
Abstract
Aim
The “JOBS Program” is an intervention for the unemployed to promote health and labor market integration and has shown positive effects in the USA and Finland. The aim of this confirmatory study was to investigate whether the JOBS Program produces similar effects in Germany.
Subject and methods
We applied a multicenter randomized controlled trial to compare an intervention group (IVG) with a waiting control group (WCG) before (T0; n = 94) and about 6 months after (T2; n = 43) the intervention.
Results
Although the proportion of long-term unemployed (≥ 12 months) in the intervention group at T2 was high (88.4 %; n = 38), the JOBS Program was beneficial concerning our primary outcomes: Compared to the WCG, the regression estimated that the IVG had (1) a 3.48-point higher level of self-esteem (p = 0.032; scale range: 10–50 points), (2) a 4.93-point higher level of generalized self-efficacy expectations (p = 0.002; scale range: 10–50 points), (3) a 0.41-point higher level of general health (p = 0.016; scale range: 1–5 points), and (4) a 2.04-point lower level of unemployment-related mental burden (p = 0.028; scale range: 10–40 points).
Conclusion
This study provides evidence for the effectiveness of the JOBS Program with respect to the above outcomes, and for older and long-term unemployed, suggesting the benefit of regular implementation for different groups of unemployed people in Germany.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Compared with people who are employed, those who are unemployed are more likely to suffer from somatic health problems such as cardiovascular or musculoskeletal disorders (Kroll et al. 2016; Lampert et al. 2018) and are at higher risk of mortality due to diseases (Roelfs et al. 2011; Garcy and Vågerö 2012) and suicide (Milner et al. 2014). Unemployed people are also most affected by mental health impairments (Paul and Moser 2009; Kim and Knesebeck 2016; McKee-Ryan et al. 2005; Lamberg et al. 2010). Internationally, there are many interventions aimed at improving the psychological well-being of unemployed people and increasing the chances of (re-)employment (Hollederer 2021, 2019; Hult et al. 2020; Paul and Hollederer 2023; Arena et al. 2023). One of those interventions is the so-called JOBS Program. It was developed in the 1980s by psychologists at the Prevention Research Center of the Institute for Social Research, University of Michigan, USA. It is aimed primarily at increasing personal resources including self-confidence, self-esteem, and self-efficacy (Curran et al. 1999; Caplan et al. 1989; Vinokur et al. 1995), and with that the mental health of the participants as well. The JOBS Program has been applied in different countries and has shown positive results in improving mental health and/or labor market integration, for example, in the United States (Caplan et al. 1989; van Ryn and Vinokur 1992; Vinokur et al. 1991b; Price et al. 1992), Finland (Vuori et al. 2002; Vuori and Silvonen 2005), Israel (Shirom et al. 2008), Ireland (Reynolds et al. 2010), the Netherlands (Brenninkmeijer and Blonk 2012), China (Price and Vinokur 2014), and South Africa (Paver et al. 2020b).
Since 2020, the JOBS Program has also been offered in Germany, where it is called the JOBS Program Germany. It was introduced as a pilot project in the framework of the overarching program called “Linking of Employment and Health Promotion in the Community Setting.” Within this program, the Federal Centre for Health Education (BZgA) and the National Association of Statutory Health Insurance Funds (GKV-Spitzenverband) were involved in cooperation with the German Federal Employment Agency.
The pilot implementation of the JOBS Program Germany was scientifically conducted and evaluated by the University of Kassel, Germany, to examine whether the JOBS Program would yield similar effects in Germany as the studies mentioned above. In this sense, this scientific evaluation was designed as a confirmatory research approach and was intended to follow the methods and objectives of the abovementioned evaluation studies successfully conducted by Vinokur et al. (2000) in the United States and by Vuori et al. (2002) in Finland.
This confirmatory study examined the effects of the JOBS Program on personal resources such as self-esteem and self-efficacy expectations as well as on health-related outcomes such as general health and mental burden related to unemployment among the unemployed in Germany. Seven JOBS training sessions were held in six different centers, and 94 unemployed individuals took part in the first interview (T0, prior to the training). We have already published promising results from the post-test data (T1, immediately after the training) (Hollederer and Jahn 2023), and here we are able to report relevant results from the follow-up (about 6 months after the training). This concerns the effects of the training on the participants’ self-esteem, generalized self-efficacy expectations, general health status, and level of unemployment-related mental burden.
Regarding these outcomes, we hypothesized that the intervention would increase the participants’ (i) self-esteem, (ii) their generalized self-efficacy expectations, and (iii) their general health status. Additionally, the JOBS training would (iv) decrease the level of unemployment-related mental burden. Following the studies by Vinokur et al. (2000) and Vuori et al. (2002), we also examined previously identified effect moderations. We hypothesized that (v) the level of depressive symptoms before the JOBS Program training (hereafter "JOBS training") would moderate the effect of the intervention on mental health outcomes, in that the training would show stronger effects among those who suffered more from unemployment-related mental burden. We further hypothesized that (vi) the duration of unemployment before the JOBS training would also moderate the effects of training on unemployment-related mental burden.
Materials and methods
Trial design, recruitment, and data collection
This confirmatory study was designed as a multicenter, non-blinded, two-arm, parallel-group, randomized controlled trial (see details on methodology in (Hollederer et al. 2021), and the study design was based on two abovementioned evaluation studies from the USA and Finland (Vinokur et al. 2000; Vuori et al. 2002).
During this pilot implementation in Germany, volunteer employment agencies were asked to inform their clients about the JOBS Program and to invite them to voluntarily participate in the JOBS training and the evaluation study. If clients were interested, they were invited to an information event where they received detailed information about the training and the study. If participants provided their informed consent, they were called via telephone to conduct the first interview prior to the JOBS training (T0).
All interviews were conducted by computer-assisted telephone interviews (CATI) with Voxco software by the Institute for Social Sciences and Communication (SOKO; https://soko-institut.de/) on behalf of BZgA. During the first interview (T0), the participants were randomly assigned to either the intervention group (IVG) or the waiting control group (WCG) (1: 1 ratio) and invited to the JOBS training. After the JOBS training, both groups were interviewed a second time (as soon as possible, but within 4 weeks after the training [T1]) and a third time (about 6 months after the training [T2]). WCG participants were offered free participation in JOBS training after the study was completed.
