
Abstract
Purpose
Effectiveness of cardiac resynchronization therapy (CRT) in patients without left bundle branch block (non-LBBB) QRS morphology is limited. Additional selection criteria are needed to identify these patients.
Methods
Seven hundred ninety consecutive patients with non-LBBB morphology, who received a CRT-device in 3 university centers in the Netherlands, were selected. Pre-implantation 12-lead ECGs were evaluated on morphology, duration, and area of the QRS complex, as well as on PR interval, left ventricular activation time (LVAT), and the presence of fragmented QRS (fQRS). Association of these ECG features with the primary endpoint: a combination of left ventricular assist device (LVAD) implantation, cardiac transplantation and all-cause mortality, and secondary endpoint—echocardiographic reduction of left ventricular end-systolic volume (LVESV)—were evaluated.
Results
The primary endpoint occurred more often in non-LBBB patients with with PR interval ≥ 230ms, QRS area < 109μVs, and with fQRS. Multivariable regression analysis showed independent associations of QRS area (HR 2.33 [1.44, 3.77], p = 0.001) and PR interval (HR 2.03 [1.51, 2.74], p < 0.001) only. Mean LVESV reduction was significantly lower in patients with baseline RBBB, QRS duration < 150 ms, PR interval ≥ 230 ms, and in QRS area < 109 μVs. Multivariable regression analyses only showed significant associations between QRS area ≥ 109 μVs (OR 2.00 [1.09, 3.66] p = 0.025) and probability of echocardiographic response to CRT.
Conclusions
In the heterogeneous non-LBBB patient population, QRS area and PR prolongation rather than traditional QRS duration and morphology are associated to both clinical and echocardiographic outcomes of CRT.



Similar content being viewed by others


References
Zareba W, Klein H, Cygankiewicz I, Hall WJ, McNitt S, Brown M, et al. effectiveness of cardiac resynchronization therapy by QRS morphology in the multicenter automatic defibrillator implantation Trial-Cardiac Resynchronization Therapy (MADIT-CRT). Circulation. 2011;123(10):1061–72. https://doi.org/10.1161/CIRCULATIONAHA.110.960898.
Gold MR, Thebault C, Linde C, Abraham WT, Gerritse B, Ghio S, et al. Effect of QRS duration and morphology on cardiac resynchronization therapy outcomes in mild heart failure: results from the Resynchronization Reverses Remodeling in Systolic Left Ventricular Dysfunction (REVERSE) study. Circulation. 2012;126(7):822–9. https://doi.org/10.1161/CIRCULATIONAHA.112.097709.
Bilchick KC. Does cardiac resynchronization therapy benefit patients with right bundle branch block: left ventricular free wall pacing: seldom right for right bundle branch block. Circ Arrhythm Electrophysiol. 2014;7(3):543–52. https://doi.org/10.1161/CIRCEP.113.000747.
Birnie DH, Ha A, Higginson L, Sidhu K, Green M, Philippon F, et al. Impact of QRS morphology and duration on outcomes after cardiac resynchronization therapy: results from the Resynchronization-Defibrillation for Ambulatory Heart Failure Trial (RAFT). Circ Heart Fail. 2013;6(6):1190–8. https://doi.org/10.1161/CIRCHEARTFAILURE.113.000380.
Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–200. https://doi.org/10.1093/eurheartj/ehw128.
Cleland JG, Abraham WT, Linde C, Gold MR, Young JB, Claude Daubert J, et al. An individual patient meta-analysis of five randomized trials assessing the effects of cardiac resynchronization therapy on morbidity and mortality in patients with symptomatic heart failure. Eur Heart J. 2013;34(46):3547–56. https://doi.org/10.1093/eurheartj/eht290.
Woods B, Hawkins N, Mealing S, Sutton A, Abraham WT, Beshai JF, et al. Individual patient data network meta-analysis of mortality effects of implantable cardiac devices. Heart. 2015;101(22):1800–6. https://doi.org/10.1136/heartjnl-2015-307634.
Kutyifa V, Stockburger M, Daubert JP, Holmqvist F, Olshansky B, Schuger C, et al. PR interval identifies clinical response in patients with non-left bundle branch block: a multicenter automatic defibrillator implantation trial-cardiac resynchronization therapy substudy. Circ Arrhythm Electrophysiol. 2014;7(4):645–51. https://doi.org/10.1161/CIRCEP.113.001299.
Senfield J, Daubert C, Abraham WT, Ghio S. St John Sutton M, Cerkvenik J et al. The impact of the PR interval in patients receiving cardiac resynchronization therapy: results from the REVERSE study. JACC Clin Electrophysiol. 2017;3(8):818–26. https://doi.org/10.1016/j.jacep.2017.01.017.
