
Abstract
Transgender women are at higher risk of HIV infection, however, there is a lack of information about HIV infection and related factors among transgender women in Vietnam. From February 2018 to June 2018, 456 transgender women were recruited in the study using Respondent-Driven Sampling technique. Participants completed the computer-based questionnaire and were tested for HIV serostatus. Multivariable logistic regression was used to identify factors related to HIV infection. The prevalence of HIV infection was 77 (16.5%), of which 19 (24.7%) were not aware of their HIV-positive status prior to the study. Factors associated with HIV infection included popper use (aOR 2.01, p = 0.044) and having regular male partner(s) (aOR 0.42, p = 0.006). More efforts are needed to reduce the high prevalence of HIV infection, such as expanding the reach of HIV screening and prevention programs to the transgender women population, particularly for substance users.
Similar content being viewed by others

Introduction
Transgender women (TGW) are defined as people who are assigned the male sex at birth but then identify themselves as women [1, 2]. Due to both individual and social barriers, TGW often do not have easy access to appropriate screening for HIV infection [3, 4] even though the HIV epidemic among TGW is now recognized as a major global public health problem [2, 4, 5]. Previous studies found that HIV prevalence were 27.3% among TGW who are sex workers compared to 14.7% for those who do not engage in sex work [2]. This means that more than one of five TGW might be living with HIV. Additional studies reported that TGW had 48 times the risk of being HIV infected compared to all reproductive age adults [2].
The significant vulnerability to HIV infection and the high rate of HIV among TGW can be attributed to multiple factors, including unprotected sex (having sex without condoms or HIV preventive medications), substance use (including alcohol and stimulants), commercial sex work and discrimination [4, 6]. The risk of HIV transmission related to engaging in receptive anal intercourse without condoms or medications was 13 times higher than vaginal intercourse [7]. The high prevalence of substance use among TGW has been reported in various studies [4, 8] as a contributing factor for HIV. The survey conducted in San Francisco revealed that 58% of TGW used alcohol and 43.3% used substances (marijuana, methamphetamine, crack cocaine, and “club drugs”) [9]. Additionally, the high prevalence of commercial sex work within the TGW community was detected in previous findings ranging from 24 to 75% [2, 10, 11].
Vietnam is a developing country located in Southeast Asia with a population of more than 90 million people in 2019 [12]. The increase in the number of TGW has been reported recently as being due to socio-cultural integration. However, LGBT people are still stigmatized and exposed to various forms of discrimination and social isolation [13]. Our review of the literature found very few studies focusing on TGW that discussed the issue of HIV prevalence and related factors in Vietnam. There was only one study using a snowball sample targeted on TGW in Ho Chi Minh City in 2016 [13]. In this study, we applied a method of collecting and analyzing chain-referral data, respondent-driven sampling (RDS), which is expected to overcome the limitations of convenience sampling and generates unbiased population estimates within hidden or hard-to-reach populations [14, 15].
The aims of this study were to explore the HIV prevalence and to identify the risk factors associated with HIV infection among transgender women in Vietnam. The findings can help determine the ways in which services and policies can be tailored for this key population.
Methods
Study Setting and Participants
From February 2018 to June 2018, a cross-sectional study was conducted in Ho Chi Minh City, Vietnam. This is the largest city in the south of Vietnam, which is known in Vietnam as the epicentre of HIV infection with a high prevalence of HIV and illicit drug use. We recruited participants using RDS, a chain referral method, which has demonstrated success in recruiting hard-to-reach populations [14, 15]. Briefly, this approach involves the selection of a small number of “seeds”, i.e. individuals who are instructed to recruit others, with recruitment being limited to some maximum number.
