
Abstract
The aim of this study was to evaluate the efficacy of mesenchymal stem cells (MSCs) in the regeneration of periodontal bone defects in animal models. A systematic review and meta-analysis were conducted following the PRISMA guidelines, and the study was recorded in PROSPERO under reference number CDR42021247462. The PICO question was: is periodontal regeneration (cementum, periodontal ligament and alveolar bone) with MSCs more effective than other techniques? Three groups were considered: Group 1: MSCs alone or mixed with regenerative materials. Group 2: only regenerative materials. Group 3: no regenerative material nor MSCs. The search was conducted using MeSH with a total of 18 articles for qualitative analysis and 5 for quantitative analysis. For the meta-analysis, a modification of the effect size algorithm was developed, which considered a comparison of means between treatments using the Student's t sample distribution. When comparing the effect size between Group 1 and Group 2, the effect size for the new cementum was 2.83 mm with an estimated confidence interval of 95% (CI 95%) between 0.48 and 5.17 mm. When considering the fit to a random-effects model, the combined variance (τ2) was 6.1573 mm, with a standard deviation (SD) of 5.6008 mm and a percentage of total heterogeneity I2 of 92.33% (p < 0.0001). For new bone, the effect size was 0.88 mm, CI 95% − 0.25 to 2.01 mm, τ2 = 1.3108 mm (SD = 1.2021 mm) and I2 = 80.46%, p = 0.0004). With regard to the new periodontal ligament, it was not possible for the meta-analysis to be performed. MSCs have a greater capacity for tissue regeneration in root cementum than in alveolar bone compared to other regenerative materials.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Periodontitis is a chronic, multifactorial, inflammatory pathology that results in the destruction of the supporting tissues of the tooth [1]. It is estimated that 50% of the European adult population presents with some form of periodontal disease, and that 750 million people worldwide suffer from severe periodontitis [2]. Periodontal regeneration consists of several methods that aid in the reconstruction or reproduction of a lost or damaged part of the supporting tissues [3,4,5]. There are many surgical techniques and regenerative materials, which include guided tissue regeneration, growth factors, bone materials, among others, and these are considered as promising solutions for the repair and regeneration of tissues in cases of periodontium, bone defects, atrophic alveolar ridge and furcation defects [6]. Regenerative medicine is a medical discipline that is based on new knowledge of mesenchymal stem cells (MSCs) and their ability to become cells of different tissues [7]. MSCs therapy has demonstrated amazing regenerative capacities in orofacial, neurological, corneal, cardiovascular, hepatic, diabetic, renal, muscular dystrophies, and autoimmune diseases [8]. MSCs are classified into two different types: embryonic and postnatal and adult [9] according to their origin or evolutionary state, and, likewise, they are classified into the following classes: totipotent, pluripotent, and multipotent [10, 11] according to their potential. In this context, MSCs show extensive proliferative potential, multipotency, tropism and immunosuppressive functions, as has been suggested by several in vitro and in vivo studies [12]. In addition to regenerating lost alveolar bone, MSCs can also induce the growth of alveolar cementum and periodontal ligament, which involves the complete regeneration of the periodontal complex [13], a process in which platelets also play a crucial role in haemostasis, immune modulation, and repair mechanisms [14].
MSCs may be isolated from different sources, which include bone marrow, blood from the umbilical cord, adipose tissue, pancreas, liver, skeletal muscle, dermis and the synovial membrane. Alternative sources exist, which include amniotic fluid and Wharton´s jelly from the umbilical cord [15]. Recent studies have indicated that there are no morphological or immunophenotypic differences between the cells obtained from these tissues [16]. In the oral cavity, MSCs can be found in the dental pulp (DPMSCs), dental follicle and gingival connective tissue, as well as other areas [17]. Bianchi et al. studied the bio-morphological reaction of human periodontal ligament fibroblasts to different types of dentinal derivates (mineralized dentine, deproteinized and demineralized dentine, and demineralized dentine), and a positive response was observed in terms of proliferation and adhesion, with stronger vinculin and integrin signal. This therefore confirms that dentinal derivates present high conductivity and inductivity properties in the regenerative processes [18].
