
Abstract
Background
Collision sport participation rates among high school youth in Canada are high. While participation is beneficial for physical and mental well-being, the rates of injury in these sports are high.
Aims
This study aims to compare injury rates and profiles across four common youth collision sports (ice hockey, tackle football, lacrosse, rugby).
Methods
Data from a cross-sectional questionnaire of 2029 high school youth were used to identify male collision sport participants to be included in this secondary analysis (n = 360).
Results
Of the 2029 students who completed the questionnaire, 360 participated in collision-based sports [Ages: 14 (5%), 15 (41%), 16 (25%), 17 (26%), 18 (3%)]. The rates of injury ranged from 12.7 injuries/100 participants/year (rugby) to 33.1 injuries/100 participants/year (ice hockey). Concussion rates ranged from 12.4 (football) to 15.8 (ice hockey) concussions/100 participants/year. Similarities existed in the profile of injuries between sports, with most injuries occurring due to contact with another player (range 57.0% to 87.5%). Injuries to the head (33.3%), wrist/hand (16.0%), shoulder (12.8%), and knee (12.0%) were the most prevalent injury type. Substantial differences in previous playing experience existed between sports.
Discussion
The high rate of injury and concussion reported across each of these sports highlights the need for the introduction of primary prevention strategies in these sports aimed to reduce the risk of injury.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sports participation in youth is associated with physical and mental well-being [1]. It is also recognised that sport participation carries with it a heightened risk of injury [2]. In particular, many popular collision sports (e.g., ice hockey, tackle football, rugby, and lacrosse) have demonstrated a high risk of injury [3]. Despite this high risk, participation in collision sports has grown in recent years, with Black et al. [4] reporting ice hockey as the second most common boys sport (20.5 participants/100 students/year) in a sample of high school students in Alberta, following basketball (33.1 participants/100 students/year). Canadian tackle football (football) was also among the most common sports while rugby was popular for males in a school setting [4]. Although lacrosse did not feature among the most popular sports, it represented the sport with the second highest rate of injury among boys [(27.6/100 participants/year (95% CIs 14.0–47.0)], surpassed only by ice hockey. These four collision sports not only present a high risk of all injury types, but also concussion specifically, with rugby, ice hockey, football, and lacrosse demonstrating the highest rates of concussion across 12 youth sports [5].
Injury prevention models have previously demonstrated the need for epidemiological studies to establish injury rates and risk factors in different sport settings to inform the development and evaluation of injury prevention strategies [6, 7]. Understanding injury rates allows stakeholders to prioritize the allocation of resources to high-risk sport populations and understanding mechanisms of injury will inform targeted injury prevention strategies. Previously, primary prevention strategies including rule changes, [8,9,10] equipment recommendations [11] and neuromuscular warm-up programs [12] have been used effectively to lower the risk of concussions and musculoskeletal injuries among youth athletes.
Ice hockey and football are collision sports that have received a relatively great deal of attention in the injury prevention literature [3]. The recent increased popularity of rugby and lacrosse in Alberta, support the need for further epidemiological investigation to inform a greater understanding of potential injury prevention strategies to ensure the safety and long-term welfare of collision sport participants in Alberta. Furthermore, recent studies in this setting have demonstrated high rates of injury [4], particularly in collision-based sports for females [13, 14] which highlights the need for a greater understanding of collision sports in a youth male context. Therefore, the objective of this study is to explore further the etiology of injury in collisions sports (e.g., ice hockey, football, lacrosse, rugby) in Alberta, Canada.
Methods
Study design and participants
This secondary analysis of a cross-sectional study was designed to capture participation, injury, and concussion rates as well as examine mechanisms and potential risk factors across youth sport in Alberta, Canada. This secondary analysis specifically targeted male collision sports (i.e., ice hockey, football, lacrosse, rugby) from a larger cohort (n = 2029) of high school students [15]. Thirty-three high schools across eight school boards and five private schools were contacted to take part in the study across both rural and urban sites. Research assistants assisted in the supervision of high school student web-based online survey completion using iPads or school computers. The study was approved by the Conjoint Health Research Ethics Board at the University of Calgary (REB17-1948), the Health Research Ethics Board at the University of Alberta (REB Pro00080524) and all participating school boards. Both parent and/or player consent (mature minor > 12 years) as well as player assent was obtained for each participant.