Adults who were registered as unemployed with their local employment agency and who were able to independently complete the CATIs in German were eligible to be study participants. Due to occupational health and safety regulations during the COVID-19 pandemic, the employment agencies were not allowed to have personal contact with their clients for a large period of the recruitment (Hollederer et al. 2023). Therefore, the employees of the employment agencies were faced with the challenge of inviting their clients by phone or e-mail. The countrywide recruitment was expected to start in April 2021 and to be finished by August 2021. Due to constraints imposed by COVID-19 pandemic-related infection control measures, the main study phase of the JOBS training sessions took place between March and December 2022 (subsequent to a pretest that was conducted to test all study processes).
Intervention
The JOBS Program applies elements of social learning based on Albert Bandura's social cognitive learning theory (Bandura 1971, 1977b) and self-efficacy theory (Bandura 1977a, 1986, 2004).
The JOBS Program training is designed as a multimodal workshop, usually lasting 5 days, with 4 to 5 hours each day. Under the guidance of two certified JOBS Program trainers, participants develop and improve their practical job search skills in small groups of 15 to 20 individuals. In terms of methods, the focus is on the following basic elements and group techniques:
-
1.
job search skills training
-
2.
active teaching and learning methods
-
3.
trained (certified) trainers for program delivery
-
4.
supportive learning environment
-
5.
inoculation against setbacks.
Typical activities include job search on social networking sites, compiling information for interviews, simulated job interviews, thinking in terms of employer perspectives, and evaluating job offers. Another essential component of the JOBS Program is the inoculation against setbacks during the job search. To be prepared against such discouraging experiences, a stress inoculation training is applied. The group anticipates potential difficulties in specific job search situations and develops appropriate problem-solving strategies. All training content is taught using active teaching and learning methods. The aim is to identify the participants' prior knowledge and skills and incorporate them into the various exercises. These are characterized, for example, by group discussions, brainstorming, and role play. Two other essential elements permeate all training activities:
-
1.
Trainers provide continuous supportive feedback to participants and encourage appreciative, respectful interaction among the participants. In this way, they create an atmosphere of social support. Trainers also show empathy for participants' concerns and feelings and encourage them to use appropriate coping strategies (Curran et al. 1999).
-
2.
Another training principle is the so-called referent power. The trainers strive to gain high esteem, trust, and respect from the participants through competent teaching, self-revelation, reduced social distance, and empathic support.
If both components can be successfully implemented, this appreciative and supportive training situation opens up better opportunities for the trainers to exert a positive influence on the participants' self-efficacy expectations, on their self-esteem, and thus on their motivation to apply for a job (Curran et al. 1999; Caplan et al. 1989).
Specifications of the JOBS Program Germany
The JOBS training sessions were free of charge, lasted approximately 20 hours (conduct within 1 to 2 weeks) in groups of eight to 15 participants, and were led by two certified JOBS Program trainers (BZgA and GKV-Spitzenverband 2021). One trainer had to have been either qualified for adult education or professionally active in employment services. The other trainer had to be unemployed or at least to have experience with unemployment. Both had to undergo training to become certified as JOBS Program trainers. An evaluation of the JOBS Program Germany from the trainers' perspective was published by (Jahn et al. 2023).
Predictor variables and outcome measures
All predictor variables and outcomes were measured by means of a questionnaire developed by the research team at the University of Kassel. During the questionnaire-based CATI, data were collected on demographic characteristics, work and unemployment history, job search intensity, re-employment, self-esteem, self-efficacy expectations, life satisfaction, and physical and mental health. Demographic characteristics were assessed using standard survey questions concerning age, gender, marital status, education, occupation, and length of unemployment. The level of education was determined by asking for the highest level of formal schooling completed and the highest vocational qualification. For the analyses, this information was combined to construct dummy variables according to the International Standard Classification of Education (ISCED) (Bohlinger 2012; Eurostat 2022), which were divided into three levels (1 = low, 2 = medium, 3 = high). Because there were only three observations in the level 3 category at T2, we combined levels 2 and 3 for the analyses. The duration of unemployment was calculated as a continuous variable for years of unemployment. No dummy variable was constructed due to the lack of variance (only 11 [12%] participants were unemployed less than 12 months).
The outcome measure (1) “self-esteem” was measured using a German version of the Rosenberg self-esteem scale (Collani and Herzberg 2003), and the outcome (2) “generalized self-efficacy expectations” was assessed by a scale from Collani and Schyns (2014). Both scales contain 10 Likert-type items scored from 1 = “strongly agree” to 5 = “strongly disagree,” resulting in a possible range from 10 to 50 points (the higher the value, the greater the self-esteem or the generalized self-efficacy expectations, respectively). The participants’ self-evaluation of (3) their general health status was done via a Likert-type item asking “How is your health in general?” scored from 1 = “very bad” to 5 = “very good” (the higher the value, the better the self-rated general health status) (EHEMU 2010). Additionally, we examined (4) the level of unemployment-related mental burden using the unemployment-related mental burden scale from Trube and Luschei (2000). The scale contains 10 Likert-type items scored from 1 = “at no time” to 4 = “very often,” resulting in a possible range of points from 10 to 40 (the higher the value, the greater the unemployment-related mental burden). The data were analyzed exclusively by the research team of the University of Kassel.
Statistical analyses
All analyses were conducted with the SPSS version 28.0 statistical software package. We treated Likert-type items as continuous variables. For scales, based on multiple items including those for self-esteem, generalized self-efficacy expectations, and unemployment-related mental burden, we calculated additive scores according to the respective scale documentation.
We carried out standard descriptive analyses and—depending on the data measurement level, number of categories, distribution, and cell counts—conducted chi-square tests or Fisher–Freeman–Halton exact tests for categorical variables and nonparametric Mann–Whitney U-tests or t-tests in order to conduct group comparisons of continuous variables. This was done (1) to describe the sample, (2) to examine how far the randomization worked out, (3) to conduct a dropout analysis, and (4) to identify significant group differences between the two groups at T0 and T2, particularly in terms of the focused outcome variables. We additionally aimed at identifying significant changes in the outcomes from T0 to T2 within the IVG and the WCG using t-tests or Wilcoxon tests for paired samples. To identify multicollinearity, we created a correlation matrix for all variables studied. According to Field (2018), a strong correlation was assumed, with a Spearman rank correlation coefficient (rs) above 0.8.
