
Summary
Background
Over the past year, there has been a significant increase in rapid antigen test (RAT) detection of SARS-CoV‑2 COVID-19. Antigen detection is usually inferior to real-time reverse transcription polymerase chain reaction (RT-PCR) in terms of sensitivity and specificity. The aim of this study was to evaluate a RAT for specificity and sensitivity in an asymptomatic collective.
Methods
The study was carried out in January 2021 at a hospital located in a district with a 7-day index and an average of more than 100 cases per 100,000 inhabitants. COVID-19 patients are treated at this hospital. All employees with symptoms typical of COVID-19 were not allowed to go to work. We used RAT by Roche® (Roche Diagnostics GmbH, D-68305 Mannheim) and RT-PCR on our employees. The testing was done voluntarily. We performed RT-PCR and RAT using two swab tubes at the same time.
Results
We could correlate 919 RAT to 919 RT-PCR tests. 12 people tested positive in RAT. All 12 tests were validated by RT-PCR. There was not one incorrect positive result in RAT. In one person COVID-19 was not detected by RAT, but then positively identified with a RT-PCR. In the group of positive RAT, the mean cycle threshold (CT) value was 19.95. Our results showed a sensitivity of 92.3%, CI (confidence interval) [0.78; 1.00] and a specificity of 100.00% CI [1.0; 1.0].
Conclusion
RAT can be an important tool for screening for SARS-CoV‑2 COVID-19 at the point of care. With low cost and resource needs, high specificity, and high specificity, RAT are performed best during the early stages of SARS-CoV‑2 COVID-19, when the viral loads are high.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
The coronavirus disease 2019 (COVID-19) pandemic, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), emerged in China in late 2019 from a zoonotic source [1]. According to the John Hopkins University, on May 2, 2021, over 152,303,832 global cases and more than 3,194,837 global deaths were recorded. The ongoing SARS-CoV‑2 pandemic challenged public health systems worldwide [2,3,4].
The gold standard for SARS-CoV‑2 detection is based on real-time reverse transcription polymerase chain reaction (RT-PCR) [2]. The RT-PCR has high sensitivity and specificity [2] but requires at least 4 h [5]. Also, RT-PCR is a laboratory-based procedure that requires equipment and trained personnel, as well as logistics for sample shipment and results communication [5]. There was an increase in the demand for RT-PCR diagnostics worldwide [2]. This led to supply bottlenecks and a significant delay in the test results [6]. Therefore, rapid and accurate tests for SARS-CoV‑2 screening are essential to expedite disease prevention and control, as well as screening [5, 7]. According to Chaimayo et al., lateral flow immunoassays using monoclonal anti-SARS-CoV‑2 antibodies, which target SARS-CoV‑2 antigens, can be complementary screening tests if their accuracy is comparable to that of the RT-PCR assays [5]. These rapid antigen tests (RAT) are usually inferior in terms of sensitivity and specificity to RT-PCR [8, 9].
According to the study by Toptan et al., it is vital to determine the sensitivity and specificity of such tests relative to standard RT-PCR in order to identify the ideal circumstances in which their application would be beneficial [2, 10]. The aim of this study was to evaluate the RAT by Roche® (Roche Diagnostics GmbH, D-68305 Mannheim) for specificity and sensitivity in an asymptomatic collective compared to the results of RT-PCR.
Material and methods
This study was approved by ethic committee of the Bayerischen Landesärztekammer (21002).
Clinical specimens
The study was carried out on all employees of the Krankenhaus Agatharied, Germany, during January 2021. The hospital is located in a district which had a 7-day index of more than 100 cases per 100,000 inhabitants. COVID-19 patients were treated at the hospital. All employees with symptoms typical of COVID-19 were not allowed to go to work.
Due to the national and local test strategy, we carried out RAT and RT-PCR on our employees. The testing was voluntary. We performed RT-PCR and RAT using two swab tubes at the same time.
The aim of this test strategy was to identify asymptomatic carriers of the virus.
Description of the tests
These tests were performed by trained healthcare professionals using a nasopharyngeal swab collected from each employee. The test results were determined using the four eyes principle. As RAT, we used the Roche® Rapid SARS COVID test. This test is a rapid chromatographic immunoassay for the detection of SARS-CoV‑2 nucleocapsid (N) antigen in respiratory specimens. The RAT was performed according to the manufacturer’s instructions [11]. Results were readable 15–30 min after starting.
