
Abstract
Health and convenience are two indispensable indicators of the society promotion. Nowadays, to improve community health levels, the comfort of patients and those in need of health services has received much attention. Providing Home Health Care (HHC) services is one of the critical issues of health care to improve the patient convenience. However, manual nurse planning which is still performed in many HHC institutes results in a waste of time, cost, and ultimately lower efficiency. In this research, a multi-objective mixed-integer model is presented for home health care planning so that in addition to focusing on the financial goals of the institution, other objectives that can help increase productivity and quality of services are highlighted. Therefore, four different objectives of the total cost, environmental emission, workload balance, and service quality are addressed. Taking into account medical staff with different service levels, and the preferences of patients in selecting a service level, as well as different vehicle types, are other aspects discussed in this model. The epsilon-constraint method is implemented in CPLEX to solve small-size instances. Moreover, a Multi-Objective Variable Neighborhood Search (MOVNS) composed of nine local neighborhood moves is developed to solve the practical-size instances. The results of the MOVNS are compared with the epsilon-constraint method, and the strengths and weaknesses of the proposed algorithm are demonstrated by a comprehensive sensitivity analysis. To show the applicability of the algorithm, a real example is designed based on a case study, and the results of the algorithm over real data are evaluated.
Similar content being viewed by others

1 Introduction
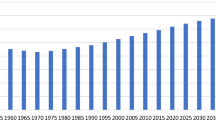
Nowadays, lower birth rates and increased life expectancy have led to an increase in the number of patients needing medical care. For example, in the EU countries, the share of people older than 60 has grown from 17 to 22% and is expected to reach 32% by 2030 [6]. Increasing population and increasing levels of expectation of patient to receive health care have led to increased demand for home health services. Moreover, high costs of hospitalization, stressful environment, access and traffic problems, various requirements of patients in need of medical care, specialized and sensitive patient care, and low-quality services at hospitals, have brought patients and needy people to home health care [17]. As a consequence, in the year 2011, more than 4.7 million patients in the United States received home health services, and in Europe, between 1 and 5% of the total public health budget is allocated to HHC services [20]. On top of that, the covid-19 pandemic during the past year showed us avoiding to visit hospitals for many non-emergency medical problems becomes a necessity [50]. Because of the lack of equipment, the number of specialized hospitals which operate as coordinators of the overall therapy process is limited [32]. Health centers are considered very strategic and critical and the smallest disruption may cause severe crises [24]. Therefore, home health care is a good alternative to hospital, residential, or institutional nursing care, and its main purpose is to improve the quality of life for clients while reducing costs. HHC offers a wide range of services, social, medico-social, and medical services such as cleaning, cooking, shopping, hygiene assistance, nursing, and the like [22]. Given the full range of operational constraints, HHC planners first, assign nurses to each patient and then, route plan and schedule nurses to visit their assigned patients. Many practical considerations need to be taken into account when generating such a plan. For instance, nurses may have different skill levels; Patients may have different preferences in terms of cost or service level; Various vehicle types with different speeds, costs, and emissions can be used to visit patients [26]. Routing decisions will have a considerable impact on the quality of a HHC plan. For example, a survey on the working time of HHC nurses in Norway has shown that between 18 and 26% of the total working time of nurses are the driving time of which 22% is because the driving directions for nurses are not optimal [20]. Such results indicate the high potential of the HHC problem in routing and scheduling optimization to improve services.
In this paper, we study the home health care scheduling and routing problem in a practical context. At the beginning of the day, the list of patients is known together with their associated time windows and priorities in receiving services from a medical staff with a specific skill level. We consider a real situation in which, an unlimited number of nurses with different service levels are available. This situation happens in an HHC company when, a relatively high number of medical staff with various backgrounds are registered, and each day a limited number of them are selected and assigned to requested services by patients.
Vehicle types with different levels of cost, speed, and emissions may be used by medical staff. The primary purpose of the problem is to allocate patients to medical staff and to find a plan for each medical staff in which the assigned patients are visited exactly once during their provided time window. Given the importance of cost reductions for the HHC institute, the main objective is to reduce the total costs, including the cost of assigning medical staff to patients, and their travel costs. Nowadays, transportation is recognized as the largest source of pollution in a logistics and supply chain system [55], and, today’s society has paid particular attention to reduce environmental pollution. Therefore in this research, reducing the amount of emission generated by vehicles is also considered as an objective function. The third objective in this work is minimizing the maximum workload assigned to each medical staff aiming at a balanced workload schedule. The last objective is maximizing the service quality provided to patients, in terms of assigning medical staffs with higher level of services.
The problem is first mathematically modeled as a mixed-integer linear problem. Then, two solution methods are implemented, namely the epsilon-constraint and the Multi-Objective Variable Neighborhood Search meta-heuristic (MOVNS). The results obtained from these two methods are compared and analyzed in terms of efficiency which shows the reasonable performance of the proposed MOVNS. Moreover, to prove the usability of the method in the real-world situation, a real example from a home health service provider in Tehran (Tavan Salamat institute), is investigated as a case study.
The main contributions of this research can be summarized as follows.
-
Introducing a multi-objective HHC with four important objectives: Min total costs, Min \(\mathrm{{CO}}_2\) emission, Min-Max workload (to balance the workload), and Max service quality.
-
Providing a multi-objective mixed-integer linear model and an epsilon-constraint method to solve smaller instances of the problem.
-
Developing a multi-objective variable neighborhood meta-heuristic composed of nine specifically designed local moves that consider improving all objectives of the problem.
-
Evaluating the proposed method over a real data set from a case study of a HHC institute and performing a comprehensive sensitivity analysis.
In the remainder of this paper, Sect. 2 presents the literature review on the single period HHC. Section 3 describes the problem details and formulation. Section 4 defines our MOVNS solution approach. Section 5 shows the computational results and sensitivity analysis. Section 6 discusses a real example from the case of Tavan Salamat HHC institute to validate the performance of the proposed MOVNS. Finally, conclusions are presented in Sect. 7.
2 Literature review
Different problems with various assumptions have been studied in the literature of the HHC [1, 46]. These problems are generally considered the planning, scheduling, and routing of healthcare staff when visiting patients at their homes. In the literature, HHC problems are categorized based on their planning horizon as the single-period or the multi-period HHC [8]. Because of the complexity of the HHC problems in practice, most of the research papers in this field focus on single-period optimization problems [14].
The main assumptions for routing and scheduling home health services are first reviewed by Fernandez et al. [18]. These authors explore how different nurses were assigned to patients, in specific time slots, and according to the number of services. A robust estimation method is considered to solve the problem and a case study is conducted in the UK. The HHC is extended by Hindle et al. [29, 30] considering resource allocation and reducing travel costs. Trautsamwieser et al. [52] present a HHC problem where mandatory working and rest times of nurses are added to general assumptions of the problem. They minimize the summation of driving times, waiting times, and overtime of the nurses. Unfulfilled preferences, soft time windows, and the number of jobs serviced by an overqualified nurse are also seen in their model. They propose a variable neighborhood search to solve numerical examples derived from real-life data from three districts in Upper Austria. Allaoua et al. [2] classify patients according to the needed service type. The objective consists of constructing optimal routes and rosters for the health care staffs. They propose a matheuristic that combines the solution of a set partitioning problem and a multi-depot traveling salesman problem with time windows. Mankowska et al. [39] study the nurse allocation and routing using a clustering concept. Patients are divided into two groups based on the number and the concurrency of required nurses. Then, the nurse allocation is performed for each cluster. A mathematical model is proposed together with a powerful heuristic based on a sophisticated solution representation. Stochastic service time was considered by Yuan et al. [53]. A stochastic programming model is proposed to formulate the problem. In their model, next to the costs, the expected penalty for late arrival at customers is minimized. Shi et al. [46] present the uncertainty of the demand for the number of needed drugs as fuzzy values. They minimize the transportation cost as the objective function of the problem. A hybrid GA is proposed to address the benchmark instances of the VRP with a time window. Erdem and Koç [15] develop a HHC routing problem in which electric vehicles are used by medical staff. The objective is to minimize the total travel time. Multiple depots, heterogeneous fleet, and time windows are the main assumptions in their problem. A hybrid meta-heuristic that combines a genetic algorithm and a variable neighborhood descent is proposed by them. Osorio Mora et al. [43] introduce a variant of the cumulative vehicle routing problem for HHC logistics. In their version of the VRP the delayed latency is optimized. Delayed latency corresponds to caregivers’ total overtime hours work while visiting patients. Multiple non-fixed depots and emergency trips from patients to the closest depot are included. A new MILP model is presented and solved using commercial solvers. Demirbilek et al [11] proposed a new heuristic to maximize patient visits for a set of nurses during the planned horizon, and for several scenarios. In their study, they have re-planned the current schedules of nurses according to the new request under consideration as well as future requests. The results proved that their approach achieves significantly higher average daily visits and shorter travel times compared to the greedy method. Nasir and Kuo [41] develop a mathematical model for home health care problem with simultaneous synchronization of vehicle routing and staff scheduling. They propose a framework in which the requirements of HHC services are captured. In their framework, synchronization between HHC staff and Home Delivery Vehicles, multiple visits to patients, multiple routes of HDVs, and pickup/delivery visits related precedence for HDVs are taken into account. A Hybrid Genetic Algorithm is proposed to solve instances of the problem. They apply their model and solution method to real-life instances in the central and western districts of Hong Kong.
