
Abstract
Background
The buccal space is an unusual location of malignancies. We report here the case of a woman with a melanoma metastasis in buccal fat pad, to evaluate the imaging features which might lead to the correct, although uncommon, diagnosis.
Case presentation
A 71-year-old woman presented with a painless visible swelling of the left cheek. MRI revealed the presence of a solid lesion located in the buccal fat pad with features suggestive of malignancy. It showed T1 hyperintensity and T2 hypointensity, and restriction of diffusion. Histological examination showed neoplastic cells compatible with melanoma.
Discussion
The lesion features (T1 hyperintensity and T2 hypointensity) initially lead our team to believe that there was a hemorrhagic component, possibly a residue of the biopsy. However, when associated with other malignancy features, such as low apparent diffusion coefficient (ADC) values and contrast enhancement, they should evoke the suspect of melanoma, provided that no biopsy was performed and no trauma occurred in the 3–7 days before.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The buccal space is one of the deep anatomical compartments of the head and neck regions, enveloped by the superficial layer of the deep cervical fascia (Fig. 1). It is delimited medially by the buccinator muscle, laterally by the platysma muscle, anteriorly by the mimic muscles, and posteriorly by the mandible, medial and lateral pterygoid muscles, and parotid and masseter muscle [1, 2].

Anatomy of the buccal space
Most of the buccal space is occupied by adipose tissue—the buccal fat pad—which laterally follows the parotid duct ending near the anterolateral portion of the parotid gland; medially, it projects towards the mandible and maxillary sinus; superiorly, it is divided by the temporal muscle into a superficial and deep portion and by the parotid duct into an anterior and posterior portion [3].
The buccal space frequently communicates with the posterior masticatory space and with the infratemporal space; moreover, there is no real lower boundary with the submandibular space. This anatomical space can thus function as a conduit to spread infectious or tumoral tissue between the mouth and the parotid gland.
Buccal space lesions are usually associated with cheek mass or facial swelling [4].
Beside inflammatory manifestations and developmental lesions such as accessory parotid tissue (present in up to 20% of the population), dermoid cysts, and vascular malformations, a variety of tumors can occur in the buccal space [5].
The most common tumor processes localized in this area arise from minor salivary glands such as pleomorphic adenoma (PA), adenoid cystic carcinoma, acinic cell carcinoma, and mucoepidermoid carcinoma. Other tumors can originate from connective, muscular, neural, and lymphatic tissue, such as rhabdomyosarcomas and neurofibromas [5].
Metastatic lesions in this region are a very rare occurrence, accounting for less than 1% of oral cavity malignancies [6]. They are most commonly located in bony structures, particularly the mandible, while only about 33% are found in soft tissues [7]. Metastatic lesions can often be the first sign of a widespread malignant disease, generally indicating poor outcome [8]. However, there are only a few studies focusing on metastatic lesions in the buccal and masticatory space, and even less literature regarding malignant melanoma metastases in this region; moreover, most studies were carried out from a surgical standpoint [9,10,11,12,13].
We report here the case of a female patient, with negative oncological history, who presented to our unit with a swelling of the left cheek, which revealed to be a melanoma metastasis only after surgical exeresis.
We analyze our experience with a revision of the literature, aiming for a retrospective evaluation of the diagnostic imaging characteristics which might be useful in guiding the differential diagnosis, to set an example to avoid repeating the same error in the future and to be of help to those who will find themselves in such a situation.
Case report
A 71-year-old woman presented with a painless visible swelling of the left cheek. Skin and oral mucosa were intact and of normal color. At palpation, the mass was mobile and apparently not adherent to the cutaneous and mucosal tissue.
For what concerns comorbidities, the patient was only known for Hashimoto thyroiditis in hormone replacement treatment (no relevant comorbidity was known).
Under ultrasound guidance, a 3-cm hypoechoic lesion was visualized in the left malar region and fine-needle-aspiration biopsy (FNAB) was performed. Cytological examination showed numerous Red Blood Cells, some lymphoid small B- and T-cells, plasma cells with no polyclonal atypia and a population of small-sized cells with plasmacytoid cells with the following immunophenotype: S-100 protein + , GFAP ± , P63 ± , cytokeratin7-, suggesting a salivary origin. However, a more precise diagnosis was not possible because of the small amount of material available.