In multivariate analyses, we used ordinary least squares (OLS) linear regression models adjusted for baseline values of the respective outcomes. We conducted sequential linear regression models that build upon each other. According to Urban and Mayerl (2018), sequential regression analysis has the advantage that it can control for the dependence of the estimate of individual predictor effects on the estimated effects of other predictors in the model. In addition, the sequential procedure can easily identify both stable and unstable predictor effects, as well as those predictors that have a strong influence on the estimate for other predictor effects. In this way, it is also possible to investigate how strongly individual estimated predictor effects are influenced by the inclusion or exclusion of other predictors in the model. By using sequential regression, the different models can be compared in terms of the increase in the coefficient of determination of the regression, and this increase can additionally be tested for statistical significance using an F-test (see last row in Tables 4 and 5). The F-test assesses the increase in the coefficient of determination that is achieved by adding additional predictor variables in an extended model. Thus, it can be observed whether the model fit is meaningfully improved via the inclusion of additional predictor variables in the regression model and whether the addition of those predictors is thus statistically reasonable (Urban and Mayerl 2018).
Model 1 (M1) included (1) the treatment indicator variable contrasting the IVG and the WCG in terms of the effect on the outcome and (2) the variable representing the baseline values of the respective outcome. The latter was performed because it is expected that the baseline (T0) value of the focused outcome has a relevant effect on the dependent outcome variable (at T2). This is especially true if the comparison groups (IVG vs. WCG) differ with respect to the baseline value. For this reason, it is recommended that baseline outcome values be included as a predictor in pre/post randomized controlled trials comparing the efficacy of two competing treatments (here, JOBS training vs. no intervention) (Wan 2021; van Breukelen 2006). Given the relevance of the baseline value of the outcome, it would not be meaningful to include only the treatment indicator variable in model 1. In model 2 (M2), demographic variables and variables representing the duration of unemployment and the level of depressive symptoms were additionally included. Those independent predictors were selected (1) on a theoretical basis or (2) if they were shown to be statistically associated at a significance level ≤ 0.2 with the outcome variable in different bi- and multivariate pretests. In the third model (M3), we further included interaction terms between our treatment indicator and the respective moderators to examine the abovementioned effect moderation (duration of unemployment, level of depressive symptoms at T0).
With the exception of the correlation analyses, where pairwise analyses were performed (Table 2), all analyses were performed as list-wise deletion (complete-case) analyses and according to the intention-to-treat principle (treating participants as if they belonged to the group to which they were originally [randomly] assigned, regardless of what treatment [if any] they received [in this case the JOBS training] (McCoy 2017)). A p-value of less than or equal to 0.05 was considered statistically significant.
Following the arguments of Ludbrook (2013), we used one-sided or two-sided p-values to evaluate our results depending on the a priori stipulated scientific hypotheses (H0) and on the alternative statistical hypotheses (H1). Since we hypothesized that the intervention would have only positive effects on the outcomes studied (H1; unidirectional), we applied one-sided significance tests (1) for the bivariate correlations between the intervention variable and the levels of the outcomes at T2 (Table 2), (2) for the IVG vs. WCG outcome comparisons at T2, and (3) for the tests whether the IVG improved from T0 to T2 (both Table 3) as well as (4) for the treatment effects analyses in the multivariate linear regression models (Tables 4 and 5). All other p-values reported are two-sided.
Results
Participant recruitment
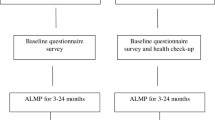
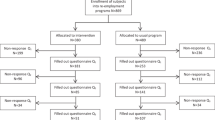
Between March and December 2022, seven JOBS training sessions were implemented, and 137 individuals signed the consent form and provided their contact data. Ninety-four participants completed the CATI at T0 and 43 at T2 (response rates 68.6 and 31.4%) (Fig. 1).

Flow chart of participant recruitment
Randomization and dropout analysis
To determine whether the statistical analyses were indeed performed according to a randomized controlled design, we compared the demographic and outcome variables for statistically significant differences between the IVG and WCG at T0 (Tables 1 and 3). There were only a few differences in demographic variables between the two groups at T0. The proportion of men was 8% greater in the IVG than in the WCG (58 vs. 50%), and the depressive symptoms score was about 14% higher in the IVG, indicating better mental health in the IVG at T0. There were also no relevant or significant differences at T0 among the outcome variables considered. For all variables reported here, we found no statistically significant differences between the two groups at T0, confirming the integrity of randomization.
The response rate of approximately 31.4% at T2 prompted us to examine whether there were statistically significant differences between those responding at T2 and those not responding (“dropouts”) with regard to (1) their demographic characteristics and (2) the levels of the outcome variables at T0. The results of the bivariate analyses on the demographic variables did not show large differences between the two groups. The proportion of men was greater among the dropouts than among the respondents (61.7 vs. 44.2%). In comparison with the responders, the group of dropouts were slightly older (1.4 years), had a lower level of education (proportion of those with high/medium educational level: 55.3 vs. 67.4%), were more often married/living in partnership (23.4 vs. 16.3% singles), and were unemployed for a shorter period of time (5.35 vs. 7.77 years). However, statistically, no differences were detectable with regard to these demographic variables. The dropouts versus responder comparisons concerning the T0 outcome levels showed only very small differences for all four outcomes, and none even came close to statistical significance. We found the largest difference for the general health status. Among dropouts, 40.4% reported “good” or “very good” general health, compared with 37.2% of responders. As the small group differences suggest for the outcomes, none of the group comparisons were statistically significant, indicating that there was no systematic bias in the results due to dropouts.
Participant characteristics
The mean age of the participants (T0, N = 94) was 44.7 years (standard deviation [SD] = 11.8). Slightly more than half of the participants were men (n = 51; 54.3%) and single (n = 52; 55.3%). Thirty-six (38.3%) individuals had a low, 50 (53.2%) a medium, and 8 (8.5%) a high level of education. The vast majority (n = 83; 88.3%) had German citizenship, and the mean duration of unemployment was 6.4 years (SD = 6.1; median = 4.03). One participant had just become unemployed, and the longest reported duration of unemployment was 26 years.
Bivariate correlation analysis
Table 2 shows the correlations between all variables studied. Regarding their directions of correlation, the treatment indicator variable has plausible correlation coefficients with the four outcome variables at T2. They correspond to the alternative statistical hypotheses defined a priori (H1), namely that the intervention would have positive effects on the outcomes. The range is from rs = −0.14 (reduction in unemployment-related mental burden [weak correlation, not statistically significant]) to rs = 0.31 (improvement of general health [weak/fair correlation, p = 0.023]). For all four outcome variables, statistically significant and plausible associations were identified between their T0 and T2 values, with moderate to strong positive correlation coefficients ranging from rs = 0.5 to 0.72.