For a more sophisticated review of single-period HHC, one may refer to the survey by Fikar and Hirsch [20]. In the remainder of this section, we briefly review the literature based on the most relevant features to the current study, including the work balance, multiple transportation modes, and multi-objective HHCs.
Workload balance Due to its importance in practice, workload balance is studied in several papers. Bredström and Rönnqvist [7] present a mathematical model for the vehicle routing and scheduling problem with time windows, and pairwise temporal precedence between customer visits. They also study propounded decisions in which several nurses were simultaneously employed to perform a service and the situation where the nurse must visit the patient at a specific time for a particular task. The objective is to minimize the summation of traveling distances and the maximal deviation in the workload of staff members. Mutingi and Mbohwa [40] develop fuzzy evaluation techniques to schedule nurses within an evolutionary framework. They develop an interactive decision support tool for constructing home health caregivers schedules, while minimizing the violation of time windows, maximizing workload balance amongst the caregivers, and maximizing the grouping efficiency. They measured the workload as the sum of travel times and duration of visits to the set of patients assigned to each nurse. To balance the workload, the sum of deviation of each nurse workload from the average workload is minimized. Lanzarone and Matta [35] derives an analytical structural method for solving the nurse assignment problem. This method accounts for randomness related to both the demands from patients already assigned and the demands from new patients. The main objectives are to minimize the waiting time and to optimize the workload balance. They assume stochastic demands from patients and multiple skill levels for nurses. The workload objective is the minimization of the maximum assigned workload which leads to reduce nurses’ overtime. Nasir et al. [42] study the development of the HHC service system in terms of long-time economic sustainability as well as operational efficiency. The objective is to minimize the total travel cost. Time window constraints, specific contract duration, resting time, and workload balance are among the constraints of this problem. A maximum workload limit is imposed for health care workers and the capacity of the health care office. An integrated planning approach among various types of health care services is modeled and solved using CPLEX. Decerle et al. [10] minimize the total traveling time of the caregivers, deviation from preferred visit time of patients, the synchronized visits non-respect, and the maximal working time difference among caregivers. The working time of a caregiver is defined as the difference between his/her departure and arrival times from and to the depot. They develop a new hybrid Memetic, and an Ant colony optimization algorithm to solve the HHC problem.
Multi-mode transport In many practical HHCs, it is more realistic to consider multiple transportation modes for nurses. For example, most of the medical staff from the Austrian Red Cross in Vienna use a combination of public transport modes (bus, tram, train, and metro) and walking to visit their assigned patients [44]. Few studies in the literature involve more than one transportation mode in an HHC problem. Hiermann et al. [28] study a real-world multi-modal home healthcare scheduling problem from a major Austrian home-healthcare provider. Their objective is to minimize the travel time and delays and to optimize the allocation of nurses to patients. Customer satisfaction is also seen in their research. Nurses use two modes of transportation (cars or public transportation), which inherently leads to travel times dependent on the chosen modality. A two-stage approach is developed by them, in which initial solutions are generated either via constraint programming or by a random procedure. Then, the initial solutions are improved by applying hyper-heuristic consists of four meta-heuristics, namely, a Variable Neighborhood Search, a Memetic Algorithm, a Scatter Search, and a Simulated Annealing. In a HHC study by Fikar and Hirsch [19], minimizing the travel and waiting time is considered as the objective function of the problem. The possibility of walking, and allowing several time breaks during a nurse trip, are the main assumptions in this problem. Moreover, they assume that nurses are traveling by small buses instead of using personal vehicles. They develop a two-stage math-heuristic which first, identifies potential walking-routes and then, optimizes the transportation system. They perform numerical studies using real-world instances from the Austrian Red Cross. Rest and Hirsch [44] involve public transportation as an additional option for nurses traveling in a HHC. They minimize the total travel and waiting time of nurses as the factors affecting customers and employees satisfaction. Assumptions such as daily periods, different levels of nurses, and hard time windows are considered. They take time-dependent travel times and forced rest times into their study. A Taboo Search is proposed by them as the solution approach. A multi-depot HHC model with multiple types of vehicles is studied by Bahadori-Chinibelagh et al. [5]. Vehicles with different capacity and transportation cost distribute the required medicine to pharmacies and collect biological samples from laboratories. Two heuristic algorithms are developed to solve the problem.
Multi-objective According to practical priorities in a HHC company, multiple objectives may be of interest in different situations. As a result, some research papers in the literature pay attention to find Pareto solutions using multi-objective optimization techniques. Braekers et al. [6] study a bi-objective HHC problem. The first objective is to minimize the transportation and overtime costs of nurses, and the second objective minimizes the dissatisfaction of patients measured by the deviation from the preferred visit time and how disliked the assigned nurses are. To solve the problem, a meta-heuristic algorithm based on the multi-directional local search framework, with a large neighborhood search as a sub-heuristic, is proposed. To assist the green HHC Fathollahi-Fard et al. [17], present a bi-objective optimization for the HHC routing problem with the objectives of reducing total costs and environmental pollution. In their work, estimation of treatment time and amount of medication required for each patient, patient service time window, and multiple vehicle types are discussed. They develop several heuristics and meta-heuristics including a Simulated Annealing, and a Slap Swarm Algorithm to find Pareto solutions. Manavizadeh et al. [38] define a weighted objective function that minimizes the total traveling distance, the total delay, and the number of used staff. They develop a mathematical model and a Simulated Annealing algorithm to solve instances of this problem. In their version of the HHC, interdependent services for patients are allowed. More recently, Khodabandeh et al. [34] develop a bi-objective mathematical model for HHC routing and scheduling problems. The first objective function minimizes the total traveling time of all routes of the nurses, and the second objective function minimizes the downgrading costs of the nurses. Downgrading costs are the difference between the actual and potential skills of the nurses. In fact, nurses with higher skills have to be paid more, and need more expensive equipment, training and nursing certificates. Therefore, downgrading costs can impose high hidden costs to the HHC company. An epsilon-constraint approach is proposed by them, and the applicability of the model in solving various sizes of the problem are discussed.
Research gap It can be seen that for the single-period HHC, various objective functions were studied, including the travel cost, travel time, travel distance, travel emission, workload balance, and, patient satisfaction. Only few works considered the HHC as a multi-objective problem where Pareto solutions are provided to the decision-maker. To have a better overview, the reviewed articles are briefly presented in Table 1.
According to the literature review, home healthcare problems are usually focused on reducing costs. Although environmental concerns are getting more attention in today’s society, very few HHC papers paid attention to this issue [17]. In this paper, a HHC problem derived from a real case, and four main objectives of cost, pollution, workload balance, and service quality are considered in a multi-objective framework. The current study is among the first ones to consider many practical aspects of a HHC problem simultaneously, and as a multi-objective problem. These aspects include patients’ priorities, patients’ time windows, unlimited number of available nurses with different skill levels, multiple types of transportation vehicles (modes), and patients’ priorities on the service level of nurses. Due to the complexity of the problem, most papers proposed meta-heuristic solution approaches, namely the Simulated Annealing, the Slap Swarm, and a hybrid multi-directional local search and large neighborhoods search method. Regarding the solution method, according to Table 1, this is the first study to develop a MOVNS for the multi-objective HHC. The MOVNS has the capability to be used for problems with multiple objectives because of its flexibility in employing several local moves in different variable neighbourhood structures.
3 Problem description
In this section, the home healthcare routing problem introduced in Sect. 1, is described in detail, and is mathematically modeled as a multi-objective mixed-integer nonlinear programming formulation. Then, the classical linearization approach is used to make the model linear.
Consider the graph \(G=(V, A)\) in which \(V\{0\} \cup U\) is the set of nodes representing the patients’ homes (\(U=\{1,2,\ldots ,u\}\)) and the depot (0), and \(A=\{(i,j)\mid i,j\in \text {V},i\ne j\}\) is the set of edges of the graph that represent the travel path between all nodes including location of patients, and the depot.
