
Abstract
Background
The purpose of this study is to evaluate patient’s perceptions of physician reimbursement for the most commonly performed surgery on the hand, a carpal tunnel release (CTR).
Methods
Anonymous physician reimbursement surveys were given to patients and non-patients in the waiting rooms of orthopaedic hand physicians’ offices and certified hand therapist’s offices. The survey consisted of 13 questions. Respondents were asked (1) what they thought a surgeon should be paid to perform a carpal tunnel release, (2) to estimate how much Medicare reimburses the surgeon, and (3) about how health care dollars should be divided among the surgeon, the anesthesiologist, and the hospital or surgery center. Descriptive subject data included age, gender, income, educational background, and insurance type.
Results
Patients thought that hand surgeons should receive $5030 for performing a CTR and the percentage of health care funds should be distributed primarily to the hand surgeon (56 %), followed by the anesthesiologist (23 %) and then the hospital/surgery center (21 %). They estimated that Medicare reimburses the hand surgeon $2685 for a CTR. Most patients (86 %) stated that Medicare reimbursement was “lower” or “much lower” than what it should be.
Conclusion
Respondents believed that hand surgeons should be reimbursed greater than 12 times the Medicare reimbursement rate of approximately $412 and that the physicians (surgeons and anesthesiologist) should command most of the health care funds allocated to this treatment. This study highlights the discrepancy between patient’s perceptions and actual physician reimbursement as it relates to federal health care. Efforts should be made to educate patients on this discrepancy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
“If a family care physician works with his or her patient to help them lose weight, modify diet, monitors whether they’re taking their medications in a timely fashion, they might get reimbursed a pittance. But if that same diabetic ends up getting their foot amputated, that’s $30,000, $40,000, $50,000—immediately the surgeon is reimbursed.” – Barack Obama, Portsmouth, NH, August 11, 2011.
These comments incited significant concern from orthopaedic surgeons and vascular surgeons alike. In fact, the Medicare allowable physician reimbursement for a below-the-knee amputation (CPT 27880) is $925.09 [3]. This is no less than a 32-fold discrepancy in the President’s perceptions and actual physician reimbursement. These inaccurate declarations have led to the development of policies to reduce health care costs by targeting Medicare physician reimbursements. Medicare physician reimbursements are consistently declining [7] while health care costs in the USA are rapidly approaching unsustainable levels [9]. These truths combined with the fact that medical inflation [5, 6] is rising more quickly than Medicare reimbursements [1, 2] have placed physicians in a precarious position.
Given the current level of focus and debate surrounding physician reimbursements in the US health care system, it is important to determine our patient’s level of understanding regarding these issues so they will be better informed consumers of medical care and cost. The purpose of this study is to evaluate patient’s perceptions of a hand surgeon performing an open carpal tunnel release (CTR).
Materials and Methods
Institutional Review Board (IRB) approval was granted (IRB# S12-03741) to convenience sample 225 respondents in the study setting consisting of surgical offices staffed by three fellowship trained orthopaedic hand surgeons and one Certified Hand Specialist (CHT) between December 1, 2012 and May 1, 2013. A 13-question anonymous survey was distributed by the respective office staffs and medical research assistants to willing participants. Surveys were self-administered and collected by our office staff while maintaining confidentiality.
A one-page description of carpal tunnel syndrome (CTS) including signs, symptoms, and treatment was provided prior to beginning the survey that was divided into three sections. In the first section of the survey, questions elicited demographic information including age, gender, and history of previous hand surgery, education level, annual household income, and medical insurance. In the second section, patients were asked open-ended questions that sought to identify how much they believe physicians are, and should be, compensated for performing an open CTR. The open-ended questions included the following:
-
1.
What do you think is a reasonable fee that a hand surgeon should receive to perform a carpal tunnel releases?
(The fee includes the operation itself, the time the surgeon spends with the patient at the hospital, and patient care for 90 days after surgery. The fee DOES NOT include preoperative evaluation or the fees the hospital or anesthesiologist charges.)
