
Summary
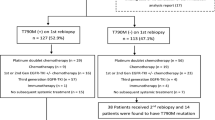
Data on the re-administration of epidermal growth factor receptor (EGFR)-tyrosine kinase inhibitors (TKIs) after osimertinib failure in patients with T790M-positive non–small cell lung cancer (NSCLC) is limited. EGFR-TKI re-administration efficacy may vary between patients with T790M loss and those with T790M persistent with re-biopsy after osimertinib treatment. Patients who received EGFR-TKI re-administration (gefitinib, erlotinib, afatinib, dacomitinib, and osimertinib) after osimertinib failure were identified from our database. T790M mutation status before EGFR-TKI re-administration was analyzed via repeat biopsy. We retrospectively evaluated the efficacy of EGFR-TKI re-administration, especially differences according to the T790M mutation status, via repeat biopsy. Until June 2020, 28 patients received EGFR-TKI re-administration and 17 underwent repeat biopsy after osimertinib failure. Patients were divided into three groups, including the T790M loss group, where active mutation persisted and T790M was lost (13/17); T790M remaining group, where both the active mutation and T790M persisted (3/17); and active mutation loss group where both the active mutation and T790M were lost (1/17). The overall response rate (ORR) of EGFR-TKI re-administration in the T790M loss group was 31% and the disease control rate (DCR) was 54%, which were higher than the ORR of 21% and DCR of 43% in the entire patient population. ORR and DCR of the not re-biopsy group were low (9% and 27%, respectively). The therapeutic effect of EGFR-TKI re-administration in patients with T790M-positive NSCLC after osimertinib failure is limited. EGFR-TKI re-administration may be considered in cases of T790M loss after repeat biopsy.


Similar content being viewed by others

Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Sève P, Reiman T, Dumontet C (2010) The role of βIII tubulin in predicting chemoresistance in non-small cell lung cancer. Lung Cancer 67:136–143. https://doi.org/10.1016/j.lungcan.2009.09.007
Lynch TJ, Bell DW, Sordella R et al (2004) Activating mutations in the epidermal growth factor receptor underlying responsiveness of non–small-cell lung cancer to gefitinib. New Engl J Medicine 350:2129–2139. https://doi.org/10.1056/nejmoa040938
Maemondo M, Inoue A, Kobayashi K et al (2010) Gefitinib or chemotherapy for non–small-cell lung cancer with mutated EGFR. New Engl J Medicine 362:2380–2388. https://doi.org/10.1056/nejmoa0909530
Wu Y-L, Zhou C, Hu C-P et al (2014) Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): an open-label, randomised phase 3 trial. Lancet Oncol 15:213–222. https://doi.org/10.1016/s1470-2045(13)70604-1
Rosell R, Carcereny E, Gervais R et al (2012) Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol 13:239–246. https://doi.org/10.1016/s1470-2045(11)70393-x
Sequist LV, Yang JC-H, Yamamoto N et al (2013) Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with egfr mutations. J Clin Oncol 31:3327–3334. https://doi.org/10.1200/jco.2012.44.2806
Mitsudomi T, Morita S, Yatabe Y et al (2009) Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol 11:121–128. https://doi.org/10.1016/s1470-2045(09)70364-x
Sequist LV, Waltman BA, Dias-Santagata D et al (2011) Genotypic and histological evolution of lung cancers acquiring resistance to EGFR inhibitors. Sci Transl Med 3:75ra26. https://doi.org/10.1126/scitranslmed.3002003
Yu HA, Arcila ME, Rekhtman N et al (2013) Analysis of Tumor Specimens at the Time of Acquired Resistance to EGFR-TKI Therapy in 155 Patients with EGFR-Mutant Lung Cancers. Clin Cancer Res 19:2240–2247. https://doi.org/10.1158/1078-0432.ccr-12-2246
Cross DAE, Ashton SE, Ghiorghiu S et al (2014) AZD9291, an Irreversible EGFR TKI, Overcomes T790M-Mediated Resistance to EGFR Inhibitors in Lung Cancer. Cancer Discov 4:1046–1061. https://doi.org/10.1158/2159-8290.cd-14-0337
Ballard P, Yates JWT, Yang Z et al (2016) Preclinical Comparison of Osimertinib with Other EGFR-TKIs in EGFR-Mutant NSCLC Brain Metastases Models, and Early Evidence of Clinical Brain Metastases Activity. Clin Cancer Res 22:5130–5140. https://doi.org/10.1158/1078-0432.ccr-16-0399
Mok TS, Wu Y-L, Ahn M-J et al (2017) Osimertinib or Platinum-Pemetrexed in EGFR T790M–Positive Lung Cancer. New Engl J Medicine 376:629–640. https://doi.org/10.1056/nejmoa1612674
Jänne PA, Yang JC-H, Kim D-W et al (2015) AZD9291 in EGFR Inhibitor-Resistant Non–Small-Cell Lung Cancer. New Engl J Medicine 372:1689–1699. https://doi.org/10.1056/nejmoa1411817
Inoue A, Yoshida K, Morita S et al (2016) Characteristics and overall survival of EGFR mutation-positive non-small cell lung cancer treated with EGFR tyrosine kinase inhibitors: a retrospective analysis for 1660 Japanese patients. Jpn J Clin Oncol 46:462–467. https://doi.org/10.1093/jjco/hyw014