The main assumptions of our HHC problem are presented as follows.
-
A given number of patients along with their locations and their available time window are known.
-
An unlimited number of nurses with different service levels are available to serve patients. This is a realistic assumption according to the case study, since in practice there are a large number of registered nurses at the HHC provider company.
-
Each patient needs to be visited by exactly one nurse during its associated time window.
-
If a nurse arrives earlier than the opening time of the patient time window, she/he has to wait until the time window starts.
-
An order of patients to be visited by a nurse starting and ending at the depot is called a tour.
-
The location of the company is assumed as the central depot, and due to the technical needs and administrative regulations, each nurse must start and end its visit tour from and to the central depot.
-
Nurses are moving between nodes using a transportation vehicle.
-
Multiple types of transportation vehicles are considered. The travel cost, as well as the emission, varies depending on the type of vehicle.
-
The available number of each vehicle type is considered unlimited. This is due to the fact that different modes of transportation are available including the nurse personal vehicle, and public transportation. Moreover, it is assumed that the company will be always able to provide a transport facility if needed.
-
The Euclidean travel distance between every pair of nodes is calculated according to the location of the depot and patients, and therefore assumed to be symmetric and following the triangular inequality.
-
For each vehicle type, the cost rate, the vehicle speed, and the \(\mathrm{{CO}}_2\) emission rate, are known. Therefore, the travel cost, the travel time, and the travel emission between every pair of nodes for each vehicle type are calculated using these rates and the travel distance matrix.
-
Each nurse tour is accomplished using a single vehicle type (i.e It is not allowed to change the vehicle type during a tour.).
-
Nurses are categorized into multiple types according to their quality of service (service level). This categorization is performed by the company based on different factors of nurse specifications, including their previous experiences, relevant skill levels, and customer satisfaction.
-
Since the level of service correlates with the nurse visit cost, each patient may have specific preferences for choosing a nurse service level. These priorities as well as the technical constraints of the company are assumed to be known when assigning nurses to patients.
3.1 Mathematical formulation
In this section, first the sets, parameters, and decision variables of the model are introduced, and then, the mathematical model of the proposed HHC problem is presented.
-
Sets:
-
V : The set of nodes including patients’ homes and the depot
-
U : The set of nodes corresponding to patients homes
-
N : The set of nurse types
-
P : The set of unlimited number of nurses of each type
-
K : The set of vehicle types
-
Parameters:
-
\(d_{ij}:\) The distance between nodes i and j \(\in V\)
-
\(ot_i:\) The opening time of the time window for patient i
-
\(ct_i:\) The closing time of the time window for patient i
-
\(st_i:\) The service time of patient i
-
\(t_{ijk}:\) The travel time from node i to node j using transport vehicle type k
-
\(c_{ijk}:\) The travel cost from node i to node j using transport vehicle type k
-
\(vc_{n}:\) The visiting cost of a patient by nurse type n for the HHC company
-
\(e_{ijk}:\) The \(\mathrm{{CO}}_2\) emission generated when traveling from node i to node j using transport vehicle type k
-
\(pr_{i,n}:\) A binary parameter which shows if nurse type n is preferred by patient i
-
\(sl_{n}:\) The service level of nurse type n
-
M : A large positive value
-
Decision variables:
-
\(x_{ijnpk}:\) Equals 1 if the nurse p of type n visits node j immediately after node i by transport vehicle type k, and 0 otherwise
-
\(at_{inpk}:\) The arrival time of nurse p of type n at node i when transport vehicle type k is used
-
\(z_{np}:\) The total working time of the nurse p of type n including his/her travel time and service times
-
\(z_{max}:\) An auxiliary variable which shows the maximum value of \(z_{np}\) over all nurses
-
\(w_{inpk}:\) The waiting time of the nurse p of type n before the service time patient i starts
Four objective functions are defined for this problem. The first objective (Eq. 1) is to minimize the cost of assigning nurses to patients and the travel cost of nurses when visiting patients. The second objective (Eq. 2) minimizes the amount of released \(\mathrm{{CO}}_2\) emission generated by traveling between nodes. The third objective function (Eq. 3) minimizes the maximum time spent by each nurse to balance the workload of nurses. Although number of available nurses of each type is not limited, the objective function of workload balance has been considered so that active nurses have acceptable working hours and are satisfied with their working time. This will also prevent too much or too low workload, and consequently increase patients satisfaction. The fourth objective function (Eq. 4) maximizes the service quality by assigning a nurse with a higher service level to each patient. The nurse must be selected from the ones included in the priority list of patient. Equations 5 and 6 determine the depot as the start and the end node of each nurse tour. Equation 7 indicates that each patient is visited exactly once. Equation 8 specifies that at most one nurse with one vehicle type can move from node i to node j. Equation 9 indicates that each nurse can only be assigned to one route of visiting patients. Equation 10 ensures that preferences of patients on the selection of nurses are satisfied. Equations 11 and 12 are flow conservation constraints at the depot and patient locations, respectively. Equation 13 explains the relationship between the arrival times of two visited nodes of i and j if a nurse visits patient j immediately after patient i. This constraint together with the flow constraints ensures the connectivity of each nurse tour. Equations 14 and 15 specify that the service time of each patient has to happen during its corresponding time window. Equation 16 ensures that the start time of the tour for each nurse is set to zero. Equation 17 calculates the working time of each nurse which is used as the workload of the nurse. Equation 18 determine the maximum workload of assigned nurses. This constraint is used to implement the min-max workload balance objective function (Eq. 3). Equations 19 to 22 define the decision variables.
3.2 Model linearization
In the presented model, Eq. 17 contains the nonlinear expression \(w_{inpk}*x_{ijnpk}\) which is a multiplication of a positive continuous variable in an integer variable. To make this expression linear, the auxiliary variable \(w_{ijnpk}^\prime\) is used. Thus, Eq. 17 is changed to Eq. 23, and Eqs. 24 to 26 are added to the main constraints of the problem.
4 Solution strategies
In this section, first, the epsilon-constraint method is implemented to solve the small-size instances of the problem. Next to the epsilon-constraint method, an efficient meta-heuristic is presented to solve larger and real-world instances of the problem. This method is the multi-objective version of the Variable Neighborhood Search method (VNS). The method is based on combining several local moves which systematically explore the solution space, and avoid trapping in a local optimum. Both methods are explained in detail in the following subsections, and their results are compared in Sect. 5.
4.1 Epsilon-constraint
One of the best classical techniques used to solve multi-objective optimization problems is the epsilon-constraint method [23]. In this method, the objective function with highest priority for the decision maker, is selected as the main objective, and other objective functions are added to the set of existing constraints. [16]. According to the literature, minimizing the cost is considered the most important objective for home health care institutions among others. In particular, traveling costs (distance, or time), is a common objective by the provider to minimize incurred costs for home visits. [25] Therefore, the cost minimization is assumed as the main objective in our epsilon-constraint method, and the emission minimization, the max workload minimization, and the service quality maximization are added to the set of constraints as presented in Eq. 27. In the epsilon-constraint method, epsilon values (\(\varepsilon _1,\varepsilon _2,\varepsilon _3\)) are changed iteratively, to obtain the Pareto optimal solutions.
4.2 The multi-objective variable neighborhood search method
The Variable Neighborhood Search (VNS) algorithm works based on alternating the neighborhood search structures and therefore is a suitable method for solving routing and scheduling optimization problems [49]. The VNS considers two main perspectives: how to define a set of pre-established neighborhoods and how to explore the solution space using these neighborhood structures [13]. This method has been successfully used to solve challenging optimization problems [4, 36, 48].
While, the proposed algorithm follows the idea and structure of the MOVND proposed by Duarte et al. [13], it is a different implementation.
The main idea of the presented MOVNS is the systematic application of a set of neighborhood operators to increase the overall identification probability of every Pareto optimal alternative. More specifically, in this research, initial solutions as well as local moves are designed to generate and improve solutions according to the objective functions. Compared with existing concepts of variable neighborhood search, applied operators are categorized based on their main functionality in improving the solution toward one of the objective functions, which means Specific local moves are designed and implemented according to each objective function. Moreover, a special shaking procedure is designed to escape from local optimum. A general overview of the proposed algorithm is depicted in Algorithm 1.