-
2.
What percentage of health care fees should be paid to the hand surgeon, the anesthesiologist and the hospital (or surgery center) for a carpal tunnel release? (please CIRCLE ONE number in EACH column and make sure they add up to 100 %)
Hand surgeon
+
Anesthesiologist
+
Hospital
=
100 %
0 %
+
0 %
+
0 %
=
100 %
10 %
+
10 %
+
10 %
=
100 %
20 %
+
20 %
+
20 %
=
100 %
30 %
+
30 %
+
30 %
=
100 %
40 %
+
40 %
+
40 %
=
100 %
50 %
+
50 %
+
50 %
=
100 %
60 %
+
60 %
+
60 %
=
100 %
70 %
+
70 %
+
70 %
=
100 %
80 %
+
80 %
+
80 %
=
100 %
90 %
+
90 %
+
90 %
=
100 %
100 %
+
100 %
+
100 %
=
100 %
Note: ALL three columns MUST add up to 100 %
-
3.
Compared to other common expenditures such as household items and electronics, where do you value a carpal tunnel release? (Fig. 1)
Fig. 1 
Compared to other common expenditures such as household items and electronics, where do you rate the value of a carpal tunnel release?
-
4.
How much do you estimate that Medicare actually pays a hand surgeon for performing a carpal tunnel release and 90 days of care following surgery?
(The fee includes the operation itself, the time the surgeon spends with the patient at the hospital, and patient care for 90 days after surgery. The fee DOES NOT include preoperative evaluation or the fees the hospital or anesthesiologist charges.)
In the final section, participants were given the amount of the actual Medicare allowable reimbursement [3] for performing an open CTR and were then asked their opinions on this amount using a Likert scale. This question was on a separate page of the study so as not to influence the preceding open-ended questions. The question was asked as follows:
-
5.
On average, Medicare pays a hand surgeon $412.33 for performing a carpal tunnel release. Please indicate your feeling about this fee (check one).
☐$412.33 is much lower than what a hand surgeon should earn for a carpal tunnel release.
☐$412.33 is somewhat lower than what a surgeon should earn for a carpal tunnel release.
☐$412.33 is about right for what a surgeon should earn for a carpal tunnel release.
☐$412.33 is somewhat higher than what a surgeon should earn for a carpal tunnel release.
☐$412.33 is much higher than what a surgeon should earn for a carpal tunnel release.

Finally, patients were given the opportunity to provide additional optional comments.
The collected data was then screened for the assumptions of parametric statistics. Statistical comparisons between patients’ perceptions of what a surgeon should be paid and what they are actually paid were made using a combination of dependent t tests, analysis of variance (ANOVA) with post hoc Bonferroni, and chi-square for dichotomous and categorical variables, as appropriate. The statistical package used for data analysis was IBM SPSS Statistics-Version 20 (IBM SPSS Inc., Chicago, IL).
Results
A total of 225 questionnaires were completed by 114 males (x̅ = 42.1 ± 14.4 years) and 110 females (x̅ = 44.9 ± 15.6 years) and one respondent that did not indicate gender. There is a significant difference between males ($4860 ± 4579) and females ($8182 ± $14,243) with regard to what a reasonable fee a hand surgeon should receive to perform a CTR (p = 0.02). There is not a significant difference between males and females with regard to what Medicare actually reimburses (p = 0.32).
Ages of respondents were evenly distributed over a range of 18–80 years old with a mean age of 43.4 ± 15 years. Among descriptive calculations using chi-square analysis with age treated as a categorical variable across 10-year intervals (20–29, 30–39, 40–49, 50–59, 60–69, 70+), no significant differences were found between respondent age and what a reasonable fee a hand surgeon should receive to perform a CTR (p = 0.91).
One third (76 respondents) of the surveys were distributed in the offices of CHTs whereas two thirds (149) of the surveys were distributed at hand surgeon’s offices. Questionnaire completion based on two geographic locations was not statistically significant (p = 0.32).