Mafi Rad M, Wijntjens GW, Engels EB, Blaauw Y, Luermans JG, Pison L, et al. Vectorcardiographic QRS area identifies delayed left ventricular lateral wall activation determined by electroanatomic mapping in candidates for cardiac resynchronization therapy. Heart Rhythm. 2016;13(1):217–25. https://doi.org/10.1016/j.hrthm.2015.07.033.
Eitel C, Wilton SB, Switzer N, Cowan K, Exner DV. Baseline delayed left ventricular activation predicts long-term clinical outcome in cardiac resynchronization therapy recipients. Europace. 2012;14(3):358–64. https://doi.org/10.1093/europace/eur298.
Celikyurt U, Agacdiken A, Sahin T, Al N, Kozdag G, Vural A, et al. Number of leads with fragmented QRS predicts response to cardiac resynchronization therapy. Clin Cardiol. 2013;36(1):36–9. https://doi.org/10.1002/clc.22061.
van Deursen CJ, Vernooy K, Dudink E, Bergfeldt L, Crijns HJ, Prinzen FW, et al. Vectorcardiographic QRS area as a novel predictor of response to cardiac resynchronization therapy. J Electrocardiol. 2015;48(1):45–52. https://doi.org/10.1016/j.jelectrocard.2014.10.003.
Brignole M, Auricchio A, Baron-Esquivias G, Bordachar P, Boriani G, Breithardt OA, et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur Heart J. 2013;34(29):2281–329. https://doi.org/10.1093/eurheartj/eht150.
Dickstein K, Vardas PE, Auricchio A, Daubert JC, Linde C, McMurray J, et al. 2010 Focused Update of ESC Guidelines on device therapy in heart failure: an update of the 2008 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure and the 2007 ESC guidelines for cardiac and resynchronization therapy. Developed with the special contribution of the Heart Failure Association and the European Heart Rhythm Association. Eur Heart J. 2010;31(21):2677–87. https://doi.org/10.1093/eurheartj/ehq337.
Strauss DG, Selvester RH, Wagner GS. Defining left bundle branch block in the era of cardiac resynchronization therapy. Am J Cardiol. 2011;107(6):927–34. https://doi.org/10.1016/j.amjcard.2010.11.010.
Engels EB, Vegh EM, Van Deursen CJ, Vernooy K, Singh JP, Prinzen FW. T-wave area predicts response to cardiac resynchronization therapy in patients with left bundle branch block. J Cardiovasc Electrophysiol. 2015;26(2):176–83. https://doi.org/10.1111/jce.12549.
Engels EB, Alshehri S, van Deursen CJ, Wecke L, Bergfeldt L, Vernooy K, et al. The synthesized vectorcardiogram resembles the measured vectorcardiogram in patients with dyssynchronous heart failure. J Electrocardiol. 2015;48(4):586–92. https://doi.org/10.1016/j.jelectrocard.2015.04.001.
Kors JA, van Herpen G, Sittig AC, van Bemmel JH. Reconstruction of the Frank vectorcardiogram from standard electrocardiographic leads: diagnostic comparison of different methods. Eur Heart J. 1990;11(12):1083–92.
van Stipdonk AMW, Ter Horst I, Kloosterman M, Engels EB, Rienstra M, Crijns H, et al. QRS Area Is a Strong Determinant of Outcome in Cardiac Resynchronization Therapy. Circ Arrhythm Electrophysiol. 2018;11(12):e006497. https://doi.org/10.1161/CIRCEP.118.006497.
Sweeney MO, van Bommel RJ, Schalij MJ, Borleffs CJ, Hellkamp AS, Bax JJ. Analysis of ventricular activation using surface electrocardiography to predict left ventricular reverse volumetric remodeling during cardiac resynchronization therapy. Circulation. 2010;121(5):626–34. https://doi.org/10.1161/CIRCULATIONAHA.109.894774.
Das MK, Suradi H, Maskoun W, Michael MA, Shen C, Peng J, et al. Fragmented wide QRS on a 12-lead ECG: a sign of myocardial scar and poor prognosis. Circ Arrhythm Electrophysiol. 2008;1(4):258–68. https://doi.org/10.1161/CIRCEP.107.763284.
Maass AH, Vernooy K, Wijers SC, van’t Sant J, Cramer MJ, Meine M, et al. Refining success of cardiac resynchronization therapy using a simple score predicting the amount of reverse ventricular remodelling: results from the Markers and Response to CRT (MARC) study. Europace. 2018;20(2):e1–e10. https://doi.org/10.1093/europace/euw445.