In the initialization part of the algorithm, first in a pre-processing step, nurse types and vehicle types are sorted in five different matrices according to different priorities namely, nurse service level, nurse cost, vehicle speed, vehicle cost, and vehicle emission. Then, three different approaches are used to generate three initial solutions. Having the initial solutions, the iterative improvement phase of the algorithm is composed of three steps. The first iterative step is called the multi-objective shake in which a perturbation strategy is applied to each available solution to diversify the search space. The next step is the Multi-Objective Variable Neighborhood Descent (MOVND) which is composed of four VND structures each contains various local moves corresponding to our four objective functions. As a result of applying the MOVND a number of new solutions are generated to construct the Pareto list. In the last step (MONeighborhoodChange), the current list of Pareto solutions are updated so that finally non-dominated solutions are kept and transferred to the next iteration.

4.2.1 Initialization
to increase the diversity of the solutions in terms of various objective functions, three strategies are used in generating initial solutions. Each strategy runs one time and at most 3 different solutions can be constructed using these strategies. The generated initial solutions are defined as the first Pareto list for the next steps. In the first strategy, the initial solution is generated in a way that vehicles and nurses with a lower cost are used. In this process, two of the prepared matrices in the pre-processing section are used. These two matrices are the ones in which nurse types and vehicle types are sorted according to their corresponding cost and called “the sorted-nurse-cost” matrix, and “the sorted-vehicle-cost” matrix, respectively. More precisely, to generate this solution, for each nurse route, first, the least cost nurse type, as well as the cheapest vehicle type, are used. Then, starting from the depot, each time the next patient is selected using the nearest neighbor strategy. This patient selection process continues as long as the priorities of patient on the nurse type as well as their associated time windows are not violated, or all patients are visited. As soon as there is no more patient to be assigned to the current nurse type and vehicle type, the route ends in the depot, and the next route is started. For the next route, the second cheapest nurse type and vehicle type are used and the same procedure is performed to generate the route. The whole process is repeated until all patients are assigned to a nurse route. An overview of the process of generating the first initial solution is presented in the Algorithm 2.
In the second strategy of generating the initial solution, The route generation process is very similar to the first initial solution except that the aim is to use nurse types with the highest service level and vehicles with the lowest emission. For the third initial solution, the priority is to use nurse types with the highest service level and vehicles with the highest speed.

4.2.2 Multi-objective shake
The multi-objective shake is applied to each existing solution in the current Pareto list and helps to escape from the local optimum by a perturbation strategy. The shake is composed of two steps, namely, the node-remove and the node-insertion.
For each solution in the current Pareto list, first, a predetermined number of visited nodes are removed randomly, and then the solution is reconstructed using the designed insertion move. The number of nodes to remove in each solution is calculated multiplying an algorithm parameter \((\alpha )\) by the number of patients. In the node-insertion step, the removed patients are inserted in a different position than they were visited before the removal, based on the min-cost insertion strategy. In case that the insertion in a new position is not feasible for every removed patient, then the shake is not performed at all.

4.2.3 Multi-objective VND
This module uses nine local neighborhood moves to improve the existing solutions.
These local moves are placed in four Variable Neighborhood Descent (VND) structures.
Each VND algorithm consists of local search operators which are applied iteratively with respect to an adopted neighborhood change strategy [33]. The strategy for the implemented VNDs is the Basic sequential VND (B-VND) [27]. The general structure of the B-VND algorithm is presented in Algorithm 5. In a B-VND structure, several local moves are applied to gradually improve the solution. The first local move is applied as long as it is able to improve the current solution. For the next local moves, each move is applied once. Then, if an improvement happens, the solution goes back to the first move again. Otherwise, the next local move is applied. This process continues until the last local move won’t be able to improve the solution. Although this algorithm is based on the main VND structure and already have been considered in other problems, each neighborhood is defined according to the characteristics of the objective functions. Moreover, during this step, new non-dominated solutions are generated [27]. Each local move is applied to improve the solution in terms of one of the objective functions.
As depicted in Algorithm 4, in the MOVND, for each VND structure, the input is the current Pareto list, and the output is a list of newly generated solutions within this VND (C-List). After applying the VND on every existing solution in the Pareto list, the Pareto list is updated by comparing its solutions with the solutions in the C-List. In this step, only non-dominated solutions are kept. Then, the updated Pareto list is used as the input for the next VND structure.
Each VND structure including its local moves is explained as follows. According to preliminary experiments, each of these nine local moves contributes to the quality of the final solution. It is also investigated in the sensitivity analyses as presented in Sect. 5.5.3.


VND-1 The neighborhood is designed to minimize the total cost including the visit cost and travel cost of nurses. Four local moves are designed and used in VND-1 namely Swap-best, Two-opt, Patient-exchange-cost, and Vehicle-exchange-cost.
-
Swap-best is the first local move in the VND-1 structure. This is a standard move that consists of simply swapping two nodes in the solution to reduce the travel cost [51]. Both nodes are taken from the same route. We implement the move in the best improvement manner so that, for each route, the best feasible swap is executed.
-
Two-opt is one of the most common local moves in solving routing problems. This move reduces the travel cost by exchanging two existing edges with two new edges. In our implementation, the best feasible Two-opt in each route is executed.
-
Patient-exchange-cost is specifically designed for our problem. It reduces the total cost of visiting a patient as well as the total travel cost by moving the corresponding patient node from one route to another route. This move is also implemented in the best improvement manner for the whole solution. So that, each time the move is executed, only one patient node is replaced.
-
Vehicle-exchange-cost, where, for each route, it is checked that if changing its currently used vehicle type to another available vehicle type reduces the travel cost. Then, the vehicle type with the minimum possible travel cost will be assigned to the considering route. It worth mentioning that, since each vehicle type may have a different travel time matrix, the time windows feasibility of patients are checked in this process.
VND-2 The VND-2 neighborhood structure reduces the total environmental emission. Since, the two local moves of “swap-best” and “two-opt” in VND1 focus on decreasing the total cost by reducing the total distance traveled by vehicles, and in order to prevent the overlap, VND2 consists of only one move which reduces the CO2 emissions. This move is called Vehicle-exchange-emission and is explained as follows. Since there exists only one move in this VND structure, it is repeatedly executed until no more improvement is possible.
-
Vehicle-exchange-emission is very similar to the previously defined Vehicle-exchange-cost move, except that the vehicle type is changed to reduce the total emission based on the corresponding \(e_{ijk}\).
VND-3 This neighborhood search structure consists of two local moves namely the Patient-exchange-workload, and the Vehicle-exchange-workload. These moves are improving each solution in terms of nurses’ workload balance.
-
Patient-exchange-workload is designed to balance nurses’ total working time including their travel time, service time, and waiting time. This move also exchanges patients between nurse routes and therefore is very similar to Patient-exchange-cost. The difference is that here the acceptance and selection criteria is the working time balance of nurses. To get a more balanced working time, we reduce the Sum Absolute Deviation (SAD) of working times associated with each nurse route. To find the SAD using the Eq. 28, first, the total working time of each nurse (np) is calculated for each route (\(Z_{np}\)). \(\bar{Z}\) is the average value of \(Z_{np}\)s.
$$\begin{aligned} \sigma =\sum _{i \in N}|Z_i-\bar{Z}| \end{aligned}$$(28) -
Vehicle-exchange-workload tries to reduce the total working time of each nurse route by assigning the fastest vehicle type. It is implemented as the best improvement move and keeps track of the time windows violation.
VND-4 The neighborhood structure consists of two local moves that improve the service quality.
-
Patient-exchange-service level, where, each patient is considered to move to another existing route with a nurse type of having a higher level of service. Indeed the patient priority, as well as the feasibility of moving to the chosen route in terms of time windows, is checked. The best improvement strategy is used for implementation.
-
Nurse-exchange-service level, in which, the currently assigned nurse type to each route is considered for a change to a nurse type with a higher service level. The patients’ preferences and the feasibility of time windows are checked for the new nurse type.
4.2.4 MONeighborhoodChange / Update Pareto list
As mentioned earlier, after applying each VND structure, the list of generated solutions in the VND (C-List), is compared with the current Pareto list. For this comparison, each solution from the C-List is compared with all existing solutions in the Pareto list in terms of their corresponding objective values. Based on this comparison, the Pareto list is updated, and only non-dominated solutions are kept to be used in the rest of the algorithm.
5 Computational results
In this section, the results of performing both solution methods are presented. Since no benchmark instances are available in the literature for the investigated problem, first it is explained how new instances are generated. Then, three standard metrics are described to evaluate the performance of the multi-objective solution methods. Finally, the results of applying both implemented methods on generated instances are presented and analyzed using the introduced metrics. Before applying the MOVNS method, the parameters of this algorithm are tuned.