Just over a quarter (27 %) of the respondents had previous hand surgery, and there was a significant difference (p < 0.001) between those who previously had hand surgery ($8535 ± $13,764) and placed an additional value of approximately $3000 to the procedure compared to those who had not previously had hand surgery ($5677 ± $8851).
Sixty-nine percent of the respondents had a 4-year college education or graduate degree. ANOVA comparing education level with a reasonable fee did show statistical significance following a Bonferroni post hoc comparison between respondents with no high school degree and high school graduates (p = 0.025), some college (p = 0.011), a 4-year degree (p = 0.001), and those with a graduate degree (p = 0.002). There were no statistical differences (p > 0.05) when comparing high school graduates with other levels of higher education (Table 1).
Seventy-two percent of respondents earned an annual income of greater than $75,000. When categorical variables were compared, there were no statistically significant differences between respondent income and a reasonable fee paid to a hand surgeon for performing an open carpal tunnel release (p = 0.30). There was also no difference between respondent income and the percentage of fee paid to the surgeon (p = 0.95). Sixty-three percent of the respondents had private insurance whereas only 10 % had Medicare coverage. ANOVA compared insurance type and reasonable fee and found no statistical differences (p = 0.10).
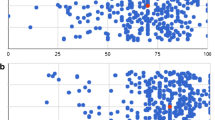
Respondents believed that the percentage of the fee appropriate for the hand surgeon should be 56 % followed by the anesthesiologist (23 %) and finally the hospital or surgery center (21 %). When compared to actual distribution of funds at our hospital, there is a threefold difference in respondent’s perceptions and how health care dollars are actually distributed (Fig. 2).

a Respondents’ perceptions of how health care fees should be distributed for performing an open CTR. b Actual distribution of health care reimbursements for performing an open CTR
Overall, respondents believed that a reasonable fee that a hand surgeon should receive to perform a open CTR was on average $6279 with a range of $80–$100,000 (Fig. 3). When outliers (defined as responses falling greater than 2 standard deviations from the mean) were removed from the analysis, the average was $5030 with a range of $80–$20,000.

What do you think is a reasonable fee that a hand surgeon should receive to perform a carpal tunnel release? When outliers are eliminated from this evaluation the mean becomes $5030 with a range of $80–$20,000
Compared to other common expenditures, >55 % of respondents indicated that the value of performing an open CTR was worth more than a year’s supply of gasoline. Approximately 85 % of respondents indicated that the value of performing an open CTR was worth more than an iPad or $600 (Fig. 4).

Compared to other common expenditures such as household items and electronics, where do you rate the value of a carpal tunnel release?
Respondents thought that Medicare actually pays hand surgeons $3474 ($100–$50,000) to perform an open CTR (Fig. 5). When outliers were removed from the analysis, the average was $2685 with a range of $100–$12,000. When asked to compare the actual Medicare reimbursement to the patient’s perceptions, 84 % indicated that the reimbursement rate was “much lower” or “somewhat lower” than what was reasonable (Fig. 6).

How much do you estimate that Medicare pays a hand surgeon for performing a CTR and 90 days of care following the surgery?

On average, Medicare pays a hand surgeon $412.33 for performing a carpal tunnel release. Please indicate your feeling about this fee
Of the 225 respondents, 45 wrote additional and optional comments. The majority (53 %) of the additional responses were considered neutral with regard to physician reimbursement. Respondents indicated that they wish they had more information to answer the survey. Representative comments include, “You left out crucial information—how long does this surgery take, how extensive is it?—In order to figure out the right cost, this matters a great deal” and “I would have a better perception if you can stated how long the surgery actually takes to perform the procedure.” Other responses considered neutral simply acknowledged the respondents lack of education regarding physician reimbursement. For example, “I have little knowledge in this area” and “I am obviously not familiar with such costs.”