Outcome measures
The study consisted of an anonymous survey including 180 questions (excluding subsequent branching questions) which took ~ 45 min to complete. Questions pertaining to participant demographics, sports activities, sport specialisation, previous injury education, sport safety practices, lifestyle choices, sport and recreation (S&R)-related concussions, and non-S&R concussions were included. Furthermore, participants were asked to report which injury they considered to be their most serious injury in the past year (injury rates reported based on most serious injury), with more detailed information captured on this specific injury. This survey was adapted from one previously used within this cohort [3]. Content validity was assessed through expert consultation, while face validity was assessed by a varsity athlete, parent, and six adolescents (grade 10–12, three boys, three girls). This process led to the addition of questions specific to S&R related concussions (concussion rates based on at least one concussion per student) as well as sport specialisation. The second iteration of the survey was assessed for face validity based on the review of four further researchers and pilot tested in one high school (n = 143), which resulted in no further changes.
Analysis
From the initial sample of participants (n = 2029), to be included in this secondary analysis, players must have identified as being male and responded that they participated in at least one of the four collision sports captured by the study (i.e., ice hockey, football, lacrosse, rugby). All data analysis was undertaken using statistical software Stata (StataCorp, 2019, Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC). Descriptive characteristics for players meeting these criteria were captured, including demographics, injury, and concussion rates within the past year. Participation rates within this study were captured as a proportion of the entire sampled population. All participant responses were cross-checked with other associated variables to assess accuracy of responses. Sport specific injury rates (# injuries/100 participants/year) were estimated with corresponding 95% confidence intervals calculated using Stata’s robust cluster variance estimator to adjust for cluster by school. Epidemiological data pertaining to each injury was reported as proportions for each sport including mechanism, location, and type of injury as well as information surrounding the activity during injury and years of playing experience. Missing data due to non-response was reported as a proportion of all responses in each corresponding table.
Results
Of the 63 school administrators who were approached to participate, 24 (38%) agreed, from which 2029 individuals completed the survey. Of these, 958 (47%) were male and 360 (37.6% of male participants) indicated they played at least one collision sport. Participant demographics for this subgroup are reported in Table 1.
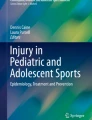
Ice hockey was the most popular collision sport played with 196/958 male students participating [20.5% (95% CI 14.9–27.3)]. In the other collision sports 161/958 played football [16.8% (95% CI 13.4–20.9)], 63/968 played rugby [6.6% (95% CI 4.1–10.3)] and 29/968 played lacrosse [3.0% (95% CI 2.0–4.5)]. Years of sport-specific playing experience are reported in Fig. 1. In ice hockey, 86% had participated for 5 years or more and in lacrosse it was 72%. Comparatively, only 26% of football players and 10% of rugby players had 5 or more years of previous playing experience.

Years of playing experience observed for boy’s collision sports
There were 365 serious injuries reported across all boys in the study. Of these, 33% of injuries were caused by collision sports (ice hockey: 17%, football: 11%, lacrosse: 3%, rugby 2%). Ice hockey not only represented the sport with the greatest proportion of injuries, but also represented the sport with the highest injury rate [33.1/100 participants/year (95% CI 24.2–36.7)]. This was followed by lacrosse [27.6/100 participants/year (95% CI 14.0–47.0)], football [21.1/100 participants/year (95% CI 15.6–27.9)] and rugby [12.7/100 participants/year (95% CI 5.5–26.7)].
Concussion
The most common site of injury in all collision sports was the head/face, accounting for the most injuries in rugby (50.0%) and the lowest proportion in football (24.4%: Table 2). Concussion (or being “knocked out”) was reported as the most common injury type in rugby (50.0%) and football (24.4%) based on most serious injury reported in the past year. Fractures were reported as the most common injury type in lacrosse (44.4%) and ice hockey (27.0%) (Table 3). Ice hockey had the highest rate of concussion 15.8/100 participants/year (95% CI 11.8–20.9) followed by lacrosse [13.8/100 participants/year (95% CI 5.3–31.5)], rugby [12.7/100 participants/year (95% CI 5.7–25.8)] and football [12.4/100 participants/year (95% CI 7.7–19.5)].