The use of advanced therapies based on MSCs in periodontal regeneration is derived from pre-clinical investigations, as very few controlled clinical trials (CCT) have been conducted to date to evaluate their efficacy in the treatment of human periodontal lesions [19]. In recent years, a wide variety of studies have been conducted in which MSCs were used in combination with other biomaterials to obtain optimal periodontal regeneration [20,21,22,23]; however, none of these achieved optimal success, and conflicting results were reported [24,25,26,27].
To the best of the authors’ knowledge, no meta-analysis of preclinical studies on the efficacy of MSCs in periodontal regeneration has been performed to date, and therefore there is a knowledge gap that must be closed in order to lay the foundations for adequate clinical studies in the future.
Methods
Protocol and registration
A specific study protocol was designed for the search and data retrieval process, which fulfilled PRISMA guidelines [28]. The protocol was registered in PROSPERO under reference ID CDR42021247462 to minimize the risk of bias and improve the transparency, precision, and integrity.
Focused question
The review was designed to answer this PICO question: Is periodontal regeneration with MSCs more effective than other techniques? P: Articles with studies of periodontal defects in animals were evaluated; I: Intervention, periodontal regenerations performed with different MSCs, alone or in combination with other biomaterials; C: Comparison of the different results of regeneration of the support periodontal tissue with different regenerative materials; O: Observation, the amount of periodontal regeneration, histologically measured as new bone, cementum and periodontal ligament in the periodontal defect were compared.
Information sources and search strategy
The search was conducted using the Rayyan QCRI programme (Qatar Computing Research Institute (Data Analytics), Doha, Qatarcon). Following the PRISMA requirements, the MeSH terms used were: “Mesenchymal Stem Cells”, “Periodontal Attachment Loss”, “Periodontal Atrophy”, “Alveolar Bone Loss” and “Guided Tissue Regeneration, Periodontal”. For verification purposes, other keywords (pluripotent stem cells, adult stem cells, hematopoietic stem cells, bone marrow stem cells (BMSCs), mesenchymal stem cell transplantation, furcation defect, bone regeneration) were also included when searching MEDLINE through PubMed, EMBASE through OVID, the Web of Science, Scopus, Cochrane Library, Clinical Trials, the five WHO regional bibliographic databases (AIM, LILACS, IMEMR, IMSEAR, WPRIM), and the Conference Proceedings Citation Index. Any potentially relevant articles that any of the authors were aware of, as well as reference lists from the retrieved articles, were also comprehensively checked. This process was complemented by a manual search (peer-reviewed journals with related content).
Eligibility criteria
All of the references identified from computerized databases were manually retrieved, and the articles were included if they met the following inclusion criteria: (1) Studies on bone defect regeneration with MSCs (type/origin) in animals without systemic conditions or genetic modification. (2) Studies in dogs, rabbit, rats, and pigs (the gender and age of the animals were not considered in the studies). (3) Studies of preclinical controlled animal models, in which MSCs were used locally to correct periodontal defects in the first six months with a single evaluation at 2—4—6—8 weeks. (4) Data on periodontal regeneration (cementum, bone and periodontal ligament). (5) Studies published in the English language. The following exclusion criteria were considered: (1) Human studies. (2) Alveolar bone regeneration only with biomaterials. (3) Studies that did not include a control group, or studies in which it was not possible to compare the regeneration results due to the absence of data regarding gain/loss of periodontal regeneration. (4) Clinical cases. (5) Studies for which there was a lack of measurements and standard deviation data. (6) Reviews, systematic reviews and meta-analysis.
Study selection and data extraction process
Data was retrieved by two researchers (LC and MPS) using a custom-made extraction sheet. Any discrepancies that arose between the two researchers were resolved by a third researcher (BVR) who was blinded to the study hypothesis. The following data was recorded: first author, country, type of study, type of animal, number of animals, overall number of defects, type of control condition (including group with other types of regenerative materials), number of defects in the control group, type of MSCs, number of defects in the MSCs group, and periodontal regeneration assessment procedure.
First the title and abstracts of all potential records were read, and a full-text protocol was used to determine the inclusion of any texts with insufficient data. Subsequently, all eligible articles were examined in full text, and if any data considered essential for the review was missing or unclear, an attempt was made to contact the corresponding author of the study in order to resolve or clarify the problem.