It is worth mentioning the various moderate to strong correlations between personal resources (self-esteem and generalized self-efficacy expectations) and the mental health outcomes (depressive symptoms and unemployment-related mental burden), with the strongest coefficient for the negative significant correlation between unemployment-related mental burden at T0 and self-esteem at T0 (rs = 0.66). Among the predictor variables, the strongest significant correlation was found between the duration of unemployment and participant’s gender (rs = 0.53). Since the analyzed predictor variables did not show strong correlations with each other, there was no evidence of multicollinearity in the bivariate correlation analysis
IVG versus WCG differences at T0 and T2 and outcome changes from T0 to T2 in both groups
Table 3 shows the values for the outcomes in the IVG and the WCG for both survey time points T0 and T2 with the associated significance tests for differences between the groups at both time points. It also shows the extent to which the outcomes changed from T0 to T2 within each group, with the respective significance tests.
Concerning the personal resource-related outcomes, that is, the participants’ self-esteem and generalized self-efficacy expectations, there were no significant group differences at either T0 or T2. On the other hand, a significant increase was clear for both outcomes in the IVG. As expected, the slight changes from T0 to T2 in the WCG are not statistically significant. The results on health-related outcomes show a different picture. The change in general health status from T0 to T2 was not statistically significant in either IVG or WCG. However, the IVG had a significantly better general health status at T2 than the WCG, while the T0 levels were similar between groups, and the small difference between the groups was not significant. Looking at unemployment-related mental burden, at first glance we see a counterintuitive trend between T0 and T2, with a small increase in the IVG and a slight decrease in the WCG. However, these marginal differences between the IVG and the WCG at both time points and the minimal outcome changes between T0 and T2 for both groups are reflected in p-values that are far from statistical significance.
Intervention effect on personal resources and health-related outcomes
In further analyses, multivariate linear regression was applied to examine whether the treatment indicator variable was associated with the outcome variables. Tables 4 and 5 report multivariate unstandardized regression coefficients, the coefficient of determination (R2), and the adjusted coefficient of determination (R2adj.) for the three sequential models (M1 to M3) for each of the four outcomes. Furthermore, it can be seen whether there was a significant change in F from model to model.
In these regression analyses, the most important model for the main effects of the predictors is model 2. Because it includes the relevant predictors (selected during different pre-analyses and based on theoretical considerations) but no interaction terms.
The interaction terms were added in model 3 to examine the hypothesized effect moderations (hypotheses V and VI). However, in multiplicative interaction models (such as M3), the interpretation of the regression coefficients is often difficult and does not reflect the main effect of the single predictor. Rather, when interaction terms are included in the model, there are often situations in which the regression coefficients for each predictor variable say nothing about their actual effect on the outcome, nor do their respective p-values (Brambor et al. 2006; Stoetzer 2017).
Hypothesis I: The JOBS training will increase participants’ self-esteem
On the German version of the Rosenberg self-esteem scale with a range from 10 to 50 points, the IVG at T2 had on average a 1.86-point higher score than the WCG (p = 0.136). On the other hand, Table 3 shows that the IVG also had a significant, albeit small, increase from T0 to T2 (p = 0.034), while a marginal nonsignificant increase was found in the WCG. Additionally, the multivariate regression coefficient in the third row of Table 4 shows that JOBS training had a significant positive effect on self-esteem in model 2. Compared with the WCG, the regression estimated that the IVG had a 3.479-point higher level of self-esteem (p = 0.032). The significant score change from T0 to T2 in the IVG and the significant positive regression coefficient in model 2, coupled with the plausibility of the association (JOBS training increases participants' self-esteem), strongly support hypothesis I.
Hypothesis II: The JOBS training will increase participants’ generalized self-efficacy expectations
On the generalized self-efficacy expectations scale with a range from 10 to 50 points, there was virtually no difference in the level of generalized self-efficacy expectations at T0 between IVG and WCG. At T2, however, the IVG clearly showed a higher score than the WCG (IVG: 36.87; WCG: 33.53; p = 0.088). This is also reflected by a significant increase from T0 to T2 in the IVG (+2.7 points; p = 0.002), while there was a nonsignificant decrease in the WCG (−0.54 points; p = 0.343) (Table 3).
The results displayed in the third row of Table 4 show—from model 1 to model 3—a clear, consistent, and statistically significant positive regression coefficient. Compared with the WCG, the regression in model 2 estimated that the IVG had a 4.930-point higher level of generalized self-efficacy expectations (p = 0.002). This significant increase in the IVG from T0 to T2, together with the significant estimate in model 2 and the plausibility of the association (JOBS training increases participants' generalized self-efficacy expectations), confirms hypothesis II.
Hypothesis III: The JOBS training will increase participants’ general health status
On a scale from 1 to 5 points, the difference at T0 between groups was negligible and statistically nonsignificant, with an average of 0.14 points higher in the IVG than the WCG (p = 0.611). At T2, the difference between groups was considerably larger (0.48) and significant (p = 0.024), but the changes from T0 to T2 in both groups showed no significant results (Table 3). The results of the multivariate analysis (third row of Table 5) show that the JOBS training had a clear, consistent, and statistically significant beneficial effect on the general health status. The most relevant model 2 showed that the IVG had a 0.410-point higher level of general health than the WCG (p = 0.016). The statistically significant IVG versus WCG-group difference at T2, the stable and significant regression coefficients, and the plausible direction of the effect (JOBS training increases the general health of the participants) confirm hypothesis III.
Hypothesis IV: The JOBS training will decrease the participants’ unemployment-related mental burden
On the unemployment-related mental burden scale, which ranged from 10 to 40 points, the respective levels between IVG and WCG at T0 and T2 did not differ significantly. The changes from T0 to T2 in both groups were also not significant (Table 3). In the third row of Table 5, however, the multivariate regression results show a different picture. The most relevant model 2 indicates that the JOBS training had a significant beneficial effect on the outcome. Compared to the WCG, the regression in model 2 estimated that the IVG had a 2.042-point lower level of unemployment-related mental burden (p = 0.028). Despite the weak results shown in Table 3, the significant regression coefficient in model 2 and the plausible direction of the effect (JOBS training reduces the unemployment-related mental burden) suggest a positive intervention effect supporting hypothesis IV.
Hypotheses V and VI: The level of depressive symptoms and/or the duration of unemployment, respectively, before the JOBS training will moderate the effect of the intervention on unemployment-related mental health burden
The results concerning the hypotheses that (1) the level of depressive symptoms and/or (2) the duration of unemployment before the JOBS training would moderate the effect of the intervention on unemployment-related mental burden do not support these hypotheses. First, the interaction terms included in model 3 have only very small regression coefficients, and second, these estimates are far from statistical significance (“Intervention × Dur_Unempl”: rs = −0.083; p = 0.656; “Intervention × Depression”: rs = 0.048; p = 0.362).