Contact with another player was the primary mechanism of serious injury across all four sports, accounting for a range between 57.0% in ice hockey to 87.5% in rugby (Fig. 2). Of these injuries, the majority were caused by a player who was bigger than the injured player in rugby (57.1%), lacrosse (50.0%) and football (44.8%), while in ice hockey most were caused by someone who was of similar size (50.0%: Fig. 3).

Injury mechanisms observed in boy’s collision sports. 4.9% missing in football. No missing in hockey, lacrosse or rugby

Relative size of the player causing an injury for boy’s collision sports. 5.5% missing in hockey. No missing in football, lacrosse or rugby
Most injuries occurred during competition across each of the four collision sports, followed by training (Fig. 4). Several injuries in each sport occurred during recreational participation (football: 10.2%, ice hockey: 7.0%, lacrosse: 6.3%). Most game-related injuries occurred during the middle of the game across all sports (Table 4).

Sport environment of injuries observed in boy’s collision sports. 2.8% of hockey responded “Unsure”. No respondents reported “other” or “missing”. Participants could select more than one response
Discussion
Collision sports are associated with high rates of both injury and concussion for male high school aged sports participants, with rates ranging from 12.7 injuries/100 participants/year (rugby) to 33.1 injuries/100 participants/year (ice hockey) for all injury types, and 12.4 concussions/100 participants/year (football) to 15.8 concussions/100 participants/year (ice hockey). These four collision sports account for 33% of all injuries to high school boys in Alberta, of which the majority come from ice hockey and football (28%). Years of previous playing experience varied greatly between sports, with most ice hockey and lacrosse players having over 5 years’ experience, while most rugby and football players had less than 5 years’ experience. Concerningly, injuries to the head were common across all four sports, accounting for an average of one third of all injuries in these sports (range: 24–50%), with the majority of these injuries being concussions. Unsurprisingly, given the nature of these sports, 95.8% of injuries occurred due to contact (70.5% contact with another person) and most injuries occurred during game play or competition when exposure to these contact events is likely more regular and with higher intensity than training. The high rates of injury and concussion specifically demonstrate the need for further research into possible injury prevention strategies in these sports, with strategies such as injury prevention warm-up programs, equipment use, and rule change likely the most effective ways to reduce the risk [9].
Of the four collision sports within this study, ice hockey had the highest rate of injury, followed by lacrosse, football, and rugby. When compared to other sports undertaken by high school males in Alberta, these injury rates represented the first, second, third, and seventh highest risk sports [4]. It must be acknowledged that the rates presented, however, represent only those that were considered the most serious injury to have occurred within the last year and, therefore, only represent a portion of the total injury rate within each of these sports. Furthermore, although comparison of these rates to other studies in these sports is difficult due to differences in the rates presented (per 100 participants per year compared with per 1000 h or athletic exposures), these rates are high with respect to other male high school sports and require the implementation of injury prevention strategies to minimise this risk of injury.
While all injuries may be targeted for injury prevention, the rates of concussion presented within this study demonstrate the opportunity for injury prevention strategies targeted specifically at concussion in high school sport. Previously, a systematic review has highlighted there are three areas which represent the best opportunity for preventing concussion occurrence, which are: policy/law change, training programs, and protective equipment [9]. In the context of youth sport specifically, there have previously been attempts in collision sports to reduce the risk of concussions in a number of ways across multiple sports. In rugby for example, the introduction of a neuromuscular training warm-up program in rugby union demonstrated a 59% reduction in concussions in players who completed the warm-up as prescribed, three times per week [12]. Furthermore, in ice hockey, policy disallowing body checking (but continuing to permit body contact) has demonstrated a combined 70% reduction in the risk of concussion in Pee Wee (ages 11–12) youth ice hockey [incidence rate ratio (IRR) = 0.3; 95% CI 0.22–0.41] [9], with similar reductions found at the non-elite Bantam (ages 13–14) and Midget (ages 15–17) age categories [10, 16]. Adding to this evidence, follow-up studies have suggested that more years of body checking experience are not protective of concussion in youth ice hockey players playing in leagues that allow body checking, which suggests no unintended concussion consequences from these policy decisions [17, 18]. Wearing a mouthguard is associated with a 64% lower odds of concussion in ice hockey [OR = 0.36; 95% CI 0.17–0.73] [11 ] and a combined estimate across multiple contact and collision sports also suggests a protective effect [IRR = 0.8; 95% CI 0.6–1.1] [9]. Collision sports should consider implementing mouthguard policy with strict enforcement if not already mandated. In youth American football, the interventions with the strongest support for concussion prevention include reducing contact in practice and contact training [19]. For instance, a policy restricting contact in practices to 60 min a week after the third week of the season was associated with a reduction in practice-related concussion by 54% [P = 0.003; [20]]. However, some primary prevention strategies have not been as successful in reducing the risk of concussion such as Hockey Canada’s 2011 “zero tolerance for head contact” [21]. Despite this, it is recognised that in the last decade our understanding and knowledge surrounding concussion has drastically improved, meaning that the increase in concussion rates globally may be driven by awareness rather than an increase in risk itself [22]. The attention drawn to the injury by high profile cases of both professional players [23] and youth [24] has meant that training and education has proliferated to enable early recognition and treatment of this serious injury across all sports, and in particular, collision sport.