Evaluation of quality and risk of bias
The risk of bias was assessed according to the Systematic Review Centre for Laboratory Animal Experimentation (SYRCLE) [29]. An overall bias risk assessment was conducted for each study included, assigning the following bias ratings: High, Unclear, and Low. The following elements were evaluated for bias: selection, performance, detection, desertion, notification, among others. These elements were assessed using the Cochrane RoB tool. SYRCLE's risk of bias tool for animal studies includes the following aspects: (1) Sequence generation: this was evaluated taking into account whether or not periodontal defects were induced. (2) Allocation concealment: randomization results were checked by evaluating the baseline characteristics in test and control groups. (3) Incomplete result data: the inclusion of all data was verified, including the types of animals (beagle dogs, rats, mini pigs, rabbits), the number of animals, the types of periodontal defects (periodontal bone defects, furcation defects type II and III), types of MSCs, control group or groups with other materials, and assessment of periodontal regeneration (periodontal ligament, root cementum and alveolar bone). (4) Selective reporting of results: the study protocols and group results were evaluated with other materials and other sources of bias [Table 1]. (5) Selective reporting of results: The MSC groups were compared with their respective control groups, to determine whether or not there was an increased number of animals in the MSC groups or the regenerative materials group, whether or not the animals had been given additional medications, the number of surgical interventions performed, and whether or not the animals in each study received the same treatment and care, or if differentiations were made taking into account the different types of animal (beagle dogs, mini pigs, rats and rabbits) and the types of periodontal defects.
Statistical analysis
Qualitative analysis
The qualitative analysis described the general aspects of the articles that met the inclusion criteria. A systematic review of the included articles was carried out, describing the previously defined characteristics (see data extraction), and distinguishing between the three study groups: (1) the first group of MSCs alone or mixed with other types of regenerative materials. (2) the second group of other regenerative materials. (3) the third group in which no regenerative material was placed. The periodontal regeneration (alveolar bone, periodontal ligament, and alveolar cementum) was assessed in each group.
Meta-analysis
Meta-analysis was used under the following systematic process: (1) Definition of experimental variables. (2) Identification of treatment and control. (3) Determining the effect size and its standard deviation. (4) Specification of the model according to the type of characteristics: qualitative or quantitative. (5) Selection of the fixed or random effects model. 6) Model validation and heterogeneity analysis. (7) Graphical representations (Forest Plot and Funnel Plot). (8) Interpretation of the results. This process was validated through the following assumptions: (1) Tissue regeneration variable measured in mm and (2) Modification of the effect size algorithm, considering a comparison of means between treatments with Student's t sample distribution.
With respect to the method used for the meta-analysis, the effect size was determined for each of the five included studies. A high variability was obtained given that in the process of calculating the effect size, the control was not used, and in contrast, comparison between Groups 1 and 2 was made. This methodological change was justified due to the extent to which the articles reviewed did not contain adequate analysis of the control treatment, and due to the lack of extensive literature available in order to guarantee the probabilistic properties of the sampling distribution of the statistic effect size. This was adjusted for both the New Cementum and the New Bone. The calculation process was carried out through the R software, using the following statistical packages: "meta" and "metasens" [30].
Results
Biographical research
111 articles were identified through the aforementioned search, the abstracts of which were reviewed for content relevant to the topic under study, with 93 of the articles excluded for this reason. After the critical analysis of the studies had been performed, 18 studies from different geographical areas met the inclusion criteria. These 18 articles were included for qualitative analysis, and 5 of said articles were included for meta-analysis (Fig. 1).

Flowchart of selected studies
Risk of bias
The articles were evaluated using the SYRCLE RoB tool for animal studies [29]. It was determined that all of the studies had a low risk of bias [31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48], in terms of sequence generation, allocation concealment, incomplete outcome data and their sources of bias. The complete data can be found in Table 1.
Qualitative analysis: Clinical features and periodontal regeneration
The first group of MSCs alone or mixed with other types of regenerative materials included several materials, such as polyglycolic acid, bone bovine, gelatin sponge, apatite-coated silk, autogenous cortical bone, platelet-rich plasma, polyglycolic acid/trimethylene carbonate, beta-tricalcium phosphate, hydroxyapatite, and biomimetic intrafibrillarly mineralized collagen. The MSCs were obtained from the dental pulp, periodontal ligament, gingival margin and bone marrow, periosteal alveolar cells. The second group of other regenerative materials was comprised of several products: bovine bone, adenovirus, beta-tricalcium phosphate, platelet rich plasma (PRP), polyglycolic acid/trimethylene carbonate, polyglycolic acid and osteoprotegerin. Periodontal regeneration was based on the results obtained by the gain of alveolar bone, periodontal ligament and alveolar cementum tissue and the results are included in full in Table 2.