Respondents at each wave selected or drove the next wave of sampling through their selection of other members of the target population. Particularly, the recruits of the seeds (wave 0) created wave 1, the recruits of wave 1 created wave 2, and so on. Every respondent in each wave had two opportunitiesto recruit other members. This process continued until the sample size was reached [14]. The seed and its corresponding waves were referred to a “chain”. The eligibility criteria for recruiting participants included (1) being a transgender woman, (2) being 18 years old or above; (3) having a study coupon from a peer participant, and (4) having the capacity and availability to answer the questionnaire within 20–25 min.
Sample Size and Sampling Procedures
Sample Size
The sample size was calculated to estimate the prevalence of HIV infection among TGW. With the expected prevalence of 18% [13], type 1 error rate of 0.05, the width of 95% confidence interval of 0.10, and the design effect of 2 [14], at least 454 participants were needed.
Selecting Seeds
During our formative work, seeds were carefully selected with assistance from six community-based organizations (CBOs) serving TGW. The diversity of seed traits played an important role in the quality of the study sample [14, 16]. In addition to the above-mentioned eligibility criteria for participants, the selected seeds had to have: (1) a large social network, (2) diversity in terms of HIV serostatus (i.e., there were both HIV+ and HIV− among seeds), (3) diversity in economic status, and (4) from various districts in the city. Each of six CBO leaders, who have the large network size and understand the context of the TGW community the most, were asked to list 10 potential seeds in order of priority. From these lists, ten seeds were selected based on the highest vote. A backup list of seeds was also prepared in case of all recruitment chains had dried up (i.e. stopped recruiting) before achieving the needed sample size. However, since this study achieved the needed sample size, the backup list was not used.
Recruitment Procedure
The data collection was conducted in five study sites covering different areas in Ho Chi Minh City. Each location had one to two CBO stations where participants came to answer the questionnaire and had an HIV finger-prick test.
Each seed received two recruitment coupons with unique numbers to invite two other TGW in their network into the study. Recruited peer participants were also provided two coupons to recruit their peers. According to the WHO guidelines on applying the respondent driven sampling technique for HIV/AIDS and sexually transmitted infection surveillance, the recruitment chain should reach at least four to six waves to reach equilibrium [14]. With the estimated sample size of 454 and ten seeds selected, two coupons for each recruiter are needed to reach the 6th wave. Each respondent received a sum of 50,000 VND (US$ 2.16) for their participation and a further sum of 25,000 VND (US $1.1) for each successfully recruited referral. The recruitment at each site occurred independently from the other sites. Therefore, all coupon recipients were referred to a specific study site. To make it easier to keep track of the recruitment waves, the coupon was only valid from 2 days to two weeks after it was issued.
TGWs who received the invited coupon came to the study sites to participate in the survey. To determine HIV prevalence, participants received a rapid HIV finger-prick testing conducted by CBO leaders and lay-testers who were trained to conduct HIV tests as their routine task. Those who have already known their positive HIV status were not provided with the HIV test. While waiting for the test result, participants were asked to answer the self-reported questionnaire which was designed as a web-based application run on computers. Participants were then informed of the rapid HIV test result and if the test showed a reactive result, the participants were referred to a HIV Testing and Counseling Clinic. There they were provided an confirmative HIV tests and support with enrollment into antiretroviral therapy (ART). In total, six waves of recruitment were produced with 456 TGWs participating and completing the questionnaire.
Measurements
Questionnaire
The questionnaire was designed to measure key variables related to the objectives of the study. Consultative meetings to improve the draft questionnaire were held with representatives of TGW from 6 CBOs in Ho Chi Minh City, CBO leaders, researchers and practitioners who have long-term experience in working with the LGBT community and HIV/AIDS patients. The questionnaire was pre-tested with 20 TGW and finalized before being applied to the survey.
The questionnaire contained information on socioeconomic characteristics, sexual behaviors and condom use with different types of sexual partners, criminal justice involvement, HIV screening, and substance use.
HIV Rapid Test
Blood was taken for HIV screening using a finger-prick blood-based rapid diagnostic test (Alere Determine™ HIV 1/2 antibody).