RT-PCR was done by Eurofins. The CE-marked Eruofins ViroBOAR kit on a Roche qPCR instrument was used for analysis. Analyses were carried out in collaboration with Eurofins Genomic GmbH Ebersberg. Results were classified as negative when cycle threshold (CT) values N‑Gen > 35 and E‑Gen was not detected, or N‑Gen was not detected and E‑Gen > 33, or both N‑Gen and E‑Gen was not detected.
Statistical analysis
Descriptive statistics were used to describe the general information of the employees. We used mean, standard deviation (SD), median, and range. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and CI were calculated. A χ2-test was used to examine associations between categorical variables. Analyses were performed with SPSS 22 (IBM, Armonk, NY, USA). P-values α < 0.05 were considered statistically significant.
Results
The workforce consists of 1204 employees. The mean age of the study population was 41.5 years (range 18–66). 918 (76%) women and 286 (24%) men were employed.
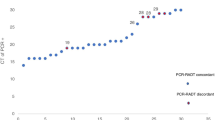
We could correlate 919 RAT to 919 RT-PCR tests (p-value 0.92). According to RAT results, 907 samples were negative and 12 were positive. All 12 positive tests were validated by RT-PCR, with a mean CT value of 19.95 (range 17.1–29.3). There was not one incorrect positive result in RAT.
In one person SARS-CoV‑2 was not detected by RAT, but then positively identified with RT-PCR. The CT value of this person was 32.
Our results showed a sensitivity of 92.3% (CI [0.78; 1.00]) and a specificity 100.00% (CI [1.0; 1.0]). The positive predictive value was 1.0 (CI [1.0; 1.0]) and the negative predictive value 0.999 (CI [0.997; 1.001]).
Discussion
Over the past year a variety of manufacturers have developed rapid tests based on SARS-CoV‑2 protein detection in respiratory samples [12]. Two different types of tests are currently available: fluorescence- or chemiluminescence-based tests, which require an evaluation device, as well as lateral flow tests for immediate visual evaluation on site [12]. We used a lateral flow test.
As far as we know, this is the largest study that investigates the effectiveness of RAT in an asymptomatic collective. We see the RAT as a suitable method as part of the screening examination for SARS-CoV‑2 COVID-19. However, RT-PCR remains the gold standard [2]. According to our results, all employees who tested positive in the RAT were confirmed in RT-PCR. However, one employee tested false negative in RAT (CT 32).
The sensitivity and specificity of the RAT for rapid detection of SARS-CoV‑2 antigen reported by the manufacturer is 97.56% (CT value 20–30), the diagnostic specificity is > 99.9% [13]. Our results showed less sensitivity (92.3%) and the same specificity (100.00%) as the manufacturer’s results.
So far, there are few data available about the performance/manageability of the available antigen tests in routine screening of asymptomatically infected or presymptomatic persons [14, 15]. Centuri described sensitivity, specificity, negative, and positive predictive values of 70.6%, 100%, 87.4%, and 100%, respectively, compared to RT-PCR [14]. However, there are also poor results reported in the literature. Compared with real-time RT-PCR testing, Prince-Guerra et al. described a sensitivity of 64.2% for specimens from symptomatic persons and 35.8% for specimens from asymptomatic persons in RAT [15]. These results differ significantly from the information provided by the producers and our results. However, we also suspect a gap in patients with high CT values. For this, however, our study is too small to be able to make an exact statement.
According to Scophyet al., the analytical performance of RAT depends on different factors including the viral load, the quality of the specimen, and how it is processed [16]. In order to have a good quality and a high level of security in the results of the tests, we recommend having them carried out by trained personnel.
RAT is able to identify infected individuals who are infectious and can potentially transmit the virus [2]. However, the incubation period of COVID-19 is up to 7 days [17,18,19,20]. During this time the CT values are very high [21], the RAT revealed a diagnostic gap. SARS-CoV‑2 viral load in the upper respiratory tract was detected at a higher level soon after the onset of symptoms [22]. Certainly, the infectivity varies from the first day after incubation to the 20th day [21, 23,24,25,26,27,28]. If the viral load is low (CT > 30), RT-PCR is superior to RAT and may prove an infection a few days earlier [23, 29,30,31,32,33,34].
In our study, the RAT CT values in median were 19.95. Previous studies reported that lower CT values are associated with higher viral culture positivity [21, 35]. Bullard et al. observed a SARS-CoV‑2 Vero cell infectivity only for RT-PCR CT < 24 and symptom onset to test < 8 days [21]. The highest sensitivity for RAT is also given for CT values between 20 and 30 [13]. Thus, a higher chance of positive antigen detection as soon as symptoms appear can be assumed.