Discussion
There are already a wide variety of interventions for the unemployed to promote health and re-employment (Liu et al. 2014; Hult et al. 2020; Hollederer 2019; Paul and Hollederer 2023). One of those interventions is the JOBS Program described and evaluated herein. This program has been applied in many countries around the globe (Caplan et al. 1989; van Ryn and Vinokur 1992; Vinokur et al. 1991a; Price et al. 1992; Vuori et al. 2002; Vuori and Silvonen 2005; Shirom et al. 2008; Barry et al. 2006; Reynolds et al. 2010; Brenninkmeijer and Blonk 2012; Price and Vinokur 2014; Paver et al. 2020b; Paver et al. 2020a) but it had not—until the pilot introduction in 2020 reported here—been implemented in Germany on a larger scale. The introduction of the JOBS Program Germany as a nationwide pilot project allowed for the first systematic evaluation of this intervention in the German context.
Hypothesis I
Hypothesis I of this evaluation was that JOBS Program Germany would succeed in increasing IVG participants’ self-esteem levels. Our results shown strongly support this hypothesis, and they are consistent with previous JOBS Program evaluation studies (Paver et al. 2020b; Vinokur et al. 1995; Vuori and Silvonen 2005). Vuori and Silvonen (2005), for example, found that JOBS training had a significant beneficial impact on self-esteem even 2 years after the intervention.
Hypothesis II
Our results clearly support our hypothesis II, namely that JOBS training would increase participants' generalized self-efficacy expectations. To our knowledge, general self-efficacy has not been examined in evaluation studies of the JOBS program. Typically, such evaluation studies have focused on job search-specific self-efficacy, and some of these studies have shown positive results (Brenninkmeijer and Blonk 2012; Paver et al. 2020b; Caplan et al. 1989; Vinokur et al. 1995). Brenninkmeijer and Blonk (2012), for example, examined the same time period between the JOBS training and the second interview as we report here (about 6 months after the training). They found a statistically significant increase in job search-specific self-efficacy. Although generalized self-efficacy expectations are a broader concept than job search-specific self-efficacy, with the latter being more targeted towards unemployment, we conclude that an increase in generalized self-efficacy expectations will also have positive effects on job search activities and intensity, and—as a consequence—on future re-employment.
Hypotheses III and IV
Hypotheses III and IV referred to the positive effects of the JOBS Program on health-related outcomes, namely (1) the general health status and (2) unemployment-related mental burden, and both were confirmed (hypothesis III) or supported (hypothesis IV), respectively, by our analyses. To date, the outcome “general health” has been examined only once within a JOBS Program evaluation study (Reynolds et al. 2010), and the authors did not report either meaningful/statistically significant effects or what instrument they used. As explained above, we employed the widely used item “How is your health in general” (see above) (EHEMU 2010). Semantically, it is a very broad question that basically covers all health-related dimensions, including somatic and mental health. It is therefore plausible that the JOBS Program Germany, which is a labor market- and health-promoting intervention, has proven to have a positive effect on general health. The results of our analyses with respect to hypothesis IV, that the JOBS training would decrease the level of unemployment-related mental burden, are less strong than those of the other three outcomes. However, they are in a clear and plausible direction with all three multivariate models, consistently resulting in negative regression coefficients, and the most relevant model 2 even showed a significant estimate. This positive result is also in line with the findings of several previous JOBS Program evaluation studies showing that the JOBS training has the potential to improve the mental health of participants (Vuori et al. 2002; Vinokur et al. 2000; Vuori and Silvonen 2005; Price et al. 1992; Vinokur et al. 1995).
Hypotheses V and VI
The design of this study was oriented towards two previous studies from the United States and Finland (Vinokur et al. 2000; Vuori et al. 2002). Therefore, it also sought to examine moderating factors that were examined in those studies. We examined whether (1) the baseline level of depressive symptoms and/or (2) the duration of unemployment before the JOBS training would moderate the effect of the intervention on mental health. We therefore included in our sequential regression model 3 two additional interaction terms. In line with Vinokur et al. (2000) and Vuori et al. (2002), we did not identify moderating effects of the baseline level of depressive symptoms on the intervention effect in terms of mental health (unemployment-related mental burden). Vinokur et al. (2000) did not examine moderating effects of the duration of unemployment, and the results of Vuori et al. (2002) showed no significant moderating effect of the duration of unemployment before the training, which is also in line with our findings.
The JOBS Program intervention in Germany
While previous studies such as those in the USA or Finland have yielded positive effects, we aimed to answer the question of whether the JOBS Program would reveal similar effects for the unemployed in Germany, with its different labor markets, social security system, and labor policies. However, if comparisons are to be made, certain aspects that may influence the different study results should be taken into account: As we did not preselect a certain sample, for example, based on specific demographic characteristics, not all study conditions could be replicated, and therefore there are differences relative to the Finnish study of Vuori et al. (2002). For example, at the time of recruitment, the respondents in Vuori et al. (2002) had a median age of 36 years (mean = 37.0 years; SD = 8.6), which is clearly younger than our sample (median = 46 years; mean = 44.7 years; SD = 11.8). In addition, the gender distribution varied between the two samples. Whereas in Vuori et al. (2002), 77.8% were women and 22.2% men, these proportions were 45.6% (female) and 54.3% (male) in the German sample. Further, the Finnish sample had a median unemployment duration of 5 months (mean = 10.7, SD = 17.3), and 28% were unemployed for 12 months or longer. In our sample, the median duration of unemployment was 48.5 months (mean = 76.7; SD = 73.3), and 88% were unemployed for 12 months or longer. There were also relevant differences between our sample and the US sample of Vinokur et al. (2000). The participants in that sample were also much younger, with a median age of 34.7 years (mean = 36.2; SD = 10.38), and 45% of participants were men and 55% women. On average they had recently lost a job (mean = 4.11 weeks since job loss) and had been unemployed for no longer than 13 weeks.
In addition, the different time points for data collection after the intervention need to be considered when comparisons are made. Whereas the time points of the second survey in the Finnish study were similar to our analysis (6 months), the time point differed in the study by Vinokur et al. (2000) (2-year follow-up).
Furthermore, one needs to be aware of the different instruments used to collect data. To clarify, we can generally determine fairly well whether different studies have shown positive training effects, for example, on mental health. However, it is not easy to directly compare the reported numbers of the different studies, because we need to take into account the scale of measurement as well as the direction of the effect in addition to the “raw” numbers. For instance, Vinokur et al. (2000) noted that the training yielded a significant decrease in depressive symptoms of 0.06 points on a scale from 11 to 55 points, whereas Vuori et al. 2002 reported a nonsignificant decrease of 0.04 points on a scale from 0 to 30 points, and in our main model 2, we identified a significant decrease of 2.04 points on the unemployment-related mental burden scale, which ranges from 10 to 40 points.