Statistical Analysis
To adjust for potential biases in recruitment, we calculated the sampling weights and incorporated them into all analysis steps. The weights were the inverse of the approximate probability of recruitment based on participants’ network sizes and differential recruitment patterns. The weight estimates were conducted using RDS Analyst (RDS-A) version 0.71 with Gile’s Successive Sampling (Gile’s SS) method [17].
The frequencies and weighted percentages were used to describe categorical variables, weighted means, and 95% CI to describe quantitative variables. In bivariate analysis, odds ratio (OR) and 95% CI generated from logistic regression were used to evaluate the relationship between HIV serostatus and each participants’ characteristic. To identify factors related to HIV infection, multivariable logistic regression was carried out using the stepwise backward selection procedure with the cutoff of p ≤ 0.2 [18].
Recruitment diagrams were created using NetDraw 2.136 (Analytic Technologies, Harvard, MA). Stata version 16 (Stata Corporation, College Station, TX) with package “svy” was used to compute descriptive statistics and modeling.
Ethics
All procedures performed in this study were in accordance with the ethical standards of the Biomedical Research Ethics Committee at the University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam (approval number: 268/DHYD-HDDD). Written informed consent was obtained from all individual participants included in the study.
Results
The recruitment chains and response rates in six waves are summarized in Fig. 1. The sampling procedure included six waves with an overall response rate of 58.5%. In the first three waves (0, 1st, 2nd), the response rate was 100%. These rates fell in the following waves 3rd, 4th, 5th, and 6th, which were 97.5%, 83.3%, 41.2%, and 33.2%, respectively.

Recruitment chains and response rates of six waves
Among 456 participants, 58 had been diagnosed with HIV infection prior to the study and were not tested with the rapid test. We found 19 participants with reactive HIV test results with confirmation who were not aware of their HIV status prior to the study. A total of 77 (16.5%) participants had positive HIV serostatus (Table 1). Differences in correlates between TGW who aware and unaware of the positive HIV status are shown in the Supplementary materials.
As shown in Table 1, the current age mean was 26.7 years. The majority of the participants had completed high school or had some higher education (75.5%) and had never been married (98.5%). The most common main occupations reported were staff/entertainment (65.3%) and business/services (20.2%), 8.9% of them reported their job as being a sex workers. More than half of participants (51.5%) reported an average monthly income between US$129–214. The average age at which participants reported their first internal identification was 17.6 years with 19.6 the age at which they came out in public as female.
The results of hormone use and interventions are summarized in Table 2. Forty-seven percent of TGW reported using of hormones, and 66.5% of those used hormones without prescriptions. More than one-third of participants (39.3%) reported that they had undergone gender-affirming surgery.
Sexual behaviors between TGW with HIV+ and HIV− are shown in Table 3. Most participants (98.2%) had sexual intercourse with others in the past, 40.8% reported having regular male partner(s), and 27.0% had non-regular sex partner(s). The percentage of participants reported having both receptive and insertive intercourse with partner(s) was 47.5%.
As shown in Table 3, more than one-fourth of participants reported using alcohol two to four times per month in the past 12 months and 29.7% reported drinking three to four standard drinks of alcohol per week. Sixty percent of the participants used alcohol 2 h before having sexual intercourse in the last 12 months. The percentages of using amphetamine-type stimulants (Yama, Crystal Ice, Ecstasy), poppers, and cannabis were 24.7%, 27.3%, and 10.0%, respectively. The prevalence of TGW using ATS/poppers 2 h before having sexual intercourse in the last 12 months was 31.8%.
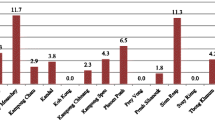
Figure 2 illustrates the factors associated with HIV infection in multivariable logistic regression analyses. After adjustment for other covariates, participants using poppers were more likely to be infected by HIV than those were non-popper use (aOR 2.01, 95% CI 1.02–3.98, p = 0.044). In contrast, participants who had regular male partner(s) had the lower odds of having HIV infection compared to those who did not (aOR 0.42, 95% CI 0.23–0.78, p = 0.006). TGW who had casual sex partners had a higher likelihood of HIV infection than those without casual sex partners, however, the difference was not statistically significant (aOR 1.70, 95% CI 0.85–3.37, p = 0.130).

