreres, Salvador Navarro-Soto
-Analysis and interpretation of data: Alex Casalots, Xavier Serra-Aracil, Laura Mora-Lopez, Albert Albert Garcia-Nalda, Carles Pericay, Joan Carles Ferreres, Salvador Navarro-Soto
-Drafting of manuscript: Alex Casalots, Xavier Serra-Aracil, Laura Mora-Lopez, Albert Albert Garcia-Nalda, Carles Pericay, Joan Carles Ferreres, Salvador Navarro-Soto
-Critical revision: Alex Casalots, Xavier Serra-Aracil, Laura Mora-Lopez, Albert Albert Garcia-Nalda, Carles Pericay, Joan Carles Ferreres, Salvador Navarro-Soto
Corresponding author
Additional information
The study has not been presented previously in any form.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Casalots, A., Serra-Aracil, X., Mora-Lopez, L. et al. T1 Rectal Adenocarcinoma: a Different Way to Measure Tumoral Invasion Based on the Healthy Residual Submucosa with Its Prognosis and Therapeutic Implications. J Gastrointest Surg 25, 2660–2667 (2021). https://doi.org/10.1007/s11605-021-04948-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-021-04948-9