Limitations
This study was originally aimed at examining the effects of the JOBS Program intervention on the reintegration into the labor market, life satisfaction, general health, and mental health outcomes among the unemployed in Germany. Of secondary interest were moderating factors such as sociodemographic characteristics, the duration of unemployment, and the job search intensity. The constraints established during the COVID-19 pandemic and its infection control measures resulted in a low number of participants, which led to low statistical power.
Conclusions
This study contributes to the existing literature on the effectiveness of the JOBS Program, for the first time in Germany. About 6 months after the training had been conducted (T2), participants in the JOBS training showed better self-esteem, higher generalized self-efficacy expectations, better general health, and decreased unemployment-related mental burden. Despite the difficulties due to the COVID-19 pandemic, particularly in terms of participant recruitment (resulting in low statistical power), our results indicate that JOBS Germany is effective.
It is known that mental health effects are stronger among the long-term than the short-term unemployed (McKee-Ryan et al. 2005), and our results suggest that the positive health effects of the JOBS Program also apply to people experiencing long-term unemployment, as 88.4% (n = 38) of the IVG were unemployed long-term (≥ 12 months) at T2. In addition, our sample was older than those in most other studies, which argues for also offering JOBS training to older unemployed people who are looking for re-employment.
The introduction of the JOBS Program as a nationwide intervention in Germany could be another way for this target group to achieve a better future with better health and increased chances for re-employment. In addition to the current concept of face-to-face teaching, blended learning concepts could be used to replace or complement the current training program. This could increase the reach and would be more feasible for certain target groups who, for personal reasons, cannot easily complete a 20-hour training course outside their home.
The results show that the training could only partially increase the self-efficacy of the participants. Among other reasons, this might be because the participants in the observation period were aware that reintegration into the labor market was made even more difficult by the COVID-19-related lockdowns. However, since self-efficacy expectations are also based on personal experience of positive coping, it could also be helpful to offer individual counseling after the training sessions. In this way, the trainers could support the participants individually in the application process beyond the training units, for example, in the preparation of contacts with employers or with regard to job interviews. Such "milestones" could be followed up and the positive aspects of these activities could be worked out—similar to the JOBS training sessions.
A focus group discussion showed that health literacy is related to help-seeking and participation in health promotion services among the unemployed (Mayer and Hollederer 2022a,2022b). Therefore, health literacy among the unemployed could contribute to maintaining their health.
The results obtained under the difficult conditions suggest that further development of the JOBS Program Germany is promising. It should also be investigated to what extent the concept of the JOBS Program can be differentiated for different subgroups of people without employment or even for groups beyond the unemployed. This is because the training is primarily based on strengthening personal resources such as self-efficacy expectations, self-esteem, and self-confidence, and therefore can certainly be extended to other groups of people, such as socially disadvantaged populations.
Data availability
The data presented in this study are not available from the corresponding author. The data used for this work were collected from volunteer participants who consented to the data collection and the corresponding data protection concept. This data protection concept includes that data will not be shared with others not involved in this research project and that data collected from subjects will be deleted 5 years after completion of data collection or no later than December 31, 2028. The data protection concept was reviewed and approved by the responsible departments in the individual institutions. All data are collected, transmitted, stored, and deleted in strict compliance with the German Federal Data Protection Act and the European General Data Protection Regulation (DS-GVO).
Code availability
Not applicable.
References
Arena AF, Mobbs S, Sanatkar S, Williams D, Collins D, Harris M, Harvey SB, Deady M (2023) Mental health and unemployment: A systematic review and meta-analysis of interventions to improve depression and anxiety outcomes. J Affect Disord 335:450–472. https://doi.org/10.1016/j.jad.2023.05.027
Barry M, Reynolds C, Sheridan A, Egenton R (2006) Implementation of the JOBS programme in Ireland. J Public Mental Health
Bandura A (1971) Social Learning Theory. General Learning Press, New York City
Bandura A (1977a) Self-efficacy: toward a unifying theory of behavioral change. Psychological review 84(2):191–215. https://doi.org/10.1037//0033-295x.84.2.191
Bandura A (1977b) Social Learning Theory. Prentice-Hall, Oxford
Bandura A (1986) Social foundations of thought and action. Englewood Cliffs, NJ 1986:23–28
Bandura A (2004) Health promotion by social cognitive means. Health Educ Behavior Off Publ Soc Public Health Educ 31(2):143–164. https://doi.org/10.1177/1090198104263660
Bohlinger S (2012) Internationale Standardklassifikation im Bildungswesen. BWB 41(4):16–19
Brambor T, Clark WR, Golder M (2006) Understanding Interaction Models: Improving Empirical Analyses. Polit Anal 14(1):63–82. https://doi.org/10.1093/pan/mpi014
Brenninkmeijer V, Blonk RWB (2012) The effectiveness of the JOBS program among the long-term unemployed: a randomized experiment in the Netherlands. Health Prom Int 27(2):220–229. https://doi.org/10.1093/heapro/dar033
BZgA, GKV-Spitzenverband (2021) Mit Selbstvertrauen in die Jobsuche – JOBS Program: Trainingsmanual zur Erprobung. Adaptierte und übersetzte Fassung des Original-Trainingmanuals „JOBS: A Manual for teaching people successful job search strategies – JOBS implementation manual“, verfasst von Joan Curran, Paula Wishart, John Gingrich und weiteren JOBS Projektmitarbeitenden des Michigan Prevention Research Center (MRPC), Institute for Social Research, Universität Michigan, Mai 1999, 1st edn., Berlin