Vegh EM, Engels EB, van Deursen CJ, Merkely B, Vernooy K, Singh JP, et al. T-wave area as biomarker of clinical response to cardiac resynchronization therapy. Europace. 2016;18(7):1077–85. https://doi.org/10.1093/europace/euv259.
Atwater BD, Emerek K, Sorensen PL, Hansen SM, Loring Z, Graff C, et al. PR Prolongation predicts inadequate resynchronization with biventricular pacing in left bundle branch block. Pacing Clin Electrophysiol. 2019;42(11):1477–85. https://doi.org/10.1111/pace.13802.
Salden F, Kutyifa V, Stockburger M, Prinzen FW, Vernooy K. Atrioventricular dromotropathy: evidence for a distinctive entity in heart failure with prolonged PR interval? Europace. 2018;20(7):1067–77. https://doi.org/10.1093/europace/eux207.
Linde C, Abraham WT, Gold MR, St John Sutton M, Ghio S, Daubert C, et al. Randomized trial of cardiac resynchronization in mildly symptomatic heart failure patients and in asymptomatic patients with left ventricular dysfunction and previous heart failure symptoms. J Am Coll Cardiol. 2008;52(23):1834–43. https://doi.org/10.1016/j.jacc.2008.08.027.
Moss AJ, Hall WJ, Cannom DS, Klein H, Brown MW, Daubert JP, et al. Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med. 2009;361(14):1329–38. https://doi.org/10.1056/NEJMoa0906431.
Tang AS, Wells GA, Talajic M, Arnold MO, Sheldon R, Connolly S, et al. Cardiac-resynchronization therapy for mild-to-moderate heart failure. N Engl J Med. 2010;363(25):2385–95. https://doi.org/10.1056/NEJMoa1009540.
van der Bijl P, Khidir M, Leung M, Mertens B, Ajmone Marsan N, Delgado V, et al. Impact of QRS complex duration and morphology on left ventricular reverse remodelling and left ventricular function improvement after cardiac resynchronization therapy. Eur J Heart Fail. 2017;19(9):1145–51. https://doi.org/10.1002/ejhf.769.
Khidir MJ, Delgado V, Ajmone Marsan N, Schalij MJ, Bax JJ. QRS duration versus morphology and survival after cardiac resynchronization therapy. ESC Heart Fail. 2017;4(1):23–30. https://doi.org/10.1002/ehf2.12122.
Rickard J, Zardkoohi O, Popovic Z, Verhaert D, Sraow D, Baranowski B, et al. QRS fragmentation is not associated with poor response to cardiac resynchronization therapy. Ann Noninvasive Electrocardiol. 2011;16(2):165–71. https://doi.org/10.1111/j.1542-474X.2011.00424.x.
Eschalier R, Ploux S, Ritter P, Haissaguerre M, Ellenbogen KA, Bordachar P. Nonspecific intraventricular conduction delay: Definitions, prognosis, and implications for cardiac resynchronization therapy. Heart Rhythm. 2015;12(5):1071–9. https://doi.org/10.1016/j.hrthm.2015.01.023.
Strik M, Regoli F, Auricchio A, Prinzen F. Electrical and mechanical ventricular activation during left bundle branch block and resynchronization. J Cardiovasc Transl Res. 2012;5(2):117–26. https://doi.org/10.1007/s12265-012-9351-1.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
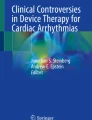
Supplementary Figure 1
Example of ECG-parameters in non-LBBB. Figure including normal 12-lead ECG on left and respesentative ECG-parameters evaluated in non-LBBB patients in the current study. ECG parameters included from upper-left to lower right box are; (1) QRS morphology with example of lead V1 RSR pattern indicative of RBBB morphology, (2) QRS duration measurement, (3) PR interval measurement with evident PR prolongation in example, (4) QRS area measurement with vector X-axis displayed. QRS area requiring area measurement in X-, Y- and Z-axis and calculation of total QRS area according to formula: (QRS areaX2 + QRS areaY2 + QRS areaZ2)1/2, (5) fQRS assessment and (6) LVAT measurement from notch or slurring to end of the QRS complex. The 12-lead ECG is representative of the QRS duration, QRS area and LVAT measurement. fQRS fragmented QRS, LVAT left ventricular activation time, non-LBBB non-left bundle branch block, RBBB right bundle branch block.(PNG 176 kb)
Rights and permissions
About this article

Cite this article
Dural, M., van Stipdonk, A.M.W., Salden, F.C.W.M. et al. Association of ECG characteristics with clinical and echocardiographic outcome to CRT in a non-LBBB patient population. J Interv Card Electrophysiol 62, 9–19 (2021). https://doi.org/10.1007/s10840-020-00866-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-020-00866-z