In the qualitative analysis, 18 articles were considered, some of which contained results expressed in percentages, millimetres and square millimetres. 67% of the studies were performed on Beagle dogs, 22% on rats and 11% on mini pigs. In the study groups, the most relevant stem cells were those obtained from the periodontal ligament (PDLMSC) and bone marrow stem cells (BM-MSC) mixed with bovine bone or platelet-rich plasma. In terms of bone defects, the most widely used stem cell type was PDLMSC with bovine bone and in furcation defects, type II and III, BM-MSC with platelet-rich plasma were used. A full summary of the results of the included studies is included in Table 2.
Meta-analysis
New cementum
The results obtained regarding the regeneration of root cementum when comparing the effect size between Group 1–Group 2, with Group 1 being stem cells and Group 2 other regenerative materials, shows that Group 1 presented greater regeneration of periodontal tissue than Group 2. Indeed, the initial results showed that among the studies reviewed, the effect size had an average of 3.4005 mm of tissue with a standard deviation of 1.2634. This means that the average effect size explicitly expresses the highest value by Group 1 compared to Group 2 with characteristics of experimental homogeneity in each of the experiments due to the coefficient of variation not greater than one, | cv |< 1.
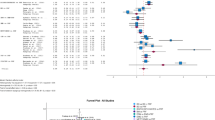
Considering the fit to a random-effects model, the combined variance, \({\tau }^{2}\) was 6.1573 with a percentage of total heterogeneity \({I}^{2}\) between studies of 92.33% (Fig. 2). At a significance level of 0.05 there was no statistical evidence to confirm that the effect between treatments is equal. There was high variability between the results obtained when comparing both treatments Q = 52.1251 (p < 0.0001), meaning therefore that there was great influence by at least one experimentation (stem cells). The Funnel plot, the influence graph and the forest plot show the significant differences between the experiments, differences that are attributed to the study by Zhou et al. 2012 [40] that has a share of the study of 13.63%, and an estimated average effect size at a confidence level of 0.95 (95%) of between 5.74 and 13.92 (Fig. 3).

Forest plot and data from the meta-analysis for the regeneration in new cementum. \({\tau }^{2}\) (estimated amount of total heterogeneity): 6.1573 (SE = 5.6008). \(\tau\) (square root of estimated \({\tau }^{2}\) value): 2.4814. \({I}^{2}\) (total heterogeneity / total variability): 92.33%. \({H}^{2}\) (total variability/sampling variability): 13.03. Test for Heterogeneity: Q (df = 4) = 52.1251, p-value < 0.0001

Funnel plot for the regeneration in new cementum
New bone
According to the results obtained when comparing the regeneration of the alveolar bone, the effect size between Group 1 and Group 2, with Group 1 being stem cells and Group 2 other regenerative materials, it was evident that Group 1 presented greater regeneration of periodontal tissue than Group 2. Indeed, the results showed that among the reviewed studies the effect size had an average of 1.2717 mm of tissue, with a standard deviation of 0.3806. This therefore means that the average effect size explicitly expresses the highest value by Group 1 compared to Group 2, with characteristics of experimental homogeneity in each of the experiments resulting from a coefficient of variation, not greater than one, | cv |< 1.
After calculating the effect size in each of the 5 studies, a high variability was determined in each of the experiments (Group with stem cells and group with other materials), an average of 1.2717 ± 0.3806 mm with characteristics of experimental homogeneity in each of the experiments due to a coefficient of variation not greater than one, | cv |< 1. Considering the fit to a random effects model, the combined variance \({\tau }^{2}\) was 1.3108, with a percentage of total heterogeneity \({I}^{2}\) between studies of 80.46% (Fig. 4). At a significance level of 0.05 there was no statistical evidence to suggest that the effect between treatments is equal. Therefore, there was a high variability between the results obtained when comparing both treatments. Q = 20.4717 (p < 0.0004). The Funnel plot, the influence plot and the forest plot show that there were significant differences between the experiments, and these differences were attributed to the study by Zhou et al. 2012 [40] that has a share of the study of 16.16% and an estimated average effect size at a confidence level of 0.95 (95%) of between 1.48 and 4.89 (Fig. 5).