The epsilon-constraint method is implemented in CPLEX 12.6, and the MOVNS algorithm is implemented in MATLAB R2016b version 9.1. All computations are carried out on a personal computer Intel Core i7 with a 3.1 GHz processor and 8.00 GB RAM.
5.1 Test instances
Since the investigated problem in this research comes from a real case, there are differences in the model compared to the literature. These novel properties including the infinite number of nurses and vehicles of different types, various nurse types with associated service levels, and patient priorities and preferences which are introduced in the current research, make it senseless to use any existing instances from the literature.
In total 30 instances are generated which are classified into two sets of small and large instances. The set of small problem instances contains 15 instances ranging from 4 to 15 patients, 2 to 3 nurse types, and 2 to 3 vehicle types. The set of large problem instances contains 15 instances ranging from 25 to 60 patients, 2 to 4 nurse types, as well as 2 to 4 vehicle types. The complete list of instances mentioning their associated number of patients (|U|), the number of nurse types (|N|), and the number of vehicle types (|K|) is presented in Table 2.
To generate the instances, first, 4 different types of nurses are considered. The visit cost (\(vc_n\)) as well as the associated service level \(sl_n\) for each nurse type (n) is assumed to be as presented in Table 3. Nurses’ service level correlates with factors such as visit cost, work experience, and treatment expertise. Similarly, four types of vehicles are considered. The corresponding travel cost (\(v^C_k\)), and produced \(\mathrm{{CO}}_2\) emission (\(v^E_k\)) per unit distance traveled by each vehicle type as well as their associated vehicle speed (\(v^S_k\)) are presented in Table 4. The \(\mathrm{{CO}}_2\) emission rates are derived from the www.co2nnect.org website (Gram per Kilometer).
The corresponding ranges for all relevant parameters are presented in Table 5. The coordination of patients’ locations is uniformly distributed in the [5,15] interval. The Euclidean distance is used to calculate the distance matrix (\(d_{ij}\)). The travel cost \(c_{ijk}\), and the \(\mathrm{{CO}}_2\) emission \(e_{ijk}\) matrices are generated by multiplying the corresponding rates of each vehicle type by the distance matrix. The travel time matrix \(t_{ijk}\), is calculated by dividing the distance matrix by the associated speed of each vehicle type. The service time (\(st_i\)) for each patient is randomly generated in range from 30 to 100 with a step-size of 5 ({30, 35,40,..., 100}). The opening of time window of each patient (\(ot_i\)) is randomly generated within an integer uniform interval of [0,520]. Then, the closing times (\(ct_i\)) are generated accordingly, by adding an integer random value from the interval of [50,200] to the corresponding opening time. Patients’ preferences \((pr_{in})\) are also randomly chosen binary values providing that for each patient at least one nurse type gets the value of “1”.
5.2 Evaluation metrics for the quality of Pareto solutions
Results of multi-objective algorithms are usually an approximation of the Pareto optimal set. Thus, an important issue is to compare the performance of these algorithms with each other. There are a number of metrics introduced in the literature for this kind of comparison [3]. Traditionally, the main two goals for a MO procedure are a good convergence to the Pareto optimal front, and a good diversity in obtained solutions. Three types of metrics are usually considered for performance measurement, which evaluate the spread of solutions on the known Pareto optimal front, the convergence to the known Pareto optimal front, and a certain combinations of convergence and spread of solutions [9, 45]. In this research, to evaluate the performance of the proposed MOVNS and compare its results with the epsilon-constraint method, five metrics are considered. Regarding the convergence, Mean Ideal Distance (MID) and regarding the diversity, Maximum Spread Index (MSI) are considered respectively. Moreover, the two common metrics of Number of Pareto Solutions (NPS) and Hyper Volume (HPV) are used to evaluates both the convergence and diversity simultaneously. In addition, the quality of the algorithm is analyzed based on the computational time (CPU). These metrics are briefly explained as follows.
-
Mean Ideal Distance (MID): The MID metric calculates the mean deviation of Pareto solutions from the ideal solution as shown by Eq. 29 [37]. In this Equation, n shows the number of Pareto solutions, j is the index of the objective function, and \(f^{j}_{Max}\) and \(f^{j}_{Min}\) represent the highest and the lowest values of \(jth\) objective, respectively. \(f^{j}_{Best}\) shows the ideal value of the corresponding objective. We consider the best value of each objective function among the solutions in the Pareto list as the corresponding ideal value. The lower the value of MID, the higher the quality of the Pareto list.
$$\begin{aligned} MID=\frac{\sum _{j=1}^{4}\sum _{i=1}^{n}\sqrt{\left( \frac{f^j_i-f^{j}_{Best}}{f^j_{Max}-f^{j}_{Min}}\right) ^2}}{n} \end{aligned}$$(29) -
Maximum Spread Index (MSI): This metric is introduced by Zitzler and Thiele [56]. and shows the diversity of Pareto solutions. The larger value of MSI indicates that solutions are scattered on a broader space, which shows the higher performance of the algorithm [3]. Using the introduced notations, Eq. 30 can be applied to calculate the MSI metric.
$$\begin{aligned} D=\sqrt{\sum _{j=1}^{4}\left( f^j_{Max}-f^j_{Min}\right) ^2} \end{aligned}$$(30) -
Number of Pareto Solutions (NPS): NPS metric measures the number of approximate non-dominated Pareto solutions that evaluate the performance of the algorithm. Indeed, the higher the NPS value, the better the M-O algorithm.
-
Hyper Volume (HPV): HPV metric is defined as a quality measure of n non-dominated objective vectors, \(PF = p^{1}, p^{2},..., p^{n}\), in a M-O optimization. Concerning a minimization problem with m objectives, the HPV indicator consists of the region that simultaneously is dominated by PF and bounded above by a reference point \(r\in R^{m}\) such that:
\(r\ge (max_pP1,..., max_pPm)\) where, \(p=(p_1,..., p_m) \in P\subseteq R^{m}\), and the relation \(\ge\) applies component-wise. In Fig. 1, this region consists of an orthogonal polytope and may be seen as the union of n axis-aligned hyper-rectangles with one common vertex (the reference point,r) [21] To calculate the HPV for both the MOVNS and epsilon method, the approximation approach introduced by Deng and Zhang [12] is considered. The reference point is assumed as the worst objective value obtained by any of the methods. All values are normalized in [0,1], and (1.1, 1.1, 1.1) is regarded as the reference point.
-
CPU-Time: The computational time is also used as an important metric to evaluate algorithm performance. It is evident that the lower value of CPU time has more advantages.

The hyper volume metric for a given Pareto front, and a reference point (r) [21]
5.3 Parameters tuning
Parameter tuning is an approach to determine appropriate parameter settings for an algorithm. Designing a statistical experiment is one of the most commonly used methods for tuning the parameters. The adjustable parameters in the proposed MOVNS are the maximum number of iterations of the algorithm (maxIteration), and the coefficient used in the multi-objective shake structure (\(\alpha\)). These parameters are set separately, for small and large data sets to get a more sophisticated result. To do this, five instances were randomly selected from each of the the small and large set of instances. Based on preliminary experiments, initial values for each parameter are chosen. Then the corresponding value levels are decided as presented in Table 6.
For each parameter, three levels are considered. Since there are not many parameters to set in the proposed MOVNS, the full factorial experiments are performed. Therefore, 9 experiments are performed for each instance stating different values of each parameter. The evaluation metrics are calculated accordingly. It worth mentioning that, due to relatively high number of experiments, for the parameters tuning only MID, MSI, and CPU are used to compare different settings.
To have a fair comparison, the obtained values of each metric are normalized between 0 and 1 over all 5 instances, using Eq. 31. For example for the MID metric, in this equation, \(x_i\) shows the associated value for instance i, and \(x_{min}\), and \(x_{max}\) are the minimum and maximum MID values over 5 investigated instances, respectively.
Then, for each of the 9 states of parameter values, the average of each metric is calculated and shown in Table 7.
Finally, these states are sorted, giving a higher priority first, to their corresponding MID, second to the CPU, and third, to the MSI values. As a result, the selected values for each parameter and each set of instances (Small / Large) are presented in Table 8.
5.4 Results and discussion
To evaluate the proposed solution methods, generated test instances are solved using both epsilon-constraint as well as the MOVNS. First, the experimental results obtained from applying both solution methods on the set of small instances, are presented in Table 9. The first column shows the instance name and specifications in the format of \(SPi(u-n-k)\) where i is the instance number, and u, n, k shows the number of patients, nurse types, and vehicle types, respectively. In this table, each instance has solved one time by using each method, and the obtained results are summarized in terms of the evaluation metrics (MID, MSI, CPU, NPS, HPV). Since for these small instances, the MOVNS is compared against the epsilon-constraint method, to calculate the MID metric, the optimal value of each objective function, j, is considered as the corresponding ideal value (\(f^{j}_{Best}\)).