Given the high rates of concussion in each of the four sports, it is unsurprising that injuries to the head accounted for the highest proportion of all injuries (33.3% of all injuries). This ranged from 24.4% of injuries in football to 50.0% of all injuries in rugby (Table 2). The proportion of injuries occurring to body location differed among sports, but overall, the wrist/hand was the second most injured site (16.0%), followed by the shoulder (12.8%) and knee (12.0%). The injuries reported here are only those that were deemed to be the most serious by the participants, and, therefore, the distribution of injury across body sites differed slightly to what has previously been seen for some injuries. In ice hockey, which was the sport with the highest participation rates, the proportion of injuries to the wrist/hand/finger were higher than previously reported [22.2% compared with 6.7% [3]] but the profile of other injured sites was similar [3, 25]. In the second highest participation sport, football, the proportion of head injuries was higher than previously reported in a similar population [24.4% vs. 14.9%] [3] and a US high school population [12.9%] [26]. The proportion of shoulder [3] and knee [3, 26] injuries were similar to the current study, however, ankle injuries accounted for twice as many injuries in this study compared to a similar sample [14.6% vs 7.8% [3]]. Furthermore, as with ice hockey, the proportion of wrist/hand injuries was substantially higher than previously reported in a similar sample. [19.5% vs 8.5%] [3]. The distribution of injuries across body sites for lacrosse and rugby differed in this study with those previously reported, with Kerr et al. [27] reporting head injuries to account for 11% of all injuries, compared with 33% in this study, while in rugby union, a recent review reported injuries to the head to account for between 9 and 41% of all injuries [28]. Importantly, however, there were only a small number of reported injuries in these sports and included only those classed as the most serious that had occurred that year, which means that the distribution of injuries across the different sites may not be reflective of all injuries occurring in these sports and may be an underestimate of site-specific rates.
One of the striking differences between sports was the years of playing experience among the participants. Most ice hockey and lacrosse players reported higher levels of experience, with 86% and 72% of players reporting greater than 5 years of playing experience, respectively. In contrast, only 25% of football players reported more than 5 years of experience and just 12% of rugby players. In fact, 21% of football participants and 25% of rugby participants reported less than 1 year of previous experience at the time of the study. A recent study in a similar female Canadian youth rugby population has even suggested that as many as 43% of players have no previous playing experience when exposed to rugby in Alberta [14]. Within collision sports, the ability to perform a safe and effective tackling technique is a key attribute for participants of all ages. For example, in rugby, Burger et al. [29] have shown that higher criterion-specific tackle-related technique scores were associated with a non-injury outcome in under 18s players. Given that most players in both rugby and football had a low level of previous experience, the players may not have developed efficient tackle proficiency, therefore, potentially leaving them at a higher risk of injury. However, previous research in football has shown that players with greater levels of experience are at a higher risk of injury than less experienced players [30].