Forest plot and data from the meta-analysis for the regeneration in alveolar bone. \({\tau }^{2}\) (estimated amount of total heterogeneity): 1.3108 (SE = 1.2021). \(\tau\) (square root of estimated \({\tau }^{2}\) value): 1.1449. \({I}^{2}\) (total heterogeneity / total variability): 80.46%. H2 (total variability/sampling variability) : 5.12%. Test for Heterogeneity: Q (df = 4) = 20.4717, p-value: 0.0004

Funnel plot for the regeneration in alveolar bone
New periodontal ligament
It was not possible to develop the meta-analysis due to the lack of data.
Discussion
The present systematic review and meta-analysis observed that periodontal regeneration with MSCs alone or mixed with other regenerative materials, such as beta-tricalcium phosphate, bovine bone or platelet-rich plasma, offered better regenerative results than those attained for the group with only regenerative materials. Qualitative studies showed that PDLSc and BMSCs appear to have greater regenerative properties. After reviewing the literature, two systematic review articles on periodontal regeneration with MSCs published by Tassi et al. [49] and Yan et al. [50] were found. In the first study, the meta-analysis was not possible because of the heterogeneities observed in the study designs. In the second study, the meta-analysis showed no statistically significant differences in effect between PDLSCs and BMScs.
An ideal bone graft substitute must have certain properties, which include osteoconduction, osteoinduction, osteoincorporation, osteointegration, and osteogenesis [51]. Despite several efforts to invent and characterize various bone graft substitutes, none of these could be accepted as an ideal alternative to autografts due to the low ability of the bone substitutes to enhance osteoinduction and osteogenesis [52, 53]. The majority of in vitro and many in vivo studies have suggested that the MSCs have the potential to increase osteoinduction and osteogenesis [46], in particular in association with bone substitute materials [41]. The use of β-TCP is applicable as a scaffold for BMSC transplantation and it helps to augment alveolar bone without affecting cementum regeneration [46].
The regenerative potential of MSCs is probably related predominantly to the stage of differentiation and lineage commitment of the cells, as well as proliferation rates, heterogeneity of selectively isolated MSCs subpopulations, the number of cells transferred to the defects and the scaffold composition and three-dimensional arrangement [54, 55].The origin of stem cells and the role these play in the regenerative processes has been the subject of much debate, sometimes with contradictory results. Nagahara et al. [46] demonstrated that periodontal regeneration with BMSCs with beta-tricalcium phosphate was enhanced at 8 weeks in alveolar cementum and alveolar bone. Nevertheless, Iwasaki et al. [44] determined that there was a considerable significant difference in periodontal regeneration in PDLSCs with beta-tricalcium phosphate and collagen compared to the BMSCs.
Bone regeneration by gene transfer into MSCs has also been reported; however, the reported transduction efficiency into MSCs by each vector was not always high. Chung et al. [31] indicated that when using MSCs with adenovirus BMP-2 (advBMP-2) in bone defects, the periodontal regeneration was significantly better at 8 weeks than in the control group. Other studies have indicated that PDLSCs, have the same results [32, 34, 39] without needing to use viral vectors. Fawzy El-Sayed et al. [33] used gingival margin stem progenitor cells (GMSCs) together with IL-1ra-releasing hyaluronic acid synthetic extracellular matrix (HA-sECM), and they concluded that there was a significant periodontal regenerative potential compared to the control groups. On the other hand, in the case of platelet-rich plasma with MSCs and autologous bone, there was no significant difference between the platelet-rich plasma alone and the autologous bone group [38]. Chondrogenic differentiation of MSCs before implantation is also a useful strategy for the regeneration of the cartilage; however, its role in alveolar bone and periodontal ligament regeneration is still not clear [45].
The main limitations of this research were related to the design of the experiments (different and non-equitable groups), the different types of animal model (dog, pig, and rat), the high variability of MSCs, and the different methodology used to apply the cells, whether alone or in combination with many different types of biomaterials.