Multivariable logistic model of factors related to HIV infection among TGW in Vietnam
Discussion
This study revealed an HIV prevalence of 16.5% among TGW in Ho Chi Minh City. This prevalence was higher than the findings from other countries, including Cambodia (5.9%) [19], China (14.8%) [20] and Malaysia (11.7%) [6]. This observed prevalence highlights the high risk for HIV infection among transgender women in Vietnam and was consistent with global literature regarding the high burden of HIV infection among the transgender population [5].
The prevalence found in this study was slightly lower than the prevalence of 18.0% reported in the study on 205 TGW conducted in Ho Chi Minh City in 2016 [13]. Although we have no clear explanation for the differences in HIV prevalence in TGW, we suggest that it might be related to the sampling variation in the two researches. The previous study recruited participants using the convenience sampling method [13] that might limit the ability to generalize the results to the study population [14, 21]. This study was conducted with a larger sample size with the RDS method. This sampling method was demonstrated to be successful in recruiting hard-to-reach populations [14, 15]. Moreover, the analysis took into account the potential biases in recruitment by applying RDS weights and made the results more generalizable [14, 22].
Over the last three years, there have been increasingly interventions that supported TGW in terms of raising their awareness of gender equality, gender identity rights, and health care rights including HIV prevention and treatment. Various organizations led by TGW and other sexual minorities have been reaching TGW with HIV and STI prevention information and referral to diagnosis and treatment services [23]. Thanks to recent progress in HIV/AIDS prevention and control in Vietnam, there was a two-thirds reduction in HIV prevalence in the population over the 10-year period from 2007 to 2017 [24, 25], which might be linked to the lower prevalence in TGW.
Nearly one-fourth (19/77, 24.7%) of those who had HIV reactive tests reported that they were not aware of their HIV-positive status before they participated in the study. These tests were provided at the CBO which was most convenient for participants. The importance of CBO in screening, detecting new cases of HIV infection in the community as well as in referring TWG to the health care and prevention services has been promotedby the Centers for Disease Control and Prevention (CDC) [5]. Since 2016, PEPFAR through USAID has piloted community-based HIV testing (lay-test) in Vietnam [23]. Under the program, CBOs in HCMC have been trained and started conducting lay-test at their offices. The introduction of community-based HIV testing has increased the number of vulnerable and high risk-taking groups such as TGW to know their HIV status [23], which is the first of the three major HIV-controls 90% tested, –90% on ARV and –90% having viral load suppression. The Government of Vietnam has committed to these targets [26]. Furthermore, prevention methods, such as condom use and Pre-Exposure Prophylaxis (PrEP) medication are also potential to reduce the high HIV prevalence among TGW. In literature, there are many studies have indicated the crucial role of condom use and PrEP in protecting against HIV infection in TGW population [27,28,29]. Therefore, CBOs should be provided with resources to expand their reach and services to TGW population, not only in HIV screening but also in community mobilization, coordinated referral networks, and prevention services, such as condom or PrEP medication distribution.
This study also reported essential findings related to factors associated with HIV infection among transgender women in Vietnam. The HIV rate among transgender women using poppers was twice as high compared with those who did not use poppers. Popper use has been well documented in previous studies as a predictor of HIV infection [30, 31]. There might be two explanationsfor this result. Firstly, TGW who engage in receptive anal intercourse might use poppers to increase dilation of the anal sphincter, reducing possible discomfort during anal intercourse. Furthermore, some previous studies showed that the receptive role in the anal intercourse was associated with decreased condom use, since those who took the insertive position had more autonomy of determining condom use [32]. Secondly, like other club drugs, poppers also had the pharmacological and neurological effects on sexual behaviors, such as promoting sexual desire, reducing sexual inhibition, modifying mental states, and decreasing physical experiences of pain [33, 34]. This might further increase risks of HIV transmission during sexual intercourse since these effects of poppers can prevent users from using condoms and lead to group sex behaviors [34, 35].