Leonetti A, Sharma S, Minari R et al (2019) Resistance mechanisms to osimertinib in EGFR-mutated non-small cell lung cancer. Brit J Cancer 121:725–737. https://doi.org/10.1038/s41416-019-0573-8
Kohsaka S, Petronczki M, Solca F, Maemondo M (2019) Tumor clonality and resistance mechanisms in EGFR mutation-positive non-small-cell lung cancer: implications for therapeutic sequencing. Future Oncol 15:637–652. https://doi.org/10.2217/fon-2018-0736
Group: O behalf of Ngse, Marino P, Touzani R et al (2018) Cost of cancer diagnosis using next-generation sequencing targeted gene panels in routine practice: a nationwide French study. Eur J Hum Genet 26:314–323. https://doi.org/10.1038/s41431-017-0081-3
Papadimitrakopoulou VA, Wu Y-L, Han J-Y et al (2018) LBA51 analysis of resistance mechanisms to osimertinib in patients with EGFR T790M advanced NSCLC from the AURA3 study. Ann Oncol 29:viii741. https://doi.org/10.1093/annonc/mdy424.064
Oxnard GR, Hu Y, Mileham KF et al (2018) Assessment of resistance mechanisms and clinical implications in patients with EGFR T790M–Positive Lung cancer and acquired resistance to osimertinib. Jama Oncol 4:1527. https://doi.org/10.1001/jamaoncol.2018.2969
Kanda Y (2013) Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl 48:452–458. https://doi.org/10.1038/bmt.2012.244
Song Y, Wu Y-L, Cao L-J et al (2019) Efficacy and safety of gefitinib as third-line treatmentt in NSCLC Patients With Activating EGFR Mutations Treated With First-line Gefitinib Followed by Second-line Chemotherapy. Am J Clin Oncol 42:432–439. https://doi.org/10.1097/coc.0000000000000538
Becker A, Crombag L, Heideman DAM et al (2011) Retreatment with erlotinib: Regain of TKI sensitivity following a drug holiday for patients with NSCLC who initially responded to EGFR-TKI treatment. Eur J Cancer 47:2603–2606. https://doi.org/10.1016/j.ejca.2011.06.046
Oda N, Hotta K, Ninomiya K et al (2018) A phase II trial of EGFR-TKI readministration with afatinib in advanced non-small-cell lung cancer harboring a sensitive non-T790M EGFR mutation: Okayama Lung Cancer Study Group trial 1403. Cancer Chemoth Pharm 82:1031–1038. https://doi.org/10.1007/s00280-018-3694-5
Ichihara E, Hotta K, Ninomiya K et al (2019) Re-administration of osimertinib in osimertinib-acquired resistant non-small-cell lung cancer. Lung Cancer 132:54–58. https://doi.org/10.1016/j.lungcan.2019.02.021
Ercan D, Choi HG, Yun C-H et al (2015) EGFR mutations and resistance to irreversible pyrimidine-based EGFRinhibitors. Clin Cancer Res 21:3913–3923. https://doi.org/10.1158/1078-0432.ccr-14-2789
Fassunke J, Müller F, Keul M et al (2018) Overcoming EGFRG724S-mediated osimertinib resistance through unique binding characteristics of second-generation EGFR inhibitors. Nat Commun 9:4655. https://doi.org/10.1038/s41467-018-07078-0
Le X, Puri S, Negrao MV et al (2018) Landscape of EGFR -dependent and -independent resistance mechanisms to osimertinib and continuation therapy post-progression in EGFR-mutant NSCLC. Clin Cancer Res 24:clincanres.1542.2018. https://doi.org/10.1158/1078-0432.ccr-18-1542
Rotow JK, Costa DB, Paweletz CP et al (2020) Concurrent osimertinib plus gefitinib for first-line treatment of EGFR-mutated non-small cell lung cancer (NSCLC). J Clin Oncol 38:9507–9507. https://doi.org/10.1200/jco.2020.38.15_suppl.9507
Arulananda S, Do H, Musafer A et al (2017) Combination osimertinib and gefitinib in C797S and T790M EGFR-mutated non-small cell lung cancer. J Thorac Oncol 12:1728–1732. https://doi.org/10.1016/j.jtho.2017.08.006
Wang Z, Yang J-J, Huang J et al (2017) Lung adenocarcinoma harboring EGFR T790M and in trans C797S responds to combination therapy of first- and third-generation egfr tkis and shifts allelic configuration at resistance. J Thorac Oncol 12:1723–1727. https://doi.org/10.1016/j.jtho.2017.06.017
Ariyasu R, Uchibori K, Sasaki T et al (2021) Monitoring epidermal growth factor receptor C797S mutation in Japanese non–small cell lung cancer patients with serial cell-free DNA evaluation using digital droplet PCR. Cancer Sci 112:2371–2380. https://doi.org/10.1111/cas.14879
Low S-K, Ariyasu R, Uchibori K et al (2022) Rapid genomic profiling of circulating tumor DNA in non-small cell lung cancer using oncomine precision assay with genexus tm integrated sequencer Transl Lung Cancer Res 0:0–0. https://doi.org/10.21037/tlcr-21-981
Acknowledgements
We thank the patients and their families for their participation in the study. We thank the staff of the Department of Thoracic Medical Oncology, Cancer Institute Hospital, Japanese Foundation for Cancer Research, for supporting this study.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
(I) Conception and design: Shinsuke Ogusu, Ryo Ariyasu, Makoto Nishio; (II) Provision of study patients: All authors; (III) Data analysis and interpretation: Shinsuke Ogusu, Ryo Ariyasu; (IV) Manuscript writing: All authors; (V) Final approval of manuscript: All authors.