In the present study, there were significant differences in the use of MSCs compared to the group of other biomaterials for periodontal regeneration. The most commonly used stem cells were periodontal ligament and bone marrow stem cells, and these cells were mixed with other regenerative biomaterials, obtaining better results in periodontal regeneration. Taking into account the results attained from the meta-analyses, it is possible to conclude that stem cells have a higher periodontal regenerative capacity than other single regenerative materials.
References
Balta MG, Papathanasiou E, Blix IJ, Van Dyke TE. Host modulation and treatment of periodontal disease. J Dent Res. 2021;100(8):798–809. https://doi.org/10.1177/0022034521995157.
Nazir M, Al-Ansari A, Al-Khalifa K, Alhareky M, Gaffar B, Almas K. Global prevalence of periodontal disease and lack of its surveillance. Sci World J. 2020. https://doi.org/10.1155/2020/2146160.
Hernández-Monjaraz B, Santiago-Osorio E, Ledesma-Martínez E, Aguiñiga-Sánchez I, Sosa-Hernández NA, Mendoza-Núñez VM. Dental pulp mesenchymal stem cells as a treatment for periodontal disease in older adults. Stem Cells Int. 2020. https://doi.org/10.1155/2020/8890873.
Liu Y, Wang H, Dou H, Tian B, Li L, Jin L, et al. Bone regeneration capacities of alveolar bone mesenchymal stem cells sheet in rabbit calvarial bone defect. J Tissue Eng. 2020. https://doi.org/10.1177/2041731420930379.
Tetè G, D’Orto B, Nagni M, Agostinacchio M, Polizzi E, Agliardi E. Role of induced pluripotent stem cells (IPSCS) in bone tissue regeneration in dentistry: a narrative review. J Biol Regul Homeost Agents. 2020;34:1–10.
Abou Neel EA, Bozec L, Knowles JC, Syed O, Mudera V, Day R, et al. Collagen–emerging collagen based therapies hit the patient. Adv Drug Deliv Rev. 2013;65:429–56. https://doi.org/10.1016/j.addr.2012.08.010.
Chen F, Gao L, Tian B, Zhang X, Zhang Y, Dong G, et al. Treatment of periodontal intrabony defects using autologous periodontal ligament stem cells: a randomized clinical trial. Stem Cell Res Ther. 2016. https://doi.org/10.1186/s13287-016-0288.
Botelho J, Cavacas MA, Machado V, Mendes JJ. Dental stem cells: recent progresses in tissue engineering and regenerative medicine. Ann Med. 2017;49:644–51. https://doi.org/10.1080/07853890.2017.1347705.
Rodríguez-Lozano F, Insausti C, Iniesta F, Blanquer M, Ramírez M, Meseguer L, et al. Mesenchymal dental stem cells in regenerative dentistry. Med Oral Patol Oral Cir Bucal. 2012. https://doi.org/10.4317/medoral.17925.
Ferrarotti F, Romano F, Gamba MN, Quirico A, Giraudi M, Audagna M, et al. Human intrabony defect regeneration with micrografts containing dental pulp stem cells: a randomized controlled clinical trial. J Clin Periodontol. 2018;45:841–50. https://doi.org/10.1111/jcpe.12931.
Hazeltine LB, Selekman JA, Palecek SP. Engineering the human pluripotent stem cell microenvironment to direct cell fate. Biotechnol Adv. 2013;31:1002–19. https://doi.org/10.1016/j.biotechadv.2013.03.002.
Naji A, Eitoku M, Favier B, Deschaseaux F, Rouas-Freiss N, Suganuma N. Biological functions of mesenchymal stem cells and clinical implications. Cell Mol Life Sci. 2019;76:3323–48. https://doi.org/10.1007/s00018-019-03125-1.
Huang GT, Gronthos S, Shi S. Mesenchymal stem cells derived from dental tissues vs. those from other sources: their biology and role in regenerative medicine. J Dent Res. 2009;88:792–806.
Bianchi S, Torge D, Rinaldi F, Piattelli M, Bernardi S, Varvara G. Platelets’ role in dentistry: from oral pathology to regenerative potential. Biomedicines. 2022. https://doi.org/10.3390/biomedicines10020218.
Buduru SD, Gulei D, Zimta A, Tigu AB, Cenariu D, Berindan-Neagoe I. The potential of different origin stem cells in modulating oral bone regeneration processes. Cells. 2019;8(1):29.
