
Abstract
This is a case of an ovarian actinomycosis diagnosed as a complex ovarian cyst by ultrasound in asymptomatic patient. The ovarian tumour markers were within normal. The tube and ovary were removed laparoscopically. She received 2 weeks of daily IV 1 g of ceftriaxone, followed by 6 months of oral amoxicillin. CT scan did not show evidence of actinomycosis elsewhere. She did not give any history of intrauterine contraceptive use.
Similar content being viewed by others


Introduction
Actinomycosis is an uncommon, chronic granulomatous disease caused by filamentous, gram-positive, non-spore-forming anaerobic or microaerophilic bacteria. Actinomyces Israelii is the major human pathogen [1].
Actinomycetes are commensal inhabitants of the oral cavity and intestinal tract [2], but acquire pathogenicity through invasion of breached or necrotic tissue. As the infection progresses, granulomatous tissue, extensive reactive fibrosis and necrosis, abscesses, draining sinuses and fistulas are formed [3]. The disease tends to spread by contiguity. Lymphadenopathy is not a clinical feature. Haematogenous dissemination is also rare [4]. Pelvic actinomycosis is typically associated with the use of intrauterine device (IUD) [5–12].
Case presentation
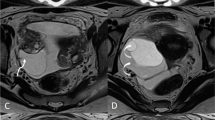
A 31-year-old lady was referred to the gynaecology clinic because of an ultrasound finding of a complex right ovarian cyst of 54 × 49 × 45 mm (Fig. 1). The ultrasound was performed because of the past history of severe right iliac fossa pain which lasted only for a day and subsided completely after. The ovarian tumour markers (CA125, CA19-9, CEA, BHCG, lactic dehydrogenase, alpha feto protein) were within normal values. She has only one child whom she delivered vaginally. The combined pills were her method for contraception. She had no previous history of use of intrauterine contraceptive device. All her previous cervical smears were negative and none of them showed actinomycosis. Preoperative full blood count revealed normal white cell count. Laparoscopy showed signs of pelvic infection in the form of omental adhesions to the anterior parietal peritoneum and adhesions between the liver and the diaphragm (Fitz Hugh Curtis syndrome). There was right adnexal mass. The ovary could not be visualized separate from the mass. This picture was suggestive of chronic inflammatory mass. The right adnexal mass was removed intact through the laparoscopic Endo Catch. The cyst contained yellowish thick material.

Ultrasound images of the tubo-ovarian abscess
The histology report (Figs. 2, 3 and 4) came as right tubo-ovarian abscess with actinomyces like organisms. Daily intravenous ceftriaxone (1 g) were given through a long line for 2 weeks. This is followed by 6 months of oral amoxicillin.