Corresponding author
Ethics declarations
Competing interests
R. Ariyasu reports honoraria from CHUGAI PHARMACEUTICAL CO., Bristol Myers Squib, ONO PHARMACEUTICAL CO., Astrazeneca, outside the submitted work, K. Uchibori reports payment for lectures from DAIICHI SANKYO COMPANY, CHUGAI PHARMACEUTICAL CO., Bristol Myers Squib, ONO PHARMACEUTICAL CO., Astrazeneca, Eli Lilly, Novartis, Thermo Fisher Scientific, Takeda Pharmaceutical Company outside the submitted work. His spouse is an employee of DAIICHI SANKYO. S.Kitazono reports honoraria from Chugai Pharmaceutical Co, Ltd . AstraZeneca, Ono Pharmaceutical, Pfizer, Bristol-Myers Squibb and Merck Sharp & Dohme Corp outside the submitted work. N. Yanagitani reports honoraria from CHUGAI PHARMACEUTICAL CO., Bristol Myers Squib, ONO PHARMACEUTICAL CO., Astrazeneca, Eli Lilly, Takeda Pharmaceutical Company, Pfizer, Bayer Yakuhin, Ltd outside the submitted work. M. Nishio reports grants and personal fees from Ono Pharmaceutical, Bristol Myers Squibb, Pfizer, Chugai Pharmaceutical, Eli Lilly, Taiho Pharmaceutical, AstraZeneca, MSD, Boehringer-Ingelheim, Novartis, Merck Biopharma, Daiichi Sankyo, Takeda Pharmaceutical Company Limited, personal fees from TEIJIN PHARMA LIMITED., AbbVie, outside the submitted work. The remaining authors have not conflicts of interest to declare.
Ethics approval
All procedures performed in studies involving human participants were conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This study was approved by the Clinical Research Ethics Committee of Cancer Institute Hospital of JFCR.
Consent to participate
The ethics review board of Cancer Institute Hospital of JFCR approved the present study and permitted the use of the opt-out method in lieu of written informed consent.
Competing interest
R. Ariyasu reports honoraria from CHUGAI PHARMACEUTICAL CO., Bristol Myers Squib, ONO PHARMACEUTICAL CO., Astrazeneca, outside the submitted work, K. Uchibori reports payment for lectures from DAIICHI SANKYO COMPANY, CHUGAI PHARMACEUTICAL CO., Bristol Myers Squib, ONO PHARMACEUTICAL CO., Astrazeneca, Eli Lilly, Novartis, Thermo Fisher Scientific, Takeda Pharmaceutical Company outside the submitted work. His spouse is an employee of DAIICHI SANKYO. S.Kitazono reports honoraria from Chugai Pharmaceutical Co, Ltd. AstraZeneca, Ono Pharmaceutical, Pfizer, Bristol-Myers Squibb and Merck Sharp & Dohme Corp outside the submitted work. N. Yanagitani reports honoraria from CHUGAI PHARMACEUTICAL CO., Bristol Myers Squib, ONO PHARMACEUTICAL CO., Astrazeneca, Eli Lilly, Takeda Pharmaceutical Company, Pfizer, Bayer Yakuhin, Ltd outside the submitted work. M. Nishio reports grants and personal fees from Ono Pharmaceutical, Bristol Myers Squibb, Pfizer, Chugai Pharmaceutical, Eli Lilly, Taiho Pharmaceutical, AstraZeneca, MSD, Boehringer-Ingelheim, Novartis, Merck Biopharma, Daiichi Sankyo, Takeda Pharmaceutical Company Limited, personal fees from TEIJIN PHARMA LIMITED., AbbVie, outside the submitted work. The remaining authors have not conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ogusu, S., Ariyasu, R., Akita, T. et al. EGFR-TKI re-administration after osimertinib failure in T790M mutation loss cases with re-biopsy. Invest New Drugs 40, 1342–1349 (2022). https://doi.org/10.1007/s10637-022-01301-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10637-022-01301-y