This study revealed that HIV prevalence among transgender women with a regular male partner was significantly lower compared with those who did not have a regular male partner. This finding is understandable as having a regular partner was equivalent to intercourse with fewer partners, thus, decreased the risk of exposure to HIV than others.
In Vietnam, with socio-cultural integration, there has been an increase in the number of TGW. However, TGW are still stigmatized and exposed to various forms of discrimination. Accessing health care services by TGW is still limited, especially for HIV prevention and care interventions. Therefore, reaching out to such a hard-to-reach population plays a key role in the success of an intervention program. In this study, the RDS approach was shown to be effective in reaching the TGW community and in detecting new HIV cases, with 19 new cases out of 456 participants. The RDS is also considered as a relatively simple and low-cost way. Therefore, HIV intervention programs can be tailored based on such peer network approach to expand their reach to TGW as well as other members of the LGBT community.
Limitations
The findings of this study should be interpreted in the context of potential limitations. First, all the participants in our study were from Ho Chi Minh City which is the very large city in Vietnam and might not be generalizable to all TGW in other areas. Second, since this study was a cross-sectional study, the association between HIV infection and related factors may not demonstrate causal relationships.
Conclusions
This study found that HIV prevalence among transgender women in Vietnam was higher than other populations and countries in the region. Using poppers increased the likelihood of HIV infection among transgender women, whereas, transgender women who had regular male partner(s) had lower odds of HIV infection. More efforts are needed to reduce this high prevalence, such as expanding the reach of HIV screening and prevention programs implemented by CBOs to the TGW population, particularly for those who use substances.
Availability of Data and Material
Available upon request to the corresponding author.
Abbreviations
- ART:
-
Antiretroviral therapy
- CBO:
-
Community-based organizations
- CI:
-
Confidence Interval
- HCMC:
-
Ho Chi Minh City
- HIV:
-
Human immunodeficiency virus
- LGBT:
-
Lesbian, gay, bisexual, and transgender
- PEPFAR:
-
The President’s Emergency Plan For AIDS Relief
- PrEP:
-
Pre-Exposure Prophylaxis
- RDS:
-
Respondent-driven sampling
- STI:
-
Sexually transmitted infections
- TGW:
-
Transgender women
- USAID:
-
The United States Agency for International Development
- USD:
-
United States dollar
- VND:
-
Vietnamese dong
References
Fuss J, Auer MK, Briken P. Gender dysphoria in children and adolescents: a review of recent research. Curr Opin Psychiatry. 2015;28(6):430–4.
Poteat T, Reisner SL, Radix A. HIV epidemics among transgender women. Curr Opin HIV AIDS. 2014;9(2):168–73.
Gonzales G, Henning-Smith C. Barriers to care among transgender and gender nonconforming adults. Milbank Q. 2017;95(4):726–48.
Nuttbrock L, Bockting W, Rosenblum A, Hwahng S, Mason M, Macri M, et al. Gender abuse, depressive symptoms, and HIV and other sexually transmitted infections among male-to-female transgender persons: a three-year prospective study. Am J Public Health. 2013;103(2):300–7.
Centers for Disease Control and Prevention. HIV and transgender people. https://www.cdc.gov/hiv/group/gender/transgender/indexhtml. Accessed 27 Nov 2019.
Wickersham JA, Gibson BA, Bazazi AR, Pillai V, Pedersen CJ, Meyer JP, et al. Prevalence of human immunodeficiency virus and sexually transmitted infections among cisgender and transgender women sex workers in Greater Kuala Lumpur, Malaysia: results from a respondent-driven sampling study. Sex Transm Dis. 2017;44(11):663–70.