Gonzalez-Vilchis RA, Piedra-Ramirez A, Patiño-Morales CC, Sanchez-Gomez C, Beltran-Vargas NE. Sources, characteristics, and therapeutic applications of mesenchymal cells in tissue engineering. Tissue Eng Regen Med. 2022;19(2):325–61.
Chen F, Sun H, Lu H, Yu Q. Stem cell-delivery therapeutics for periodontal tissue regeneration. Biomaterials. 2012;33:6320–44. https://doi.org/10.1016/j.biomaterials.2012.05.048.
Bianchi S, Mancini L, Torge D, Cristiano L, Mattei A, Varvara G, et al. Bio-morphological reaction of human periodontal ligament fibroblasts to different types of dentinal derivates: in vitro study. Int J Mol Sci. 2021;22(16):8681. https://doi.org/10.3390/ijms22168681.
Novello S, Debouche A, Philippe M, Naudet F, Jeanne S. Clinical application of mesenchymal stem cells in periodontal regeneration: a systematic review and meta-analysis. J Periodontal Res. 2020;55:1–12. https://doi.org/10.1111/jre.12684.
Hynes K, Menicanin D, Gronthos S, Bartold PM. Clinical utility of stem cells for periodontal regeneration. Periodontol. 2012;59:203–27.
Chen F, Jin Y. Periodontal tissue engineering and regeneration: current approaches and expanding opportunities. Tissue Eng Part B Rev. 2010;16:219–55.
Iohara K, Zheng L, Ito M, Tomokiyo A, Matsushita K, Nakashima M. Side population cells isolated from porcine dental pulp tissue with self-renewal and multipotency for dentinogenesis, chondrogenesis, adipogenesis, and neurogenesis. Stem Cells. 2006;24:2493–503.
Zhou S, Schuetz JD, Bunting KD, Colapietro AM, Sampath J, Morris JJ, et al. The ABC transporter Bcrp1/ABCG2 is expressed in a wide variety of stem cells and is a molecular determinant of the side-population phenotype. Nat Med. 2001;9:1028–34. https://doi.org/10.1038/nm0901-1028.
Dhote R, Charde P, Bhongade M, Rao J. Stem cells cultured on beta tricalcium phosphate (β-TCP) in combination with recombinant human platelet-derived growth factor—BB (rh-PDGF-BB) for the treatment of human infrabony defects. J Stem Cells. 2015;10:243–54.
Chen F, Gao L, Tian B, Zhang X, Zhang Y, Dong G, et al. Treatment of periodontal intrabony defects using autologous periodontal ligament stem cells: a randomized clinical trial. Stem Cell Res Ther. 2016;7:33.
Sánchez N, Fierravanti L, Núñez J, Vignoletti F, González-Zamora M, Santamaria S, et al. Periodontal regeneration using a xenogeneic bone substitute seeded with autologous periodontal ligament-derived mesenchymal stem cells: A 12-month quasi-randomized controlled pilot clinical trial. J Clin Periodontol. 2020. https://doi.org/10.1111/jcpe.13368.
Abdal-Wahab M, Abdel GKA, Ezzatt OM, Hassan AAA, Ansary EL, Mervat MS, Gamal AY. Regenerative potential of cultured gingival fibroblasts in treatment of periodontal intrabony defects (randomized clinical and biochemical trial). J Periodontal Res. 2020;55:441–52.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339: b2700.
Hooijmans CR, Rovers MM, de Vries RBM, Leenaars M, Ritskes-Hoitinga M, Langendam MW. SYRCLE’s risk of bias tool for animal studies. BMC Med Res Methodol. 2014;14:43. https://doi.org/10.1186/1471-2288-14-43.
Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health. 2019;22:153–60. https://doi.org/10.1136/ebmental-2019-300117.
Chung VH, Chen AY, Kwan C, Chen PK, Chang SC. Mandibular alveolar bony defect repair using bone morphogenetic protein 2-expressing autologous mesenchymal stem cells. J Craniofac Surg. 2011;22:450–4. https://doi.org/10.1097/SCS.0b013e3182077de9.
Tsumanuma Y, Iwata T, Washio K, Yoshida T, Yamada A, Takagi R, et al. Comparison of different tissue-derived stem cell sheets for periodontal regeneration in a canine 1-wall defect model. Biomaterials. 2011;32:5819–25. https://doi.org/10.1016/j.biomaterials.2011.04.071.