The tubo-ovarian abscess after surgical removal

Microscopy. Actinomycosis. H&E ×400

Microscopy. Actinomycosis. Grocott silver ×400
Postoperative CT scan did not show any other lesion in the abdomen or the pelvis.
Discussion
Ovarian actinomycosis is rare because the structure of the ovary is resistant to surrounding inflammatory disease [13]. It has been assumed that bacteria enter the ovary when the surface is broken by the process of ovulation. Timely detection and treatment prevents complications such as pelvic actinomycotic masses leading to frozen pelvis. A delay in diagnosis can even be fatal [14]. Direct extension from established ileocaecal actinomycosis was believed to involve the female genital tract [15].
Computed tomography is the most useful imaging modality. It determines the location and extent of the disease, occasionally contributes to an accurate preoperative diagnosis through fine needle aspiration and is used for monitoring the radiologic response to treatment on follow-up examinations [16].
Although actinomycetes are sensitive to penicillin, surgery is usually performed to eradicate the inflammatory process [17]. The usual recommended antibiotic regimen is intravenous penicillin G (18–24 million units/day) for 2–6 weeks, followed by oral penicillin or amoxicillin for 6–12 months [18].
In this case, there were no clinical features to suggest that the adnexal mass is an ovarian abscess. CT/MRI scan has not been done initially, as the tumour markers were normal. However, preoperative diagnosis of an ovarian abscess by CT/MRI scan may help to speed the surgery. The laparoscopic findings of omental and liver adhesions were suggestive of pelvic infection. It is very difficult to know how she gets infected with actinomycosis as there was no history of IUD use or ileocaecal disease. Postoperative CT scan was requested to exclude any hidden source of actinomycosis. Long-term treatment of penicillin was required to minimize the recurrence of actinomycosis and to treat other unrecognized source.
Very few cases of ovarian actinomycosis without a previous history of IUD have been reported [19–21].
Conclusion
Tubo-ovarian actinomycosis was diagnosed in a healthy woman who had never used the intrauterine contraceptive device and with no past history of pelvic infection. Treatment of actinomycosis consists of adequate surgery, such as drainage of the abscess and reduction of infected tissue and long-term antibiotic therapy.
References
Iwasaki M, Nishikawa A, Akutagawa N et al (2003) A case of ovarian actinomycosis. Infect Dis Obstet Gynecol 11:171–173
Dayan K, Neufeld D, Zissin R et al (1996) Actinomycosis of the large bowel: unusual presentations and their surgical treatment. Eur J Surg 162:657–660
Cintron JR, Del Pino A, Duarte B et al (1996) Abdominal actinomycosis. Dis Colon Rectum 39:105
Wong VK, Turmezei TD, Western VC (2011) Actinomycosis. BMJ 343:d6099
Schmidt WA (1982) IUDs, inflammation and infection: assessment after two decades of IUD use. Hum Pathol 13:878–881
Hager WD, Douglas B, Majumadar B et al (1979) Pelvic colonization with actinomyces in women using intrauterine contraceptive devices. Am J Obstet Gynecol 135:680–684
Henderson SR (1973) Pelvic actinomycosis associated with an intrauterine device. Obstet Gynecol 41:726–732
Muller-Holzner E, Ruth NR, Abfalter E et al (1995) IUD-associated pelvic actinomycosis: a report of five cases. Int J Gynecol Pathol 14:70–74
Fiorino AS (1996) Intrauterine contraceptive device associated actinomycotic abscess and actinomyces detection on cervical smear. Obstet Gynecol 87:142–149
Gupta PK, Malkani PD, Bhasin K et al (1971) Cellular response in the uterine cavity after IUD insertion. Contraception 4:375–384
Burkman R, Schlesselman S, Mc Caffrey L et al (1982) The relationship of genital tract actinomycetes and the development of pelvic inflammatory disease. Am J Obstet Gynecol 143:585–589
Bhagavan BS, Gupta PK (1978) Genital actinomycosis and intrauterine contraceptive devices. Cytopathologic diagnosis and clinical significance. Hum Pathol 9:567–578
Koshiyama M, Yoshida M, Fujii H et al (1999) Ovarian actinomycosis complicated by diabetes mellitus simulating advanced ovarian carcinoma. Eur J Obstet Gynecol Reprod Biol 87:95–99
Munot MV, Tambekar R, Veerkar V et al (2007) Actinomycotic salpingitis: a complication of misplaced Cu-T. J Obstet Gynecol India 57:442–443
Shroff CP, Deodhar KP, Patkar VD et al (1981) Tubo-ovarian actinomycosis. J Postgrad Med 27:29–32
Harris LA, De Cosse JJ, Dannenberg A (1989) Abdominal actinomycosis: evaluation by computed tomography. Am J Gastroenterol 84:198
Wagenlehner FME, Mohren B, Naber KG et al (2003) Abdominal actinomycosis. Clin Microbiol Infect 9:881–885
Russo TA (1995) Agents of actinomycosis. In: Mandell GL, Bennett JE, Dolin R (eds) Principles and practice of infectious diseases, 4th edn. Churchill Livingstone, New York, pp 2280–2288
Singh S, Batra A, Dua S et al (2012) Ovarian actinomycosis: presenting as ovarian mass without any history of intrauterine copper device. J Global Infect Dis 4:222–223
Petrone L, Sivalingam J, Vaccaro A (1999) Actinomycosis-an unusual case of an uncommon disease. J Am Board Fam Pract 12:158–161
Marwah S, Marwah N, Singh I et al (2005) Ovarian actinomycosis in absence of intrauterine contraceptive device: an unusual presentation. Acta Obstet Gynecol Scand 84:602–603
Acknowledgments
The author is grateful to Dr. Emma Hutley (consultant microbiologist) and Dr. Richard Stitson (consultant histopathologist) for their help in preparation of this article.
Conflict of interest
Magdy Moustafa declares that he has no conflict of interest.
Informed consent was obtained from the patient for which identifying information is included in this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Moustafa, M. Tubo-ovarian abscess secondary to actinomycosis: unexpected presentation and its treatment. Gynecol Surg 12, 53–55 (2015). https://doi.org/10.1007/s10397-014-0871-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10397-014-0871-3