Centers for Disease Control and Prevention. Anal sex and HIV risk. https://www.cdcgov/hiv/risk/analsex.html. Accessed 27 Nov 2019.
Gupta S, Sarpal SS, Kumar D, Kaur T, Arora S. Prevalence, pattern and familial effects of substance use among the male college students—a north Indian study. J Clin Diagn Res. 2013;7(8):1632–6.
Santos G-M, Rapues J, Wilson EC, Macias O, Packer T, Colfax G, et al. Alcohol and substance use among transgender women in San Francisco: prevalence and association with human immunodeficiency virus infection. Drug Alcohol Rev. 2014;33(3):287–95.
Herbst JH, Jacobs ED, Finlayson TJ, McKleroy VS, Neumann MS, Crepaz N, et al. Estimating HIV prevalence and risk behaviors of transgender persons in the United States: a systematic review. AIDS Behav. 2008;12(1):1–17.
Garofalo R, Deleon J, Osmer E, Doll M, Harper GW. Overlooked, misunderstood and at-risk: exploring the lives and HIV risk of ethnic minority male-to-female transgender youth. J Adolesc Health. 2006;38(3):230–6.
Vietnam General Statistics Office. Average population by location. https://www.gsogov.vn/defaultaspx?tabid=217. Accessed 27 Nov 2019.
Colby D, Nguyen NA, Le B, Toan T, Thien DD, Huyen HT, et al. HIV and Syphilis prevalence among transgender women in Ho Chi Minh City. Vietnam AIDS Behav. 2016;20(Suppl 3):379–85.
World Health Organization. Introduction to HIV/AIDS and sexually transmitted infection surveillance: module 4: introduction to respondent-driven sampling. Geneva: World Health Organization; 2013.
Kimani SM, Watt MH, Merli MG, Skinner D, Myers B, Pieterse D, et al. Respondent driven sampling is an effective method for engaging methamphetamine users in HIV prevention research in South Africa. Drug Alcohol Depend. 2014;143:134–40.
Wylie JL, Jolly AM. Understanding recruitment: outcomes associated with alternate methods for seed selection in respondent driven sampling. BMC Med Res Methodol. 2013;13:93.
Handcock MS, Fellows IE, Gile KJ. RDS analyst: software for the analysis of respondent-driven sampling data, version 0.71. 2014.
Zellner D, Keller F, Zellner GE. Variable selection in logistic regression models. Commun Stat Simul Comput. 2004;33(3):787–805.
Chhim S, Ngin C, Chhoun P, Tuot S, Ly C, Mun P, et al. HIV prevalence and factors associated with HIV infection among transgender women in Cambodia: results from a national Integrated Biological and Behavioral Survey. BMJ Open. 2017;7(8):e015390.
Yan H, Xiao W, Chen Y, Chen Y, Lin J, Yan Z, et al. High HIV prevalence and associated risk factors among transgender women in China: a cross-sectional survey. J Int AIDS Soc. 2019;22(11):e25417.
Heckathorn DD. Snowball versus respondent-driven sampling. Sociol Methodol. 2011;41(1):355–66.
Salganik MJ, Heckathorn DD. Sampling and estimation in hidden populations using respondent-driven sampling. Sociol Methodol. 2004;34:193–239.
Vu BN, Green KE, Thi Thu Phan H, Hung Tran M, Van Ngo H, Hai Vo S, et al. Lay provider HIV testing: a promising strategy to reach the undiagnosed key populations in Vietnam. PLoS ONE. 2018;13(12):e0210063.
Vietnam Government. The national strategy on HIV/AIDS prevention and control in Viet Nam till 2010 with a vision to 2020. Hanoi: Vietnam Government; 2004.
Vietnam Ministry of Health Vietnam Administration of HIV/AIDS Control. Report on HIV/AIDS prevention and control in 2017 and key tasks in 2018. Hanoi: Vietnam Ministry of Health; 2017.