A comparison between the epsilon-constraint and the MOVNS algorithm in terms of the evaluation metrics: MID,MSI, CPU, NPS, HPV
It is observed that even for a small set of instances, for the ones containing more than 13 nodes, the epsilon-method was not able to find any solution due to memory problems. Therefore, all the comparisons for this set are based on 13 instances of the smallest sizes. To have a better understanding, the values of each metric obtained from the results of both solution methods are presented in Fig. 2. In this figure, parts A, B, C, D, and E depict the comparison of the results for the MID, MSI,CPU, NPS, and HPV respectively. It can be seen from Fig. 2, and Table 9 that, the MOVNS method outperforms the epsilon-constraint over all instances in terms of all three metrics.
The results of solving set of large instances are presented in Table 10. For the set of large instances, we have only applied the MOVNS method to show the usability of the method for instances closer to the real-word size. For these experiments, to calculate the MID metric, the ideal solution is composed of the best value of each objective function among all the obtained non-dominated solutions. Since the epsilon-constraint method could not solve these instances, no comparison is performed over the results. It can be concluded that although the CPU time is getting higher by increasing the instance size, the largest CPU time is still around half an hour, which is acceptable for the nurse scheduling application.
5.5 Sensitivity analysis
In this section, the behavior of the proposed method is evaluated by different sensitivity analyses. The main idea of these analyses is to investigate the impact of the main parts of the MOVNS. First, the impact of each of the initial solution strategies on the final solution is checked. Then, the performance of each neighborhood structure (\({VND}_i\)) is analyzed. Three instances are selected randomly from both small and large sets of instances to perform all sensitivity analyses. To show the impact of each of the mentioned parts of the algorithm, the obtained results in the case that the corresponding algorithm part is skipped, are compared against the final results of the complete algorithm.
5.5.1 The influence of initial solutions
To perform this analysis, the MOVNS algorithm is used to solve the selected instances each time by skipping one of the initial solution strategies. We used the five introduced metrics for these comparisons. The results of removing each of the initial solution strategies are presented in Table 11.
In this table, the first column is the instance name, the second column is the metric name, and the third column shows the metrics’ values when the full algorithm is used. As can be seen, in all cases, eliminating the initial solution causes an increase in the MID values and a decrease in MSI, CPU, NPS and HPV values. To have a better understanding, the impact of removing each of the initial solution strategies are presented as an average change percentage (avg Increase/decrease) in the last rows of Table 11. These values are calculated by using Eq. 32.
where, k corresponds to removing the \(k^{th}\) initial strategy; \(v^1_j\), is the MID, the CPU, or the MSI value obtained from solving the instance j, using the full MOVNS, and, \(v^k_j\) is the value of the same metric when in the algorithm, the \(k^{th}\) initial strategy is skipped.
As a result, it is observed that removing each of the proposed initial solution strategies has a significant effect on the quality of final solutions. Moreover, it can be concluded that for the selected instances, the first initial solution strategy has the largest effect on the solution quality.
5.5.2 The influence of neighborhood structures
Similar to the sensitivity analysis of initial solution strategies, in this section, the influence of VND structures is investigated. Thereby, three types of experiments were run, by removing each of the VND structures separately. Again, the change in the MID, CPU, and MSI metrics are calculated using the Eq. 32, where this time, k corresponds to removing the \(k^{th}\) VND structure from the algorithm. According to Table 12, although the amount of change in the quality of the results depends on the instance size, the average change (%) reported for removing each of the VND structures, clearly indicates that all four VND structures have remarkable effect on the quality of final solutions. It can also be interpreted that, the first and the third VND structures are the most effective ones.
5.5.3 The influence of local moves
In this section, two sets of experiments are conducted to determine the influence of each existing local moves and their order of presence in the VNDs. Similar to the previous sections, all experiments are performed on three randomly selected instances.
To show the contribution of each local move on the quality of the solution, in the first set of experiments, the proposed MOVND is compared against 9 different versions where each time one local move is missing. Results are presented in Table 13. An average value of percentage changes in each evaluation metric over all three instances is presented at the bottom lines of the table. It can be seen that except for very few cases for the HPV metric, for every other metrics and in almost all cases the values are worsened when any local move is removed.
The second set of experiments concern the order of local moves within each VND. For these experiments, three other versions of the MOVND are compared to the proposed MOVND. Considering the number of local moves in each VND, only one order change would be possible in both VND-3, and VND-4, and no change for VND-2. These two sets of changes are presented as reordering Move 6 and Move 7 for VND-3, and reordering Move 8 and Move 9 for VND-4. Regarding the first VND which is composed of four local moves, here we have only presented the results for changing the order of Move 1 and Move 2 as the two more important local moves in this VND. As presented in Table 14, without no exception, in all cases no improvement is found in any metric by any of the investigated reordering.
6 Case study
In this section, the proposed solution approach is tested over a real example. This example is derived from the case of an HHC company in the city of Tehran.Footnote 1 The HHC center provides counseling, nursing, laboratory, and physiotherapy services to various groups of customers including patients, the elderly, and children. According to our survey, it offers more than 500 services per month. Each patient applies for one or more services in advance. Normally, there are a large number of medical staff registered at the institute. This staff is paid based on the number and types of accomplished services. Therefore it is possible to assume that an unlimited number of different medical staff types is available every day. Each day, the institute needs to assign proper medical staff to each patient depending on the preferences and the associated time window. This planning has to be made a day in advance so that the medical staff is informed about their visit plans for the next day.
The medical staff in this institute is divided into four groups according to their associated service level, namely types 1 to 4. Nurses are ranked and categorized based on different factors that are important to the institution. Some of the main factors considered by the institute include records of previous experiences of the nurse and the associated feedback from previous patients, the academic background, and relevant skills.
When a medical staff is assigned to provide services to one or more patients, he/she should first come to the institute to receive the necessary equipment and start his/her visit tour. At the end of the day, after finishing the tour, the equipment needs to be delivered to the institute again. There are three vehicle types available for the medical staff, namely, the institution vehicle or the vehicle which is rented by the institution, the personal vehicle of the staff which is also paid by the company in case of usage, and the public transport. Details of the information on medical staff and vehicle types are presented in Tables 15 and 16.
In our example, on one specific day of the institute, 30 patients received services from the medical staff.
When a patient contacts the institute, the necessary information including his/her preferred time window, and the proper types of medical staff is identified. Moreover, the necessary service time is also estimated by the institute.
The MOVNS is used to solve the described HHC example. As a result, 327 Pareto solutions are obtained. Based on these results, the quality metrics of MID and MSI are 1.02 and 2603.2, respectively. It took 244.12 s for the MOVNS to find these solutions.
Although it gives flexibility to the decision-maker to have a list of non dominated solutions at hand, in practice, how to select the desired solution from the Pareto list is always an issue. Specifically, in this case, 161 Pareto solutions are a large number that can’t be directly provided to the decision-maker. Therefore, in the following sections, first, four best solutions based on each objective function, are selected out of the obtained Pareto solutions. These solutions are also used to analyze the performance of the MOVNS. Then, a Multi-Criteria Decision Making (MCDM) method is used to propose one best solution to the decision-maker. Using such a technique would make the method more practical in real-world applications.
6.1 The best solution for each objective
In this section, four solutions are selected among all the Pareto solutions, each of them having the best value in one of the objective functions to highlight the conflicts between considered objectives. Table 17 shows the objective values of these four selected solutions.
Detailed solution structures corresponding to these four solutions are presented in Tables 18, 19, 20,21. In the solution structure, node 1 is the HHC Institute, and nodes 2 to 31 are the patients’ locations.
According to these results, in the first solution, the first objective has the lowest cost of 3,910,690, while it caused a considerable increase in emission and max-workload from their best values 12.5 and 592.6 in solutions 2 and 3, to 14.75 and 616.70, respectively. Also, the service level is reduced from 212 in Solution 4 to 177. It is clear that, the best value of each objective function achieved by sacrificing the values of other objectives, which indicates an existing conflict between the considered objectives.
Minimizing operating costs is the first and foremost goal for home health care providers. The total costs include transportation cost and patient visits cost. Thus, to minimize the total costs, the MOVNS tends to use the cheapest vehicle as well as the cheapest medical staff to service the patients. Nevertheless, the availability of each patient and his/her preferences on medical staff types have to be followed. As can be seen in Table 18, the public transportation facility (vehicle type 3) as the cheapest vehicle type, is selected for all the medical staff routes. Moreover, the most expensive medical staff type (type 1) selected for just one route to prevent the extra cost of visiting.
