
Abstract
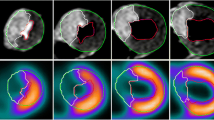
The purpose of the study was to validate by histopathology, contrast enhanced cine steady-state free precession and T2-weighted CMR for the assessment of ischemic myocardial area-at-risk (AAR) in the presence of microvascular obstruction (MVO). Eleven anesthetized pigs underwent CMR 7 to 10 days post infarction. The area-at-risk was measured from T2-weighted fast spin echo (T2-STIR) and contrast-enhanced steady-state free precession magnetic resonance imaging (CE-SSFP) images using semi-automated algorithms based on a priori knowledge of perfusion territory. Also, late gadolinium enhancement (LGE) was performed to measure final infarct size (FIS). Histopathological comparison with Evans blue dye to define AAR and triphenyltetrazolium chloride to define FIS served as the reference. All infarcts demonstrated MVO on LGE images. Bland–Altman analysis showed no significant bias in AAR or myocardial salvage between T2-STIR and CE-SSFP or between CMR and histopathology. The mean differences ± 2SD from Bland–Altman analysis were: AAR: Evans Blue vs. T2-STIR [0.7%; + 13.5%; − 12.1%]; AAR: Evans Blue vs. CE-SSFP [0.1%; + 13.8%; − 13.7%]; AAR: T2-STIR vs. CE-SSFP [0.7%; + 6.2%; − 4.9%]; Salvage: Evans Blue − TTC vs. T2-STIR-LGE [0.8%; + 11.1%; − 9.6%]; Salvage: Evans Blue − TTC vs. CE-SSFP-LGE [0.1%; + 9.9%; − 9.6%]; Salvage: CE-SSFP-LGE vs. T2-STIR-LGE [0.7%; + 6.2%; − 4.9%]. Both T2-STIR and CE-SSFP sequences allow for unbiased quantification of AAR in the presence of ischemia/reperfusion injury when analysed by semi-automated algorithms. These experimental data, which was validated by histopathology, supports the use of CMR for the assessment of myocardial salvage during the subacute phase.



Similar content being viewed by others
Abbreviations
- AAR:
-
Area-at-risk
- FIS:
-
Final infarct size
- CMR:
-
Cardiovascular magnetic resonance
- CE-SSFP:
-
Contrast-enhanced steady-state free precession magnetic resonance imaging
- ECG:
-
Electrocardiogram
- LV:
-
Left ventricular
- B-SSFP:
-
Balanced-steady-state-free-precession
- FOV:
-
Field of view
- TR:
-
Repetition time
- TE:
-
Echo time
- LGE:
-
Late gadolinium enhancement
- MVO:
-
Microvascular obstruction
- TTC:
-
Triphenyltetrazolium chloride
References
Botker HE et al (2012) Measuring myocardial salvage. Cardiovasc Res 94(2):266–275
Croisille P, Kim HW, Kim RJ (2012) Controversies in cardiovascular MR imaging: T2-weighted imaging should not be used to delineate the area at risk in ischemic myocardial injury. Radiology 265(1):12–22
Kim HW et al (2015) Relationship of T2-weighted MRI myocardial hyperintensity and the ischemic area-at-risk. Circ Res 117(3):254–265
Hansen ES et al (2016) Cardiovascular MR T2-STIR imaging does not discriminate between intramyocardial haemorrhage and microvascular obstruction during the subacute phase of a reperfused myocardial infarction. Open Heart 3(1):e000346
Fernandez-Jimenez R et al (2015) Myocardial edema after ischemia/reperfusion is not stable and follows a bimodal pattern: imaging and histological tissue characterization. J Am Coll Cardiol 65(4):315–323
Fernandez-Jimenez R et al (2017) Dynamic edematous response of the human heart to myocardial infarction: implications for assessing myocardial area at risk and salvage. Circulation 136(14):1288–1300
Sorensson P et al (2010) Assessment of myocardium at risk with contrast enhanced steady-state free precession cine cardiovascular magnetic resonance compared to single-photon emission computed tomography. J Cardiovasc Magn Reson 12:25
Kumar A et al (2011) CMR imaging of edema in myocardial infarction using cine balanced steady-state free precession. JACC Cardiovasc Imaging 4(12):1265–1273
Hammer-Hansen S et al (2017) Early gadolinium enhancement for determination of area at risk: a preclinical validation study. JACC Cardiovasc Imaging 10(2):130–139
Nordlund D et al (2017) Experimental validation of contrast-enhanced SSFP cine CMR for quantification of myocardium at risk in acute myocardial infarction. J Cardiovasc Magn Reson 19(1):12
Pedersen SF et al (2015) Dimethyl sulfoxide reduces microvascular obstruction and intramyocardial hemorrhage in a porcine ischemia–reperfusion model. Heart Res Open J 2(2):85–91
Tufvesson J et al (2016) Automatic segmentation of myocardium at risk from contrast enhanced SSFP CMR: validation against expert readers and SPECT. BMC Med Imaging 16:19
Sjogren J et al (2012) Semi-automatic segmentation of myocardium at risk in T2-weighted cardiovascular magnetic resonance. J Cardiovasc Magn Reson 14:10
Heiberg E et al (2008) Automated quantification of myocardial infarction from MR images by accounting for partial volume effects: animal, phantom, and human study. Radiology 246(2):581–588
Reeder SB, Herzka DA, McVeigh ER (2004) Signal-to-noise ratio behavior of steady-state free precession. Magn Reson Med 52(1):123–130
Acknowledgements
Funded by The Danish Diabetes Academy and supported by the Novo Nordisk Foundation (NNF17OC0028766) and The Health Research Fund of Central Denmark Region, Denmark.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hansen, E.S.S., Pedersen, S.F., Pedersen, S.B. et al. Validation of contrast enhanced cine steady-state free precession and T2-weighted CMR for assessment of ischemic myocardial area-at-risk in the presence of reperfusion injury. Int J Cardiovasc Imaging 35, 1039–1045 (2019). https://doi.org/10.1007/s10554-019-01569-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-019-01569-x