Forty percent of the respondents had additional comments indicating that Medicare reimbursements were too low. Representative comments include, “Hard to believe payment is sooo low. Very undervalued!” “Surprised to see that the price paid to the ones that save one of the most important tools your body uses is that low. Your hands are priceless. This low fee is almost hard to believe,” “Way to low a fee. Any patient will tell you after a successful operation HEALTH IS PRICELESS” and “I can’t believe the fee indicated is correct. I hope I receive any medical attention I need before I reach the point of Medicare.”
Three respondents wrote additional comments indicating that they felt the current rate of Medicare reimbursement is about right or possibly too high. These comments were, “Considering what I get paid for my job expertise—if we were to level the playing field—maybe $412.00 for an hour’s work (surgeon only) is fair,” “If [the hand surgeon] can do 3 a day, then $412.33 is fair.” Finally, one respondent commented that, “Hand surgeons probably don’t starve.”
Discussion
On March 23, 2010, Barack Obama signed into law the Patient Protection and Affordable Care Act (PPACA), commonly referred to as the Affordable Care Act (ACA). Much debate ensued over the constitutionality of the PPACA that was ultimately decided by a narrow margin. On June 28, 2012, the case of National Federation of Independent Business versus Sebelius was decided by the US Supreme Court which is the landmark case upholding the constitutionality and the vast majority of the provisions outlined in the PPACA. Although currently accepted as law, there is still much unclear about how the ACA will be implemented.
Important to this discussion is how the public perceives physician reimbursement for outpatient surgical procedures. The average age of patients with symptomatic CTS is age 50 [8] and lays outside the provisions of Medicare. It is important to note that most private insurance companies base their physician reimbursement schedules on those of Medicare, although based on the surgical practice and geographic location, some patients may be paying more and some less for the same procedure. Hence, the implications of what happens at the federal level is not reserved for those over the age of 65.
The rates of Medicare reimbursements have fallen over the past decade while the percentage of federal expenditure has been increasing [2]. In 2013, 24 % of federal spending is budgeted for health care. This number is expected to increase to 28 % by 2016 [7]. It is clear that health care costs are skyrocketing. However, it is clearly not due to increasing physician reimbursement.
Our respondents indicated that physicians (surgeons and anesthesiologist) should command most (79 %) of the health care funds allocated to performing a CTR. When comparing these perceptions to actual reimbursement at a local hospital, we find that a drastic disparity exists between perception and reality. The hospital commands 70 % ($1267) of the Medicare reimbursement for performing a CTR compared to 23 % ($412) to the surgeon and 7 % ($120) to the anesthesiologist. Medicare reimbursement to the facility and physicians totals around $1800. This value is far smaller than our respondents believe reimbursement to the surgeon for actually performing a CTR is worth. Our data was acquired in an academic center where reimbursements could be obtained for the individual services. This data may not be generally applicable to physician’s working in private practice where surgeons bill independently from the hospital and surgery centers. Moreover, some surgeons have financial interest in a surgery centers which would also influence total surgeon reimbursement. This study demonstrates that our patients place a significant value on the services hand surgeons provide.
Our respondents believed that hand surgeons should be reimbursed >12 times ($5030) that of Medicare reimbursement (~$412) for performing an open CTR. Moreover, respondents overestimated Medicare reimbursement by greater than sixfold ($2685). Finally, 84 % of respondents felt that the hand surgeon’s reimbursement by Medicare was “somewhat lower” or “much lower” than it should be.
Fowler and Buterbaugh [4] reported that respondents of a similar survey indicated that “reasonable surgeon fee” for performing a CTR was $2630 ± $3058. Moreover, they reported that the respondent’s perception of Medicare reimbursement for a CTR was $1892 ± $4180. Our study demonstrates an even larger discrepancy in our patient’s perceptions and actual physician reimbursements. Our patient population valued a CTR almost two times more than those in Fowler’s study and overestimated Medicare reimbursements 30 % higher.