Although this study did not examine the specific events by which injury occurred, the participants did report that 70.5% of all injuries occurred due to contact with another person. The majority of injuries being caused by contact are similar to that which is reported previously in football [26], ice hockey [25] and rugby [28]. In lacrosse, contact with another player accounted for 45% of injuries [31] compared with 66.7% of injuries in this study. Of the serious injuries that were reported by the participants to have been caused by contact with another person, on average, 49.2% of the injuries were caused by a participant that was reported as bigger than the injured participant (Fig. 2). The substantial number of players being injured by larger players may be indicative of size disparity between players that participate in collision sports. To combat this issue, there have been efforts to group players based on their maturity status and size as opposed to their biological age in many sports [32]. In rugby and football for example, several leagues and countries have adopted weight restrictions for certain age groups, however, there are challenges associated with this approach [33, 34].
When comparing injury proportions occurring in different formats, competitive fixtures accounted for the most injuries, ranging from 44.9 to 85.7% of all injuries (Fig. 4). Of these match injuries, the highest proportion occurred in the middle of the match (63.0–79.0%). The second largest proportion of injuries came from practice/training sessions, accounting for between 0 and 34.7% of injuries. When comparing different collision sports, rugby demonstrated the highest proportion of match injuries (85.7%) while football demonstrated the highest proportion of training injuries (34.7%). Given the exposure to training is often far greater than that of competition, when comparing incidence rates between different exposure types (match vs training), often a low incidence does not reflect the high proportion of injuries occurring during training [35 ]. Therefore, it is important to recognise that a substantial proportion of injuries occur during training and thus provide a good opportunity for injury prevention strategies, as the environment can be considered more controllable than that of match play.
There are several limitations to consider when interpreting the results of this study. As with all cross-sectional self-report studies, it must be recognised that the responses provided by the participants may be limited by recall bias. Furthermore, given that this is a study regarding sports participation and injuries, there may be some selection bias in the sample, i.e., the survey may have been completed by those who have an interest in sport or may have been affected by a recent injury. This may have led to an overestimation of the rates of participation and injury in these groups. However, it is also possible that there may be some degree of underestimation as participants were asked to only state their top 3 sports, and if they partook in more than this, they were unable to list participation in any further sports. In the injury rates provided, these sport-specific rates represented injuries that were considered the most serious injury of all injuries that may have occurred, meaning that they may not reflect a true rate of injury in each respective sport. Further, as no individual exposure to each sport was obtained, the presentation of rates was per 100 participants per year. Finally, it must also be recognised that 79% of the respondents to the questionnaire were from urban centres and, therefore, the generalisability of these findings to smaller, more rural, or indigenous populations is limited.
Conclusions
This study has demonstrated the high rates of all injury and concussion in boy’s collision sports. This is particularly noteworthy when it is considered that these four sports contribute 33% of all serious injuries to this population. While there are common features to the profile of injuries across these sports (for example the high proportion caused by contact and high number to the head), it is also apparent that there are individual differences between each sport which must be considered when implementing prevention strategies. In the context of youth collision sport, a wide range of variation exists in player experience and given the high proportion of injuries attributed to contact, it may be important to implement injury prevention interventions which are specific to the experience level of the player and address potential differences in contact proficiency. Overall, this study demonstrates the potential need for primary prevention strategies in youth collision sport to maintain the welfare of the participants.