Caplan RD, Vinokur AD, Price RH, van Ryn M (1989) Job seeking, reemployment, and mental health: a randomized field experiment in coping with job loss. J Appl Psychol 74(5):759–769. https://doi.org/10.1037/0021-9010.74.5.759
Collani GV, Herzberg PY (2003) Eine revidierte Fassung der deutschsprachigen Skala zum Selbstwertgefühl von Rosenberg. Zeitschrift für Differentielle und Diagnostische Psychologie 24(1):3–7. https://doi.org/10.1024//0170-1789.24.1.3
Collani GV, Schyns B (2014) Generalisierte Selbstwirksamkeitserwartung. Zusammenstellung sozialwissenschaftlicher Items und Skalen (ZIS). Edited by ZIS - GESIS Leibniz Institute for the Social Sciences. Available online at https://zis.gesis.org/skala/von-Collani-Schyns-Generalisierte-Selbstwirksamkeitserwartung. Accessed 13 Jan 2024
Curran J, Wishart P, Gingrich J (1999) JOBS: A manual for teaching people successful job search strategies. JOBS implementation manual. Edited by Michigan Prevention Research Center (MPRC), Institute for Social Research, University of Michigan. Ann Arbor, Michigan
EHEMU (2010) The Minimum European Health Module: EHEMU Technical report 2010_4.6
Eurostat (2022) Glossary: International standard classification of education (ISCED). Hg. v. European Union. Statistical Office of the European Union (EUROSTAT). https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Glossary:International_standard_classification_of_education_(ISCED), Accessed 24 Apr 2023
Field A (2018) Discovering statistics using IBM SPSS statistics, 5th edn. SAGE, Los Angeles
Garcy AM, Vågerö D (2012) The length of unemployment predicts mortality, differently in men and women, and by cause of death: A six year mortality follow-up of the Swedish 1992–1996 recession. Social Sci Med 74(12):1911–1920
Hollederer A (2019) Health promotion and prevention among the unemployed: a systematic review. Health Prom Int 34(6):1078–1096. https://doi.org/10.1093/heapro/day069
Hollederer A (2021) Gesundheit und Krankheit von Arbeitslosen sowie Chancen und Grenzen arbeitsmarktintegrativer Gesundheitsförderung. In: Hollederer A (ed) Gesundheitsförderung bei Arbeitslosen, 1st edn. Fachhochschulverlag, Frankfurt am Main, pp 12–35
Hollederer A, Jahn HJ, Klein D (2021) JOBS Program Germany for health promotion among the unemployed in the community setting with institutions for employment promotion (JobsProgramDtl): study protocol for a randomized controlled trial. BMC public health 21(1):261.https://doi.org/10.1186/s12889-021-10251-8
Hollederer A, Jahn HJ (2023) Results from a nationwide evaluation study of labor market-integrative health promotion for the unemployed: impact of the JOBS Program Germany. IJERPH 20(19):6835. https://doi.org/10.3390/ijerph20196835https://doi.org/10.1186/s12889-021-10251-8
Hollederer A, Frempong AH, Jahn HJ (2023) Herausforderungen bei der Förderung der Gesundheit von Arbeitslosen am Beispiel JOBS Program Deutschland. Public Health Forum 31(3):175–180. https://doi.org/10.1515/pubhef-2023-0048
Hult M, Lappalainen K, Saaranen TK, Räsänen K, Vanroelen C, Burdorf A (2020) Health-improving interventions for obtaining employment in unemployed job seekers. Cochrane Database System Rev. https://doi.org/10.1002/14651858.CD013152.pub2
Jahn HJ, Mayer D, Hollederer A (2023) Health promotion for the unemployed: the evaluation of the JOBS Program Germany from the trainers’ perspective. Archives of Public Health 81(199):1–18. https://doi.org/10.1186/s13690-023-01203-2
Kim TJ, von dem Knesebeck O (2016) Perceived job insecurity, unemployment and depressive symptoms: a systematic review and meta-analysis of prospective observational studies. Int Arch Occup Environ Health 89(4):561–573. https://doi.org/10.1007/s00420-015-1107-1
Kroll LE, Müters S, Lampert T (2016) Unemployment and Health: An overview of current research results and data from the 2010 and 2012 German Health Update. Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz 59(2):228–237. https://doi.org/10.1007/s00103-015-2282-7
Lamberg T, Virtanen P, Vahtera J, Luukkaala T, Koskenvuo M (2010) Unemployment, depressiveness and disability retirement: a follow-up study of the Finnish HeSSup population sample. Social Psychiat Psychiatric Epidemiol 45(2):259–264. https://doi.org/10.1007/s00127-009-0063-z
Lampert T, Kuntz B, Hoebel J, Müters S, Kroll LE (2018) Kap. 8.2 Gesundheitliche Ungleichheit. In: Bundeszentrale für politische Bildung (bpb), Statistisches Bundesamt (Destatis), Wissenschaftszentrum Berlin für Sozialforschung (WZB) in Zusammenarbeit mit Das Sozio-oekonomische Panel (SOEP) des Deutschen Instituts für Wirtschaftsforschung (DIW) (eds) Datenreport 2018: Ein Sozialbericht für die Bundesrepublik Deutschland, Bonn, pp 302–313
Liu S, Huang JL, Wang M (2014) Effectiveness of job search interventions: A meta-analytic review. Psychol Bull 140(4):1009–1041. https://doi.org/10.1037/a0035923
Ludbrook J (2013) Should we use one-sided or two-sided P values in tests of significance? Clin Exp Pharmacol Physiol 40(6):357–361. https://doi.org/10.1111/1440-1681.12086
Mayer D, Hollederer A (2022a) Health literacy of the unemployed – How can health literacy contribute in coping with unemployment? [Gesundheitskompetenzen bei Erwerbslosen – Wie kann Gesundheitskompetenz zur Bewältigung von Erwerbslosigkeit beitragen?]: in German. Public Health Forum 30(2):91–94.https://doi.org/10.1515/pubhef-2022-0035
Mayer D, Hollederer A (2022b) What helps the unemployed to stay healthy? A qualitative study of coping with the negative effects of job loss. Journal of public health research 11(2492)
McCoy CE (2017) Understanding the Intention-to-treat Principle in Randomized Controlled Trials. Western J Emerg Med 18(6):1075–1078. https://doi.org/10.5811/westjem.2017.8.35985
McKee-Ryan F, Song Z, Wanberg CR, Kinicki AJ (2005) Psychological and physical well-being during unemployment: a meta-analytic study. J Appl Psychol 90(1):53–76. https://doi.org/10.1037/0021-9010.90.1.53
Milner A, Page A, Lamontagne AD (2014) Cause and effect in studies on unemployment, mental health and suicide: a meta-analytic and conceptual review. Psychol Med 44(5):909
Paul K-I, Hollederer A (2023) The Effectiveness of Health-Oriented Interventions and Health Promotion for Unemployed People – a Meta-Analysis. Int J Environ Res Public Health 20:6028. https://doi.org/10.3390/ijerph20116028