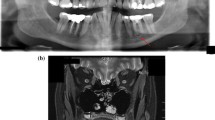
The following month, Magnetic Resonance Imaging (MRI) with intravenous paramagnetic contrast (Gadobutrol) was performed (Fig. 1). T1-weighted (T1w), T2-weighted (T2w), fat-saturated Short-TI Inversion Recovery (STIR), Diffusion-Weighted Imaging (DWI), and T1w sequences after contrast administration were acquired. It revealed the presence of a solid polylobate lesion located around the left parotid duct, with an antero-inferior component of 13 × 13 × 15 mm in the soft tissues adjacent to the buccinators, and another component of about 22 × 27 × 29 mm in the buccal fat pad (Fig. 2) extending into the infratemporal fossa up to the pterygo-maxillary fissure, which exerted a mass effect on the masticatory muscles and the posterolateral wall of the maxillary sinus. The mass showed contrast medium uptake and diffusion restriction (apparent diffusion coefficient, ADC = 0.9). Notably, the lesion displayed hyperintense signal compared to muscles in T1w sequences and hypointensity on T2w sequences. Some enlarged oval lymph nodes with progressive contrast enhancement were present in the left fifth cervical level. Overall, the MRI findings were suggestive of a malignant lesion that the radiologists assumed to have arisen from minor salivary glands on the basis of the anamnesis of the patient and of the epidemiology of neoplasms in this region.

Magnetic resonance imaging revealed a solid mass located in the left buccal space. a The lesion (arrow) showed a focal component with high signal intensity on axial T1-weighted imaging and b low signal intensity on T2-weighted imaging and c on fat-saturated T2 STIR sequences. d Diffusion-weighted imaging revealed a restricted diffusion change with e low apparent diffusion coefficient of 0.9. f After intravenous contrast administration, the lesion showed increased signal intensity on T1-weighted imaging
The T1 hyperintensity was referred to possible blood residues in consideration of the recent bioptic procedure.
Surgical exeresis was performed 2 weeks later. Intraoral access through the gingival fornix was obtained. The lesion, which extended to the pterygo-maxillary fissure, did not adhere to the surrounding tissues and was easily removed. It was partially solid, with a colliquated component.
Histological examination showed the presence of fibro-connective and lymphatic tissue containing malignant neoplastic cells compatible with a nodule of melanoma inside the buccal fat pad (Fig. 3).

Microscopic pictures of the surgical specimen. a–d H&E stain at increasing magnification (respectively, × 40, × 100, × 200, and × 400) showing proliferating atypical cells containing coarse-brownish granules suspected to be melanin; e, f, respectively, S-100 and SOX10 immunohistochemical stains confirming the diagnosis of melanoma
Gene mutation analysis for c-KIT and BRAF was performed: c-KIT was Wild Type (WT), while V600 mutation of BRAF exon 15 was found.
[F-18]FDG PET-CT (Fig. 4) revealed multiple localizations of pathological radiotracer hyper-accumulation: bilateral suprahyoid and axillary lymph nodes, fifth liver segment, right adrenal gland, multiple abdominal solid lesions (perigastric, left psoas muscle, right iliac fossa), various subcutaneous, and muscular tissue localizations (left and right thigh and gluteus, right pectoral muscle, right masseter, and right fourth toe).

[F-18]FDG PET-CT reveals avid FDG uptake by the left buccal space lesion (a). Multiple pathological radiotracer hyper-accumulation localizations were present, such as in a voluminous left axillary lymph node (b), a perigastric solid lesion (c), and in the muscular tissue of the left thigh (d)
Full-body computed tomography (CT) with intravenous contrast was then performed, with the following results: no encephalic lesions; 2-cm left cervical lymph node (LN); 5-mm left paracardiac micronodule; 7-cm LN conglomerate in the left axillary region; bilateral adrenal lesions (3.5 cm on the right side; 2 cm on the left); multiple enlarged mesenteric LNs, the largest of about 2 cm; 2.8-cm lesion in the left psoas muscle.
Dermatological examination revealed a 2-cm ulcerated cutaneous lesion on the distal phalanx of the left fifth finger, compatible with a primitive localization. The patient reported having it for about 1 year but never investigating it. Incisional biopsy of the lesion was performed, and histological examination confirmed the presence of melanoma cells with V600E mutation of BRAF gene.
Immediately afterwards, treatment was begun with Dabrafenib 300 mg/die and Trametinib 2 mg/die.
Two follow-up full-body CTs at 2 and 6 months were performed and showed significant size reduction of the axillary and abdominal LNs, of the adrenal and mesenteric localizations, and disappearance of the thoracic nodules.
Discussion
A variety of processes can occur in the buccal space, such as infections, developmental lesions, and tumoral processes.
Neoplastic lesions in this area origin most commonly from minor salivary glands, such as pleomorphic adenoma, adenoid cystic carcinoma, acinic cell carcinoma, and mucoepidermoid carcinoma.
The most frequent benign glandular tumor is PA, which consists of both mesodermal and glandular tissue [3]. It has smooth, rounded margins and shows low signal intensity on T1w image, high T2 signal intensity, and no diffusion restriction on DWI.
The most common malignant glandular tumor is adenoid cystic carcinoma. Some authors have suggested that lesions with low or intermediate T2-hyperintensity or invading surrounding tissues tend to be more aggressive, whereas lesions characterized by high signal intensity in T2w sequences have lower cellularity and better prognosis [14].