References
Briere FN, Imbeault A, Goldfield GS, Pagani LS (2020) Consistent participation in organized physical activity predicts emotional adjustment in children. Pediatr Res 88:125–130
Billette J, Janz T. Injuries in Canada: insights from the Canadian Health Survey. Statistics Canada Catalogue no.82-624-X
Emery CA, Meeuwisse WH, McAllister JR (2006) Survey of sports participation and sports injury in calgary and area high schools. Clin J Sports Med 16:20–26
Black AM, Meeuwisse DW, Eliason PH, Hagel BE, Emery CA (2021) Sport participation and injury rates in high school: a Canadian survey of 2029 high school students. J Safety Res 78:314–321
Pfister T, Pfister K, Hagel B, Ghali WA, Ronksley PE (2016) The incidence of concussion in youth sports: a systematic review and meta-analysis. Br J Sport Med 50:292–297
Van Mechelen W, Hlobil H, Kemper HCG (1992) Incidence, severity, etiology and prevention of sports injuries. Sports Med 14(2):82–99
Finch C (2006) A new framework for research leading to sports injury prevention. J Sci Med Sport 9(1–2):3–9
Black AM, Hagel BE, Palacios-Derflingher L, Schneider KJ, Emery CA (2017) The risk of injury associated with body checking among Pee Wee ice hockey players: an evaluation of Hockey Canada’s national body checking policy change. Br J Sports Med 51(24):1767–1772
Emery CA, Black AM, Kolstad A, Martinez G, Nettel-Aguirre A, Engebretsen L et al (2017) What strategies can be used to effectively reduce the risk of concussion in sport? A systematic review. Br J Sports Med 51:978–984
Emery C, Palacios-Derflingher L, Black AM, Eliason P, Krolikowski M, Spencer N et al (2020) Does disallowing body checking in non-elite 13- to 14-year-old ice hockey leagues reduce the rates of injury and concussion? A cohort study in two Canadian provinces. Br J Sports Med 54:414–420
Chisholm DA, Black AM, Palacios-Derflingher L, Eliason PH, Schneider K, Emery CA et al (2020) Mouthguard use in youth ice hockey and the risk of concussion: nested case-control study of 315 cases. Br J Sports Med 54:866–870
Hislop MD, Stokes KA, Williams S, McKay CD, England ME, Kemp SPT et al (2017) Reducing musculoskeletal injury and concussion risk in schoolboy rugby players with a pre-activity movement control exercise programme: a cluster randomised controlled trial. Br J Sports Med 51(15):1140–1146
Cairo AL, Raisanan AM, Shill IJ, Black AM, Emery CA (2022) High injury and concussion rates in female youth team sport: an opportunity for prevention. Int J Sports Med 43:608–615
Shill IJ, West SW, Sick S, Schneider K, Hagel BE, Pasenan K et al (2021) Injuries and concussions in female high school rugby: prevention is worth a try. Clin J Sports Med. https://doi.org/10.1097/JSM.0000000000000993. Online ahead of print
Black AM, Meeuwisse D, Eliason PH, Hagel BH, Emery CA (2020) Sport participation and injury rates in high school: a survey of 2029 high school students. Clin J Sports Med 30:e111–e117
Emery C, Eliason P, Warriyar V, Palacios-Derflingher L, Black AM, Krolikowski M et al (2022) Body checking in non-elite adolescent ice hockey leagues: it is never too late for policy change aiming to protect the health of adolescents. Br J Sports Med 56:12–17
Emery C, Kang J, Shrier I, Goulet C, Hagel B, Benson B et al (2011) Risk of injury associated with bodychecking experience among youth hockey players. Can Med J Assoc 183:1249–1256
Eliason P, Hagel B, Palacios-Derflingher L, Vineetha Warriyar KV, Bonfield S, Black AM, et al (2022) No association found between body checking experience and injury or concussion rates in adolescent ice hockey players. Br J Sports Med. https://doi.org/10.1136/bjsports-2021-104691. Online ahead of print
Pankow MP, Syrydiuk RA, Kolstad AT, Hayden AK, Dennison CR, Mrazik M, et al (2021) Head games: a systematic review and meta-analysis examining concussion and head impact incidence rates, modifiable risk factors and prevention strategies in youth tackle football. Sports Med. 52(6):1259–1272. https://doi.org/10.1007/s40279-021-01609-4
Pfaller AY, Brooks MA, Hetzel S, McGuine TA (2019) Effect of a new rule limiting full contact practice on the incidence of sport-related concussion in high school football players. Am J Sports Med 47:2294–2299
Krolikowski MP, Black AM, Palacios-Derflingher L, Blake TA, Schneider KJ, Emery CA (2017) The effect of the “zero tolerance for head contact” rule change on the risk of concussions in youth ice hockey players. Am J Sports Med 45:468–473