Paul KI, Moser K (2009) Unemployment impairs mental health: Meta-analyses. J Vocational Behavior 74(3):264–282. https://doi.org/10.1016/j.jvb.2009.01.001
Paver R, de Witte H, Rothmann S, van den Broeck A, Blonk R (2020a) A systematic literature review of the implementation and evaluation of the JOBS programme: A suggested framework for South Africa. South African J Econ Manag Sci 23(1):1–13. https://doi.org/10.4102/sajems.v23i1.3049
Paver R, de Witte H, Rothmann S, van den Broeck A, Blonk RWB (2020b) The implementation and evaluation of the South African adaptation of the JOBS program. Front Psychol 11. https://doi.org/10.3389/fpsyg.2020.01418
Price RH, van Ryn M, Vinokur AD (1992) Impact of a preventive job search intervention on the likelihood of depression among the unemployed. J Health Soc Behav 33:158–167. https://doi.org/10.2307/2137253
Price RH, Vinokur AD (2014) The JOBS program: impact on job seeker motivation reemployment, and mental health. In Oxford handbook of job loss and job search, pp 575–590. https://doi.org/10.1093/oxfordhb/9780199764921.013.006
Reynolds C, Barry MM, Nic Gabhainn S (2010) Evaluating the impact of the winning new jobs programme on the re-employment and mental health of a mixed profile of unemployed people. Int J Mental Health Prom 12(2):32–41
Roelfs DJ, Shor E, Davidson KW, Schwartz JE (2011) Losing life and livelihood: a systematic review and meta-analysis of unemployment and all-cause mortality. Social Sci Med 72(6):840–854
Shirom A, Vinokur A, Price RH (2008) Self-Efficacy as a Moderator of the Effects of Job-Search Workshops on Re-Employment: A Field Experiment1. J Appl Social Psychol 38(7):1778–1804. https://doi.org/10.1111/j.1559-1816.2008.00369.x
Stoetzer M-W (2017) Regressionsanalyse in der empirischen Wirtschafts- und Sozialforschung Band 1. Springer, Berlin Heidelberg
Trube A, Luschei F (2000) Entwicklungs- und Vermittlungs-Assistenz (EVA) - Ein Instrument zur Wiedereingliederung Langzeitarbeitsloser. Abschlussbericht über die Evaluation des Projekts “Entwicklungs- und Vermittlungs-Assistenz (EVA)”. Im Auftrag des Instituts für Arbeitsmarkt- und Berufsforschung (IAB), Nürnberg. Edited by Universität – Gesamthochschule Siegen, Zentrum für Planung und Evaluation Sozialer Dienste (ZPE). Siegen (ZPE-Schriftenreihe, 7). Available online at http://www.luschei.de/images/projekte_forschung/eva/Trube_Luschei_2000_-_Abschlussbericht_ueber_die_Evaluation.pdf. Accessed 13 Jan 2024
Urban D, Mayerl J (2018) Angewandte Regressionsanalyse: Theorie, Technik und Praxis. Wiesbaden: Springer VS (Studienskripten zur Soziologie). Available online at https://link.springer.com/book/10.1007/978-3-658-01915-0. Accessed 13 Jan 2024
van Breukelen GJP (2006) ANCOVA versus change from baseline: more power in randomized studies, more bias in nonrandomized studies corrected. J Clin Epidemiol 59(9):920–925. https://doi.org/10.1016/j.jclinepi.2006.02.007
van Ryn M, Vinokur AD (1992) How did it work? An examination of the mechanisms through which an intervention for the unemployed promoted job-search behavior. Am J Commun Psychol 20(5):577–597
Vinokur AD, Price RH, Caplan RD (1991a) From field experiments to program implementation: Assessing the potential outcomes of an experimental intervention program for unemployed persons. Am J Commun Psychol 19(4):543–562
Vinokur AD, van Ryn M, Gramlich EM, Price RH (1991b) Long-term follow-up and benefit-cost analysis of the Jobs Program: A preventive intervention for the unemployed. J Appl Psychol 76(2):213–219. https://doi.org/10.1037/0021-9010.76.2.213
Vinokur AD, Price RH, Schul Y (1995) Impact of the JOBS Intervention on Unemployed Workers Varying in Risk for Depression. Am J Commun Psychol 23(1):39–74. https://doi.org/10.1007/BF02506922
Vinokur AD, Schul Y, Vuori J, Price RH (2000) Two years after a job loss: Long-term impact of the JOBS program on reemployment and mental health. J Occup Health Psychol 5(1):32–47. https://doi.org/10.1037/1076-8998.5.1.32
Vuori J, Silvonen J (2005) The benefits of a preventive job search program on re-employment and mental health at 2-year follow-up. J Occup Organiz Psychol 78(1):43–52. https://doi.org/10.1348/096317904X23790
Vuori J, Silvonen J, Vinokur AD, Price RH (2002) The Työhön Job Search Program in Finland: Benefits for the unemployed with risk of depression or discouragement. J Occup Health Psychol 7(1):5–19. https://doi.org/10.1037//1076-8998.7.1.5
Wan F (2021) Statistical analysis of two arm randomized pre-post designs with one post-treatment measurement. BMC Med Res Methodol 21(1):1–16. https://doi.org/10.1186/s12874-021-01323-9
Acknowledgements
We thank all unemployed people for their participation in this survey. We thank the German Federal Centre for Health Education (BZgA), the National Association of Statutory Health Insurance Funds (GKV-Spitzenverband), and Prof. Dr. Jukka Vuori (Finnish Institute of Occupational Health) for their good cooperation.
Funding
Open Access funding enabled and organized by Projekt DEAL. This research was funded by the German Federal Ministry of Education and Research, grant number BMBF/DLR FKZ: 01EL2001.
Author information
Authors and Affiliations
Contributions
Conceptualization, AH and HJJ; Data curation, HJJ; Formal analysis, HJJ; Funding acquisition, AH; Investigation, AH and HJJ; Methodology, AH and HJJ; Project administration, AH and HJJ; Supervision, AH; Writing—original draft, HJJ and AH; Writing—review & editing, HJJ and AH. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval
The study (grant number BMBF/DLRFKZ: 01EL2001) was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the University of Kassel on June 3, 2020. The committee assessed the planned project as ethically unobjectionable. The registration in the German Clinical Trials Register (DRKS) took place on 20.07.2020 (DRKS-ID: DRKS00022388).
Consent to participate
Written informed consent was obtained from all subjects involved in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare no conflict of interest. The funders had no role in the design of the study; the collection, analysis, or interpretation of data; the writing of the manuscript; or the decision to publish the results.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jahn, H.J., Hollederer, A. The health benefits of the JOBS Program Germany for unemployed people: A 6-month follow-up study. J Public Health (Berl.) (2024). https://doi.org/10.1007/s10389-023-02155-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10389-023-02155-1