RAT is a useful addition to the RT-PCR testing capacity when defined requirements are fulfilled. The test seems to have the potential to quickly detect the possible existence of a transfer-relevant infection during the onset of the disease, allowing (on site, point-of-care) a first (pre-)decision about the person in question [36]. However, the WHO is currently still limiting the informative value of RAT. The original quote from WHO was as follows: “with the limited data now available, WHO does not currently recommend the use of antigen-detecting rapid diagnostic tests for patient care, although research into their performance and potential diagnostic utility is highly encouraged” [37].
We therefore recommend repeating the tests regularly over several days in order to identify as early as possible all asymptomatic persons in a sensitive facility, if an RT-PCR test is not available. RAT has several advantages, such as the ease and fast achievement of the test, the rapid answer, the lower cost, and the non-requirement of special equipment [16]. Therefore, these tests can be used frequently for detecting infected individuals who are asymptomatic, presymptomatic, and without known or suspected exposure to SARS-CoV‑2 [38]. We agree with Drosten’s statement, “RAT can be beneficial in congregate settings, such as a long-term care facility or a correctional facility, workplace, or a school testing its students, faculty, and staff. RAT are likely perform best during the early stages of COVID-19, when the viral loads are higher” [2].
References
Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382:727–33.
Corman VM, Haage VC, Bleicker T, et al. Comparison of seven commercial SARS-CoV‑2 rapid point-of-care antigen tests. medRxiv. 2020; https://doi.org/10.1101/2020.11.12.20230292.
Johns Hopkins. Coronavirus resource center.. https://coronavirus.jhu.edu/map.html. Accessed 2 May 2021.
World Health Organization. Coronavirus disease (COVID-19) weekly epidemiological update and weekly operational update.. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports. Accessed 1 Sept 2020.
Chaimayo C, Kaewnaphan B, Tanlieng N, et al. Rapid SARS-CoV‑2 antigen detection assay in comparison with real-time RT-PCR assay for laboratory diagnosis of COVID-19 in Thailand. Virol J. 2020;17:177. https://doi.org/10.1186/s12985-020-01452-5.
SD Biosensor. SARS-CoV‑2 rapid antibody test package insert. 2020.
Lambert-Niclot S, Cuffel A, Le Pape S, et al. Evaluation of rapid diagnostic assay for detection of SARS-CoV‑2 antigen in nasopharyngeal swab. J Clin Microbiol. 2020;58(8):e977–20. https://doi.org/10.1128/JCM.00977-20.
Mak GC, Cheng PK, Lau SS, et al. Evaluation of rapid antigen test for detection o f SARS-CoV‑2 virus. J Clin Virol. 2020;129:104500. https://doi.org/10.1016/j.jcv.2020.104500.
Bruning AHL, Leeflang MMG, Vos J, et al. Rapid tests for influenza, respiratory syncytial virus, and other respiratory viruses: a systematic review and meta-analysis. Clin Infect Dis. 2017;65(6):1026–32.
Toptan T, Eckermann L, Pfeiffer AE, et al. Evaluation of a SARS-CoV‑2 rapid antigen test: potential to help reduce community spread? J Clin Virol. 2021;135:104713.
https://dccdn.de/www.doccheckshop.at/media/pdf/7a/ae/25/Roche_SARS-CoV-2_Antigentest_Packungsbeilage.pdf. Accessed 28 Feb 2021.
https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Vorl_Testung_nCoV.html;jsessionid=5A23876099BA59B1729E1FDA3DD20693.internet082?nn=2386228#doc13490982bodyText6. Accessed 13 Feb 2021.
https://www.nadal-test.com/en/antigen. Accessed 13 Feb 2021.
Cerutti F, Burdino E, Milia MG, et al. Urgent need of rapid tests for SARS CoV‑2 antigen detection: evaluation of the SD-Biosensor antigen test for SARS-CoV‑2. J Clin Virol. 2020;132:104654. https://doi.org/10.1016/j.jcv.2020.104654.
Prince-Guerra JL, Almendares O, Nolen LD, et al. Evaluation of Abbott BinaxNOW rapid antigen test for SARS-CoV‑2 infection at two community-based testing sites—Pima County, Arizona, November 3–17, 2020. MMWR Morb Mortal Wkly Rep. 2021;70:100–5.
Scohy A, Anantharajah A, Bodéus M, et al. Low performance of rapid antigen detection test as frontline testing for COVID-19 diagnosis. J Clin Virol. 2020;129:104455.
Lauer SA, Grantz KH, Bi Q, et al. The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med. 2020;172:577–82.
Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020;382:1199–207.
Linton NM, Kobayashi T, Yang Y, et al. Incubation period and other epidemiological characteristics of 2019 novel coronavirus infections with right truncation: a statistical analysis of publicly available case data. J Clin Med. 2020;9:538.
WHO. Report of the WHO-China joint mission on coronavirus disease 2019 (COVID-19). 2020c.
Bullard J, Dust K, Funk D, et al. Predicting infectious SARS-CoV‑2 from diagnostic samples. Clin Infect Dis. 2020; https://doi.org/10.1093/cid/ciaa638.
Zou L, Ruan F, Huang M, et al. SARS-CoV‑2 viral load in upper respiratory specimens of infected patients. N Engl J Med. 2020;382(12):1177–9.
Arons MM, Hatfield KM, Reddy SC, et al. Presymptomatic SARS-CoV‑2 infections and transmission in a skilled nursing facility. N Engl J Med. 2020;382:2081–90.
Avanzato VA, Matson MJ, Seifert SN, et al. Case study: prolonged infectious SARS-CoV‑2 shedding from an asymptomatic immunocompromised cancer patient. Cell. 2020;183(7):1901–1912.e9. https://doi.org/10.1016/j.cell.2020.10.049.
Aydillo T, Gonzalez-Reiche AS, Aslam S, et al. Shedding of viable SARS-CoV‑2 after immunosuppressive therapy for cancer. N Engl J Med. 2020;383:2586–8.
Choi B, Choudhary MC, Regan J, et al. Persistence and evolution of SARS-CoV‑2 in an immunocompromised host. N Engl J Med. 2020;383(23):2291–3. https://doi.org/10.1056/NEJMc2031364.
Covid-Investigation Team. Clinical and virologic characteristics of the first 12 patients with coronavirus disease 2019 (COVID-19) in the United States. Nat Med. 2020;26:861–8.
He X, Lau EHY, Wu P, et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med. 2020b;26:672–5.
Wolfel R, Corman VM, Guggemos W, et al. Virological assessment of hospitalized patients with COVID-2019. Nature. 2020;581:465–9.
Hurst JH, Heston SM, Chambers HN, et al. SARS-CoV‑2 infections among children in the biospecimens from respiratory virus-exposed kids (BRAVE kids) study. Clin Infect Dis. 2020;3:ciaa1693. https://doi.org/10.1093/cid/ciaa1693.
Kimball A, Hatfield KM, Arons M, et al. Asymptomatic and presymptomatic SARS-CoV‑2 infections in residents of a long-term care skilled nursing facility—King County, Washington, March 2020. MMWR Morb Mortal Wkly Rep. 2020;69:377–81.
Xiao AT, Tong YX, Gao C. Dynamic profile of RT-PCR findings from 301 COVID-19 patients in Wuhan, China: a descriptive study. J Clin Virol. 2020;127:104346.
Zheng S, Fan J, Yu F, et al. Viral load dynamics and disease severity in patients infected with SARS-CoV‑2 in Zhejiang province, China, January–March 2020: retrospective cohort study. BMJ. 2020;369:m1443.
Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395:1054–62.
La Scola B, Le Bideau M, Andreani J, et al. Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards. Eur J Clin Microbiol Infect Dis. 2020;39:1059–61.
WHO. Advice on the use of point-of-care immunodiagnostic tests for COVID-19. 2020. https://www.who.int/news-room/commentaries/detail/advice-on-the-use-of-point-of-care-immunodiagnostic-tests-for-covid-19. Accessed 29 Apr 2020.
https://www.who.int/news-room/commentaries/detail/advice-on-the-use-of-point-of-care-immunodiagnostic-tests-for-covid-19. Accessed 14 Feb 2021.
Mina MJ, Parker R, Larremore DB. Rethinking Covid-19 test sensitivity—a strategy for containment. N Engl J Med. 2020;383:e120. https://doi.org/10.1056/NEJMp2025631.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
T. von Ahnen, M. von Ahnen, U. Wirth, H.M. Schardey, and S. Herdtle declare that they have no competing interests.
Ethical standards
All procedures performed in studies involving human participants or on human tissue were in accordance with the ethical standards of the institutional and/or national research committee and with the 1975 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
von Ahnen, T., von Ahnen, M., Wirth, U. et al. Evaluation of a rapid-antigen test for COVID-19 in an asymptomatic collective. Wien Med Wochenschr 172, 70–73 (2022). https://doi.org/10.1007/s10354-021-00883-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10354-021-00883-1