Stephen W West, Matthew Cross, Grant Trewartha, Aileen Taylor, John Brooks, Simon Kemp, Duncan Locke, Osman Ahmed & Keith Stokes (2021) Trends in match concussion incidence and return-to-play time in male professional Rugby Union: A 16- season prospective cohort study, Brain Injury, 35:10, 1235–1244, https://doi.org/10.1080/02699052.2021.1972142
Boylen R (2017) A look at Sidney Crosby's NHL concussion history sportsnet.ca2017. Accessed: 02 Dec 2020. https://www.sportsnet.ca/hockey/nhl/look-sidney-crosbys-nhl-concussion-history/
Mickool S (2018) The story behind the Zackery Lystedt Law seattlemag.com2018. Accessed: 02 Dec 2020. https://www.seattlemag.com/article/story-behind-zackery-lystedt-law
Matic GT, Sommerfeldt MF, Best TM, Collins CL, Comstock RD, Flanigan DC (2015) Ice hockey injuries among United States high school athletes from 2008/2009–2012/2013. Sports Med 43:119–125
Badgeley MA, McIlvain NM, Yard EE, Fields SK, Comstock RD (2013) Epidemiology of 10,000 high school football injuries: Patterns of injury by position played. J Phys Act Health 10:160–169
Kerr ZY, Caswell SV, Lincoln AE, Djoko A, Dompier TP (2016) The epidemiology of boys’ youth lacrosse injuries in the 2015 season. Injury Epidemiol 3:1–15
Leahy TM, Kenny IC, Campbell MJ, Warrington GD, Cahalan R, Harrison AJ, et al (2020) Injury surveillance and prevention practices across Rugby schools in Ireland. Phys Therapy Sport 43:((Leahy, Kenny, Campbell, Warrington, Harrison, Lyons, Comyns) Department of Physical Education and Sport Sciences, University of Limerick, Limerick, Ireland(Kenny, Warrington, Cahalan, Comyns) Health Research Institute, University of Limerick, Limerick, I):134–142
Burger N, Lambert MI, Viljoen W, Brown JC, Readhead C, Hendricks S (2016) Tackle technique and tackle-related injuries in high-level South African Rugby Union under-18 players: real-match video analysis. Br J Sports Med 50(15):932–938
Stuart MJ (2005) Gridiron football injuries. Epidemiol Pediatr Sports Inj 49:62–85
Pierpoint LA, Lincoln AE, Walker N, Caswell SV, Currie DW, Knowles SB et al (2019) The first decade of web-based sports injury surveillance: descriptive epidemiology of injuries in US High School Boys’ Lacrosse (2008–09 Through 2013–2014) and National Collegiate Association Men’s Lacrosse (2004–2005 Through 2003–2014). J Athl Train 54:30–41
Cumming S, Lloyd R, Oliver J, Eisenmann J, Malina R (2017) Bio-banding in sport: application to competition, talent identification, and strength and conditioning of youth athletes. Strength Cond J 39:34–47
World Rugby. Weight consideration guideline playerwelfare. Accessed: 02 Dec 2020. https://playerwelfare.worldrugby.org/?subsection=64
Kerr ZY, Marshall S, Simon JE, Hayden R, Snook E, Dodge T, et al (2015) Injury rates in age-only versus age-and-weight playing standard conditions in American Youth Football. Orthop J Sports Med 3 (9). https://doi.org/10.1177/2325967115603979
West SW, Williams S, Kemp SPT, Cross MJ, McKay C, Fuller CW, et al (2019) Patterns of training volume and injury risk in elite rugby union: an analysis of 1.5 million hours of training exposure over eleven seasons. J Sports Sci. 38(3): 238–247. https://doi.org/10.1080/02640414.2019.1692415
Acknowledgements
We would like to acknowledge research coordinators (Stacy Kozak, Stephen Chaudhary, Carla van den Berg), graduate students, research assistants, school administrators, teachers, and high-school students who made this work possible. The Sport Injury Prevention Research Centre is one of the International Olympic Committee Research Centers for the Prevention of Injury and Protection of Athlete Health.
Funding
This work was supported by funds available from the International Olympic Committee and a Canadian Institute for Health Research Foundation Research Grant [C Emery PI—grant # 375089 2018]. Carolyn Emery holds a Canada Research Chair (Tier 1) in Concussion.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
No potential conflict of interest was reported by the authors.
Ethical approval
Ethical approval was granted by the Conjoint Health Research Ethics Board at the University of Calgary (Ref: REB17-1948), the Health Research Ethics Board at the University of Alberta (Ref: REF Pro00080524) and all participating school boards.
Informed consent
Both parent and or player informed consent (mature minor >12 years) as well as player assent was obtained for each participant.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
West, S.W., Pankow, M.P., Gibson, E.S. et al. Injuries in Canadian high school boys’ collision sports: insights across football, ice hockey, lacrosse, and rugby. Sport Sci Health 19, 1129–1137 (2023). https://doi.org/10.1007/s11332-022-00999-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-022-00999-w