Other tumors can originate from connective, muscular, neural, and lymphatic tissue, such as rhabdomyosarcomas and neurofibromas [5]; rhabdomyosarcomas appear as muscle density masses at CT and are hyperintense relative to muscles on T2w MRI often showing bone destruction [15], while neurofibromas show low intensity on T1w imaging and high intensity on T2w imaging and are often associated with neurofibromatosis. Single neurofibromas characteristically show the target sign with peripheral hyperintensity [15].
Usually, in diffusion-weighted MRI, the ADC of malignant neoplasms of the head and neck regions is lower than that of benign tumors, and it is an important tool in guiding the diagnostic process [16].
Metastatic malignant melanoma is an uncommon head and neck neoplasm. The most frequent localizations of melanoma metastases are lymph nodes (73.6%), lungs (71.3%), liver (58.3%), brain (49.1%), bone (48.6%), heart (47.2%), adrenal glands (46.8%), and gastrointestinal tract (43.5%) [17].
Melanoma localized in the oral cavity and surrounding anatomical regions, such as the buccal fat pad, accounts for 0.2–8% of the total cases of melanomas of the body [18]. However, most studies focus on primary malignant melanoma, while secondary localization of melanoma in this region has been very rarely reported in the literature, with only one study describing a metastatic melanoma in the tongue and, to the best of our knowledge, no reports at all of the secondary melanomas in the buccal space [19].
Therefore, based on epidemiologic criteria, it is rather hard to diagnose metastatic melanoma in the buccal space in patients with an unknown primary tumor, as in our case.
Yet, MRI may be helpful in the identification of melanoma metastases [20].
Two main MRI patterns of melanoma can be identified: a melanocytic and amelanocytic pattern [21].
Lesions showing a melanocytic pattern, which is the more common one, are characterized by signal hyperintensity in T1w and hypointensity in T2w images. This is due to the presence of melanin and blood products inside the lesion, although some authors argue that the T1 hyperintensity is more relevantly associated with the presence of blood products [21,22,23].
Less commonly, malignant melanoma may show an amelanocytic (and therefore a specific) pattern, characterized by hypo- or isointensity in T1w images and hyper- or isointensity in T2w images [21], which is associated at histopathological examination to lower quantity of melanin inside the lesion [24].
Macroscopically, metastatic malignant melanoma may present in different ways, ranging from small rapidly growing lesions which may initially go undetected or misrecognized as artifacts, to showing a military pattern [25].
In our case, MRI showed a single lesion that exhibited diffusion restriction with ADC of 0.9 and high contrast medium uptake, characteristics suggestive of malignancy as it was proposed in the report.
Moreover, the mass was characterized by T1 hyperintensity and T2 hypointensity, a behavior which may be attributed to the melanoma melanocytic pattern; however, it is not specific, since such features may be ascribed to other paraphysiological and pathological processes, including hemorrhages and proteinic fluid collections.
In this case, radiologists supposed that there was a hemorrhagic component inside the lesion, possibly a residue of the FNAB which had been performed 1 month and a half before. Yet, this was a mistake. In fact, only early subacute hemorrhage dating 3–7 days is featured by T1 hyperintensity and T2 hypointensity, whereas chronic hemorrhages dating more than 1 month are rather characterized by both T1 and T2 hypointensity (26).
Overlooking this aspect and ignoring a part of the anamnesis, radiologists assumed that they were dealing with a primitive buccal space neoplasm, namely with a malignant (minor) salivary gland tumor.
On the contrary, this case teaches that T1 hyperintensity and T2 hypointensity, when associated with other malignancy features in buccal space lesion such as low ADC values and contrast enhancement, should always evoke the suspicion of melanoma, provided that no biopsy was performed and no trauma occurred in the 3–7 days before MRI examination.
Abbreviations
- ADC:
-
Apparent diffusion coefficient
- CT:
-
Computed tomography
- DWI:
-
Diffusion-weighted imaging
- FNAB:
-
Fine-needle-aspiration biopsy
- LN:
-
Lymph node
- MRI:
-
Magnetic resonance imaging
- PA:
-
Pleomorphic adenoma
- STIR:
-
Short-TI inversion recovery
- T1w:
-
T1-weighted
- T2w:
-
T2-weighted
References
Tart RP, Kotzur IM, Mancuso AA, Glantz MS, Mukherji SK. CT and MR imaging of the buccal space and buccal space masses. RadioGraphics. 1995;15(3):531–50.
Kurabayashi T, Ida M, Tetsumura A, Ohbayashi N, Yasumoto M, Sasaki T. MR imaging of benign and malignant lesions in the buccal space. Dentomaxillofac Radiol. 2002;31(6):344–9.