Table19 shows the structure of the solution for the minimum emission Pareto solution. The least environmentally pollutant vehicle type (type 3), is selected for all routes. Moreover, since the type of selected medical staff is not important for the emission objective function, contrary to the previous solution structure, medical staff type 1 is selected for visiting more nodes. It is worth noting that, in both structures, vehicle type 3 is selected because of its cheapest cost and lowest emission.
The third solution presented in Table 20 has the best value of the third objective function, the min-max workload. As described in Sect. 3, for this objective, we minimize the maximum time spend by medical staff during the route. Therefore, the lower value for this objective function indicates a more balanced solution. According to the solution structure shown in Table 20, vehicles type 1 and 2, as the fastest vehicles are allocated to the routes with longer trips which leads to a lower travel time, and is in line with minimizing the time spent by medical staff.
Table 21 shows the Pareto solution in which the highest service level medical staff are selected in most of to maximize the fourth objective value. As observed, medical staff types 1 and 2 with the highest service level, are selected the most. Note that, the selection of nurses is also based on the preferences of the patients.
6.2 Selecting one best solution
If the decision-maker prefers to select one specific solution among the Pareto solutions, MCDM would be an effective option. For the current example, we use the method of Displaced Ideal Solution (DIS) proposed by Zeleny [54]. The DIS is an MCDM method that looks for a solution with the minimum distance from the ideal point, using Eq. 33 [31]. In this equation, \(f^j_{Best}\) is the best value of \(j^{th}\) objective function, and \(f^j_i\) is the value of that objective function in the considering solution. The set of Pareto solutions are then sorted according to the DIS metric.
In our example, one solution with the minimum distance to the ideal point is selected. The value of objective functions for this selected solution next to the best value of each objective function (the ideal point) is presented in Table 22, and the solution structure is depicted in Table 23.
7 Conclusion and future work
In this paper, a four-objective mathematical model for optimizing home health care routing is proposed based on a real case of a HHC institute. The presented model is developed for planning, allocating, and routing HHC medical staffs in a limited time, with the objectives of minimizing the cost of visiting patients and transportation, minimizing the environmental pollution of transportation activities, maximizing the workload balance between assigned medical staffs, and maximizing the level of service to patients. One of the essential assumptions of the model is to consider the preferences of patients in receiving higher levels of services by assigning higher quality medical staff. In addition, hard time windows are considered to reflect the available time of each patient. Based on the studied case, the main practical characteristic of the problem is to consider an unlimited number of various types of medical staff for planning. To solve this complex problem, a MOVNS meta-heuristic is designed and implemented.
Based on the sensitivity analysis, the flexible structure of the developed MOVNS makes it capable to efficiently solve the multi-objective optimization HHC problem, by employing local moves aiming at each specific objective. It is shown that the multiple VND structure as well as using multiple strategies to generate the initial set of solutions contribute to the quality of the achieved Pareto set. Comparing the results of the MOVNS against the epsilon-constraint method indicate that even for smaller instances, the epsilon method takes a long computation time and only gives a very limited number of Pareto solutions. On the other hand, the MOVNS is able to provide a large number and higher quality Pareto solutions in short computation time. However, for the largest solved instance, the MOVNS takes about half an hour to find the Pareto set. Therefore, a more efficient implementation of the algorithm in a faster programming language would make it more practical.
Furthermore, a real example from Tavan Salamat Institute in Tehran is used to show the applicability of the proposed method. According to this case study, it can be seen that the four mentioned objectives in the model help the planners to pay attention to important dimensions of home health care institutions. The higher level of services, in terms of assigning more appropriate medical staff to patients, as one of the objective functions in the present study, is an indicator of the stability of the company in the competitive market of health care institutions, so these institutions must pay more attention to patients’ priorities and preferences. Optimal allocations can satisfy patients and thus improve the company value. Considering public transportation as a transport mode for medical staff is an effective solution to reduce both total costs and environmental pollution.
For the future, this research can be extended from both modeling and solution method points of view. To get closer to real-world problems, the model can be considered as a multi-depot problem where nurses start their job from multiple offices of an HHC company. Moreover, some home health services do not require special equipment, so the medical staff can start his/her tour from home. Another possibility would be to study uncertainty in the duration of services or travel times. To improve the solution method, other meta-heuristic methods can be implemented, to have a better comparison of the results for larger instances. In addition, adaptive reordering for VND can be considered in future research. In an adaptive VND, in each iteration the order of the neighborhoods is altered based on the success of the previous iteration [33, 47]. Other multi-criteria decision-making methods can also be used to provide a limited number of Pareto solutions to the decision-maker.
Data availability
The datasets generated during the current study are available in the github repository, [https://github.com/DivsalarA/MOHHC]
Code availability
The code is not public currently.
Notes
Tavan Salamat Institute: www.tavanparastar.com.
References
Akjiratikarl, C., Yenradee, P., Drake, P.R.: Pso-based algorithm for home care worker scheduling in the UK. Comput. Ind. Eng. 53(4), 559–583 (2007)
Allaoua, H., Borne, S., Létocart, L., Calvo, R.W.: A matheuristic approach for solving a home health care problem. Electron. Notes Discret. Math. 41, 471–478 (2013)
Arjmand, M., Najafi, A.A.: Solving a multi-mode bi-objective resource investment problem using meta-heuristic algorithms. Adv. Comput. Tech. Electromagn. 1(1), 41–58 (2015)
Arroyo, J.E.C., dos Santos, Ottoni R., de Paiva, Oliveira A.: Multi-objective variable neighborhood search algorithms for a single machine scheduling problem with distinct due windows. Electron. Notes Theor. Comput. Sci. 281, 5–19 (2011)
Bahadori-Chinibelagh, S., Fathollahi-Fard, A.M., Hajiaghaei-Keshteli, M.: Two constructive algorithms to address a multi-depot home healthcare routing problem. IETE J. Res. 68(2), 1108–1114 (2022)
Braekers, K., Hartl, R.F., Parragh, S.N., Tricoire, F.: A bi-objective home care scheduling problem: analyzing the trade-off between costs and client inconvenience. Eur. J. Oper. Res. 248(2), 428–443 (2016)
Bredström, D., Rönnqvist, M.: Combined vehicle routing and scheduling with temporal precedence and synchronization constraints. Eur. J. Oper. Res. 191(1), 19–31 (2008)
Cissé, M., Yalçındağ, S., Kergosien, Y., Şahin, E., Lenté, C., Matta, A.: OR problems related to home health care: a review of relevant routing and scheduling problems. Oper. Res. Health Care 13, 1–22 (2017)
Deb, K.: Multi-objective optimisation using evolutionary algorithms: an introduction. In: Multi-objective evolutionary optimisation for product design and manufacturing, Springer, pp 3–34 (2011)
Decerle, J., Grunder, O., El Hassani, A.H., Barakat, O.: A hybrid memetic-ant colony optimization algorithm for the home health care problem with time window, synchronization and working time balancing. Swarm Evolut. Comput. 46, 171–183 (2019)
Demirbilek, M., Branke, J., Strauss, A.K.: Home healthcare routing and scheduling of multiple nurses in a dynamic environment. Flex. Serv. Manuf. J. 33(1), 253–280 (2021)
Deng, J., Zhang, Q.: Combining simple and adaptive Monte Carlo methods for approximating hypervolume. IEEE Trans. Evolut. Comput. 24(5), 896–907 (2020)