This study has several limitations. The surveys were given to willing respondents in the waiting rooms prior to seeing a hand surgeon or a CHT; therefore, self-selection bias may have been an unintentional consequence. The patients in this sample may not be representative of the general population due to higher income and educational levels. Although instructions were specific about anonymity, patients may have answered how much their hand surgeon should be paid as opposed to how much a hand surgeon should be reimbursed to perform an open CTR. We attempted to negate this bias by including the CHT offices as a setting to distribute the survey and demonstrated that statistical differences (p ≥ 0.05) did not exist between respondents who answered the survey in the hand surgery offices and the offices of CHTs. We are unable to control for geographic bias, however. Although we have a large referral radius, our respondents are from a relatively small geographic area. Therefore, our results may not be generalizable to all regions of the USA.
The design of the non-validated survey and order of questions may have introduced some bias, although based on experience, the survey questions were non-ambiguous and simple to answer. First, we asked questions about a reasonable fee that a hand surgeon should receive to perform a CTR followed by how health care fees should be distributed and ultimately asked how the respondent values the CTR compared to other common expenditures. All these questions are based on personal opinions and do not require specific knowledge of health care policies or reimbursement schedules. These questions were followed by a question that can be misinterpreted as one requiring specific knowledge of Medicare reimbursement when asked how much Medicare actually pays for a CTR. Respondents may perceive that there is a right or wrong answer. Moreover, they may reflexively provide a response that is necessarily less than their opinion of how reimbursements should be distributed. Finally, it was possible to skip to the end of the survey to “discover” how much Medicare reimburses for a CTR. While providing a separate survey indicating the amount of the Medicare reimbursement would have provided a “fool-proof” way to insure questions were answered in consecutive order, we did not think this element was crucial to the study. Moreover, it added an additional layer of complexity for the office staff that we did not think was warranted.
With these limitations in mind, our results are quite compelling. Our respondents believed that hand surgeons should be reimbursed >12 times that of the Medicare reimbursement rate for performing an open CTR. Moreover, respondents overestimated Medicare reimbursement by greater than sixfold. These results underscore the drastic disparity between respondents’ perceptions of surgeon reimbursement for performing the most common surgery of the hand [9].
This study demonstrates that patients perceive a significant value in the services we provide. Patients should be educated on the disparity of health care costs and physician reimbursements for these life-altering procedures.
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study. The authors declare that they have no conflict of interest. IRB approval was obtained for the human research conducted in this study.
References
Bozic KJ, Cramer B, Albert TJ. Medicare and the orthopaedic surgeon: challenges in providing, financing, and accessing musculoskeletal care for the elderly. J Bone Joint Surg Am. 2010;92(6):1568–74.
Federal Budget Spending Estimates for Fiscal Years 2011 – 2016. http://www.usgovernmentspending.com/federal_budget_detail_fy12bs12016n
Find A Code LLC. http://www.Findacode.Com 2013.
Fowler JR, Buterbaugh GA. Patient perception of physician reimbursement for common hand surgical procedures. Orthopedics. 2013;36(9):e1149–54.
http://ycharts.com/indicators/us_health_care_inflation_rate.
Iglehart JK. Medicare’s declining payments to physicians. N Engl J Med. 2002;346(24):1924–30.
Pomerance J, Zurakowski D, Fine I. The cost-effectiveness of nonsurgical versus surgical treatment for carpal tunnel syndrome. J Hand Surg [Am]. 2009;34(7):1193–2000.
Truffer CJ, Keehan S, Smith S, et al. Health spending projections through 2019: the recession’s impact continues. Health Aff (Millwood). 2010;29(3):522–9.
Author information
Authors and Affiliations
Corresponding author
About this article

Cite this article
Kokko, K.P., Lipman, A.J., Sapienza, A. et al. “Hand surgeons probably don’t starve”: Patient’s perceptions of physician reimbursements for performing an open carpal tunnel release. HAND 10, 773–778 (2015). https://doi.org/10.1007/s11552-015-9774-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11552-015-9774-7