Vietnam Ministry of Health. Optimizing Viet Nam’s HIV response: an investment case. Hanoi: MOH; 2014.
Bórquez A, Guanira JV, Revill P, Caballero P, Silva-Santisteban A, Kelly S, et al. The impact and cost-effectiveness of combined HIV prevention scenarios among transgender women sex-workers in Lima, Peru: a mathematical modelling study. Lancet Public Health. 2019;4(3):e127–e136136.
Burns DN, Grossman C, Turpin J, Elharrar V, Veronese F. Role of oral pre-exposure prophylaxis (PrEP) in current and future HIV prevention strategies. Curr HIV/AIDS Rep. 2014;11(4):393–403.
Pawa D, Firestone R, Ratchasi S, Dowling O, Jittakoat Y, Duke A, et al. Reducing HIV risk among transgender women in Thailand: a quasi-experimental evaluation of the sisters program. PLoS ONE. 2013;8(10):e77113.
Haverkos HW, Kopstein AN, Wilson H, Drotman P. Nitrite inhalants: history, epidemiology, and possible links to AIDS. Environ Health Perspect. 1994;102(10):858–61.
Lampinen TM, Mattheis K, Chan K, Hogg RS. Nitrite inhalant use among young gay and bisexual men in Vancouver during a period of increasing HIV incidence. BMC Public Health. 2007;7(1):35.
Zhang H, Lu H, Pan SW, Xia D, Zhao Y, Xiao Y, et al. Correlates of unprotected anal intercourse: the influence of anal sex position among men who have sex with men in Beijing. China Arch Sex Behav. 2015;44(2):375–87.
Yang X, Xia G. Causes and consequences of increasing club drug use in China: a descriptive assessment. Subst Use Misuse. 2010;45(1–2):224–39.
Drumright LN, Patterson TL, Strathdee SA. Club drugs as causal risk factors for HIV acquisition among men who have sex with men: a review. Subst Use Misuse. 2006;41(10–12):1551–601.
Prestage G, Down I, Grulich A, Zablotska I. Sex partying among gay men in Sydney, Melbourne and Brisbane. Australia AIDS Behav. 2011;15(2):298–304.
Acknowledgements
The authors would like to thank all TGW who participated in this study, as well as the individuals and institutions that made this research possible: Dr. Cathy J. Reback from Friends Community Center and UCLA Center for HIV Identification, Prevention and Treatment Service. Dr Sherry Larkins from University of California, Los Angeles. Nguyen Ngoc Tuan, Sa Liem, Pham Hong Son, Nguyen Minh Thuan, Huynh Tien Dat, Trang Van Toan from Community-based organizations at Ho Chi Minh City, Vietnam. We would like to thank Dr. Kevin P. Mulvey and Dr. Bruce G. Trigg for editing the language contents of this paper.
Funding
This study was funded by USAID Enhanced Community HIV Link-Southern Project.
Author information
Authors and Affiliations
Contributions
VTTV: designed the study, coordinated data collection, and provided editorial input; KQL: designed the study, coordinated data collection, conducted statistical analyses, drafted and revised the manuscript; LHTCH: designed the study, coordinated data collection, and provided editorial input; HTNA: drafted and revised the manuscript; NVN: participated in the study design, provided editorial input; VVT: coordinated data collection, and provided editorial input; NLL: participated in the study design, provided editorial input; HHH: drafted and revised the manuscript; TVAP: participated in the study design, coordinated data collection, and provided editorial input; NNNT: participated in the study design, coordinated data collection, and provided editorial input; DVD: participated in the study design, provided editorial input. All authors read and approved the final submitted manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Vi, V.T.T., Long, K.Q., Hong, L.H.T.C. et al. HIV Prevalence and Factors Related to HIV Infection Among Transgender Women in Vietnam: A Respondent Driven Sampling Approach. AIDS Behav 24, 3132–3141 (2020). https://doi.org/10.1007/s10461-020-02867-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-020-02867-5