Duarte, A., Pantrigo, J.J., Pardo, E.G., Mladenovic, N.: Multi-objective variable neighborhood search: an application to combinatorial optimization problems. J. Glob. Optim. 63(3), 515–536 (2015)
Erdem, M., Bulkan, S.: A literature review on home healthcare routing and scheduling problem. Eurasian J. Health Technol. Assess. 2(1), 19–32 (2017)
Erdem, M., Koç, Ç.: Analysis of electric vehicles in home health care routing problem. J. Clean. Prod. 234, 1471–1483 (2019)
Fan, Z., Li, W., Cai, X., Huang, H., Fang, Y., You, Y., Mo, J., Wei, C., Goodman, E.: An improved epsilon-constraint-handling method in MOEA/D for CMOPs with large infeasible regions. Soft Comput. 23(23), 12491–12510 (2019)
Fathollahi-Fard, A.M., Hajiaghaei-Keshteli, M., Tavakkoli-Moghaddam, R.: A bi-objective green home health care routing problem. J. Clean. Prod. 200, 423–443 (2018)
Fernandez, A., Gregory, G., Hindle, A., Lee, A.: A model for community nursing in a rural county. J. Oper. Res. Soc. 25(2), 231–239 (1974)
Fikar, C., Hirsch, P.: A matheuristic for routing real-world home service transport systems facilitating walking. J. Clean. Prod. 105, 300–310 (2015)
Fikar, C., Hirsch, P.: Home health care routing and scheduling: a review. Comput. Oper. Res. 77, 86–95 (2017)
Fonseca, C.M., Paquete, L., López-Ibánez, M.: An improved dimension-sweep algorithm for the hypervolume indicator. In: 2006 IEEE international conference on evolutionary computation, IEEE, pp 1157–1163 (2006)
Frifita, S., Masmoudi, M.: VNS methods for home care routing and scheduling problem with temporal dependencies, and multiple structures and specialties. Int. Trans. Oper. Res. 27(1), 291–313 (2020)
Gao, X., Cao, C.: Multi-commodity rebalancing and transportation planning considering traffic congestion and uncertainties in disaster response. Comput. Ind. Eng. 149, 106782 (2020)
Goodarzian, F., Hosseini-Nasab, H., Muñuzuri, J., Fakhrzad, M.B.: A multi-objective pharmaceutical supply chain network based on a robust fuzzy model: a comparison of meta-heuristics. Appl. Soft Comput. 92, 106331 (2020)
Grieco, L., Utley, M., Crowe, S.: Operational research applied to decisions in home health care: a systematic literature review. J. Oper. Res. Soc. 72(9), 1960–1991 (2021)
Gutiérrez, E.V., Vidal, C.J.: Home health care logistics management: framework and research perspectives. Int. J. Ind. Eng. Manag. 4(3), 173–182 (2013)
Hansen, P., Mladenović, N., Todosijević, R., Hanafi, S.: Variable neighborhood search: basics and variants. EURO J. Comput. Optim. 5(3), 423–454 (2017)
Hiermann, G., Prandtstetter, M., Rendl, A., Puchinger, J., Raidl, G.R.: Meta-heuristics for solving a multi-modal home-healthcare scheduling problem. Cent. Eur. J. Oper. Res. 23(1), 89–113 (2015)
Hindle, T., Hindle, A., Spollen, M.: Resource allocation modelling for home-based health and social care services in areas having differential population density levels: a case study in Northern Ireland. Health Serv. Manag. Res. 13(3), 164–169 (2000)
Hindle, T., Hindle, G., Spollen, M.: Travel-related costs of population dispersion in the provision of domiciliary care to the elderly: a case study in English Local Authorities. Health Serv. Manag. Res. 22(1), 27–32 (2009)
Hwang, C.L., Masud, A.S.M.: Multiple objective decision making-methods and applications: a state-of-the-art survey, vol. 164. Springer Science & Business Media, Berlin (2012)
Karakostas, P., Panoskaltsis, N., Mantalaris, A., Georgiadis, M.C.: Optimization of car t-cell therapies supply chains. Comput. Chem. Eng. 139, 106913 (2020)
Karakostas, P., Sifaleras, A., Georgiadis, M.C.: Adaptive variable neighborhood search solution methods for the fleet size and mix pollution location-inventory-routing problem. Exp. Syst. Appl. 153, 113444 (2020)
Khodabandeh, P., Kayvanfar, V., Rafiee, M., Werner, F.: A bi-objective home health care routing and scheduling model with considering nurse downgrading costs. Int. J. Environ. Res. Public Health 18(3), 900 (2021)
Lanzarone, E., Matta, A.: Robust nurse-to-patient assignment in home care services to minimize overtimes under continuity of care. Oper. Res. Health Care 3(2), 48–58 (2014)
Liang, Y.C., Lo, M.H.: Multi-objective redundancy allocation optimization using a variable neighborhood search algorithm. J. Heuristics 16(3), 511–535 (2010)
Maghsoudlou, H., Afshar-Nadjafi, B., Niaki, S.T.A.: A multi-objective invasive weeds optimization algorithm for solving multi-skill multi-mode resource constrained project scheduling problem. Comput. Chem. Eng. 88, 157–169 (2016)
Manavizadeh, N., Farrokhi-Asl, H., Beiraghdar, P.: Using a metaheuristic algorithm for solving a home health care routing and scheduling problem. J. Proj. Manag. 5(1), 27–40 (2020)
Mankowska, D.S., Meisel, F., Bierwirth, C.: The home health care routing and scheduling problem with interdependent services. Health Care Manag. Sci. 17(1), 15–30 (2014)
Mutingi, M., Mbohwa, C.: Multi-objective homecare worker scheduling: a fuzzy simulated evolution algorithm approach. IIE Trans. Healthc. Syst. Eng. 4(4), 209–216 (2014)
Nasir, J.A., Kuo, Y.H.: A decision support framework for home health care transportation with simultaneous multi-vehicle routing and staff scheduling synchronization. Decis. Support Syst. 138, 113361 (2020)
Nasir, J.A., Hussain, S., Dang, C.: An integrated planning approach towards home health care, telehealth and patients group based care. J. Netw. Comput. Appl. 117, 30–41 (2018)
Osorio-Mora, A., Soto-Bustos, M., Gatica, G., Palominos, P., Linfati, R.: The multi-depot cumulative vehicle routing problem with mandatory visit times and minimum delayed latency. IEEE Access 9, 27210–27225 (2021)
Rest, K.D., Hirsch, P.: Daily scheduling of home health care services using time-dependent public transport. Flex. Serv. Manuf. J. 28(3), 495–525 (2016)
Riquelme, N., Von Lücken, C., Baran, B.: Performance metrics in multi-objective optimization. In: 2015 Latin American computing conference (CLEI), IEEE, pp 1–11 (2015)
Shi, Y., Boudouh, T., Grunder, O.: A hybrid genetic algorithm for a home health care routing problem with time window and fuzzy demand. Exp. Syst. Appl. 72, 160–176 (2017)
Simeonova, L., Wassan, N., Salhi, S., Nagy, G.: The heterogeneous fleet vehicle routing problem with light loads and overtime: Formulation and population variable neighbourhood search with adaptive memory. Exp. Syst. Appl. 114, 183–195 (2018)
de Siqueira, E.C., Souza, M.J., de Souza, S.R.: A multi-objective variable neighborhood search algorithm for solving the hybrid flow shop problem. Electron. Notes Discr. Math. 66, 87–94 (2018)
Smiti, N., Dhiaf, M.M., Jarboui, B., Hanafi, S.: Skewed general variable neighborhood search for the cumulative capacitated vehicle routing problem. Int. Trans. Oper. Res. 27(1), 651–664 (2020)
Taghipour, F., Tavakkoli-Moghaddam, R., Eghbali-Zarch, M.: Home healthcare routing and scheduling problem during the covid-19 pandemic. In: IFIP International Conference on Advances in Production Management Systems, Springer, pp 373–382 (2021)
Toffolo, T.A., Christiaens, J., Van Malderen, S., Wauters, T., Berghe, G.V.: Stochastic local search with learning automaton for the swap-body vehicle routing problem. Comput. Oper. Res. 89, 68–81 (2018)
Trautsamwieser, A., Gronalt, M., Hirsch, P.: Securing home health care in times of natural disasters. OR spectrum 33(3), 787–813 (2011)
Yuan, B., Liu, R., Jiang, Z.: A branch-and-price algorithm for the home health care scheduling and routing problem with stochastic service times and skill requirements. Int. J. Prod. Res. 53(24), 7450–7464 (2015)
Zeleny, M.: Multiple criteria decision making Kyoto 1975, vol. 123. Springer Science & Business Media, Berlin (2012)
Zhang, S., Lee, C., Choy, K., Ho, W., Ip, W.: Design and development of a hybrid artificial bee colony algorithm for the environmental vehicle routing problem. Transp. Res. Part D Transp. Environ. 31, 85–99 (2014)
Zitzler, E., Thiele, L.: Multi-objective evolutionary algorithms: a comparative case study and the strength pareto approach. IEEE Trans. Evolut. Comput. 3(4), 257–271 (1999)
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
GK: Writing- Original draft preparation, Software, Investigation. AD: Conceptualization, Methodology, Validation, Supervision, Writing- Reviewing and Editing. SE: Methodology, Reviewing and Editing, Supervision.
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kordi, G., Divsalar, A. & Emami, S. Multi-objective home health care routing: a variable neighborhood search method. Optim Lett 17, 2257–2298 (2023). https://doi.org/10.1007/s11590-023-01993-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11590-023-01993-y