Kim H-C, Han MH, Moon MH, Kim JH, Kim I-O, Chang K-H. CT and MR imaging of the buccal space: normal anatomy and abnormalities. Korean J Radiol. 2005;6(1):22.
Gupta TD, Brasfield R. Metastatic melanoma. A clinicopathological study. Cancer 1964;17(10):1323–39.
Smoker WRK. Oral cavity. In: PM Som, HD Curtin, editors. Head and neck imaging. 3rd ed. St Louis, Mo: Mosby; 1996. p. 488–544.
Irani S. Metastasis to the oral soft tissues: a review of 412 cases. J Int Soc Prev Community Dent. 2016;6(5):393.
Hirshberg A, Leibovich P, Buchner A. Metastases to the oral mucosa: analysis of 157 cases. J Oral Pathol Med. 1993;22(9):385–90.
Vega LG, Dipasquale J, Gutta R. Head and neck manifestations of distant carcinomas. Oral Maxillofac Surg Clin North Am. 2008;20(4):609–23.
Henderson LT, Robbins KT, Weitzner S. Upper aerodigestive tract metastases in disseminated malignant melanoma. Arch Otolaryngol Head Neck Surg. 1986;112(6):659–63.
Billings K, Wang M, Sercarz J, Fu Y. Clinical and pathologic distinction between primary and metastatic mucosal melanoma of the head and neck. Otolaryngol Head Neck Surg. 1995;112(6):700–6.
Barlas Aydogan L, Myers JN, Myers EN, Kirkwood J. Malignant Melanoma Metastatic to the Tonsil. Laryngoscope. 1996;106(3):313–6.
Coelho FH, Pellicioli ACA, Martins MAT, Pavesi VCS, Schmerling RA, Martins MD. Multiple metastases of malignant melanoma in the head and neck: a case report and literature review. General Dentistry. 2014;62(1):43–8.
Mifsud M, Padhya TA. Metastatic melanoma to the upper aerodigestive tract: a systematic review of the literature. Laryngoscope. 2014;124(5):1143–9.
Walvekar RR, Myers EN. Management of the mass in the buccal space. In: Salivary gland disorders. Berlin: Springer; 2007. p. 281–94.
Shah GV. MR imaging of salivary glands. Neuroimaging Clin N Am. 2004;14(4):777–808.
Wang J, Takashima S, Takayama F, Kawakami S, Saito A, Matsushita T, et al. Head and neck lesions: characterization with diffusion-weighted echo-planar MR imaging. Radiology. 2001;220(3):621–30.
Patel JK, Didolkar MS, Pickren JW, Moore RH. Metastatic pattern of malignant melanoma. A study of 216 autopsy cases. Am. J. Surg. 1978;135(6):807–10.
Kumar A, Bindal R, Shetty DC, Singh HP. Primary oral malignant melanoma: Clinicopathological series of four cases. Dent Res J. 2012;9(3):338.
Alves MGO, Chagas LR, Carvalho YR, Cabral LAG, Coletta RD, Almeida JD. Metastatic melanoma of the tongue: a case report with immunohistochemical profile. Gerodontology. 2014;31(4):314–9.
Yoshioka H, Kamada T, Kandatsu S, Koga M, Yoshikawa K, Matsuoka Y, et al. MRI of mucosal malignant melanoma of the head and neck. J Comput Assist Tomogr. 1998;22(3):492–7.
Escott EJ. A variety of appearances of malignant melanoma in the head: a review. RadioGraphics. 2001;21(3):625–39.
Woodruff WW, Djang WT, Mclendon RE, Heinz ER, Voorhees DR. Intracerebral malignant melanoma: high-field-strength MR imaging. Radiology. 1987;165(1):209–13.
Gaviani P, Mullins ME, Braga TA, Hedley-Whyte ET, Halpern EF, Schaefer PS, et al. Improved detection of metastatic melanoma by T2*-weighted imaging. AJNR Am J Neuroradiol. 2006;27(3):605–8.
Isiklar I, Leeds NE, Fuller GN, Kumar AJ. Intracranial metastatic melanoma: correlation between MR imaging characteristics and melanin content. AJR Am J Roentgenol. 1995;165(6):1503–12.
Rainov NG, Burkert W. Miliary metastatic tumors. J Neurosurg. 1997;87(6):979–979.
Grand DJ, Woodfield CA, Mayo-Smith WW. Practical body MRI: protocols, applications and image interpretation. Cambridge: Cambridge University Press; 2009.
Acknowledgements
Open access funding provided by Università degli Studi di Milano within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Grillo, P., Savoldi, A.P., Di Meo, R. et al. An unusual case of melanoma metastasis in the buccal space: learning by mistakes to distinguish it from salivary neoplasms. Oral Radiol 37, 146–152 (2021). https://doi.org/10.1007/s11282-020-00470-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11282-020-00470-x