Fawzy El-Sayed KM, Mekhemar MK, Beck-Broichsitter BE, Bähr T, Hegab M, Receveur J, et al. Periodontal regeneration employing gingival margin-derived stem/progenitor cells in conjunction with IL-1ra-hydrogel synthetic extracellular matrix. J Clin Periodontol. 2015;42:448–57. https://doi.org/10.1111/jcpe.12401.
Han J, Menicanin D, Marino V, Ge S, Mrozik K, Gronthos S, et al. Assessment of the regenerative potential of allogeneic periodontal ligament stem cells in a rodent periodontal defect model. J Periodontal Res. 2014;49:333–45. https://doi.org/10.1111/jre.1211.
Duan X, Tu Q, Zhang J, Ye J, Sommer C, Mostoslavsky G, et al. Application of induced pluripotent stem (iPS) cells in periodontal tissue regeneration. J Cell Physiol. 2011;226:150–7. https://doi.org/10.1002/jcp.22316.
Suaid FF, Ribeiro FV, Rodrigues TL, Silvério KG, Carvalho MD, Nociti FH, et al. Autologous periodontal ligament cells in the treatment of class II furcation defects: a study in dogs. J Clin Periodontol. 2011;38:491–8. https://doi.org/10.1111/j.1600-051X.2011.01715.x.
Nuñez J, Sanz-Blasco S, Vignoletti F, Muñoz F, Arzate H, Villalobos C, et al. Periodontal regeneration following implantation of cementum and periodontal ligament-derived cells. J Periodontal Res. 2012;47:33–44. https://doi.org/10.1111/j.1600-0765.2011.01402.x.
Simsek SB, Keles GC, Baris S, Cetinkaya BO. Comparison of mesenchymal stem cells and autogenous cortical bone graft in the treatment of class II furcation defects in dogs. Clin Oral Investig. 2012;16:251–8. https://doi.org/10.1007/s00784-010-0486-7.
Suaid FF, Ribeiro FV, Gomes TR, Lopes ES, Silvério KG, Carvalho MD, Nociti FH, et al. Autologous periodontal ligament cells in the treatment of Class III furcation defects: a study in dogs. J Clin Periodontol. 2012;39:377–84. https://doi.org/10.1111/j.1600-051X.2012.01858.x.
Zhou W, Mei L. Effect of autologous bone marrow stromal cells transduced with osteoprotegerin on periodontal bone regeneration in canine periodontal window defects. Int J Periodontics Restorative Dent. 2012;32:174.
Khorsand A, Eslaminejad MB, Arabsolghar M, Paknejad M, Ghaedi B, Rokn AR, et al. Autologous dental pulp stem cells in regeneration of defect created in canine periodontal tissue. J Oral Implantol. 2013;39:433–43. https://doi.org/10.1563/AAID-JOI-D-12-00027.
Tobita M, Uysal CA, Guo X, Hyakusoku H, Mizuno H. Periodontal tissue regeneration by combined implantation of adipose tissue-derived stem cells and platelet-rich plasma in a canine model. Cytotherapy. 2013;15:1517–26. https://doi.org/10.1016/j.jcyt.2013.05.007.
Yu X, Ge S, Chen S, Xu Q, Zhang J, Guo H, et al. Human gingiva-derived mesenchymal stromal cells contribute to periodontal regeneration in beagle dogs. Cells Tissues Organs. 2013;198:428–37. https://doi.org/10.1159/000360276.
Iwasaki K, Komaki M, Yokoyama N, Tanaka Y, Taki A, Honda I, et al. Periodontal regeneration using periodontal ligament stem cell-transferred amnion. Tissue Eng Part A. 2014;20:693–704. https://doi.org/10.1089/ten.TEA.2013.0017.
Cai X, Yang F, Yan X, Yang W, Yu N, Oortgiesen DAW, et al. Influence of bone marrow-derived mesenchymal stem cells pre-implantation differentiation approach on periodontal regeneration in vivo. J Clin Periodontol. 2015;42:380–9. https://doi.org/10.1111/jcpe.12379.
Nagahara T, Yoshimatsu S, Shiba H, Kawaguchi H, Takeda K, Iwata T, et al. Introduction of a mixture of β-tricalcium phosphate into a complex of bone marrow mesenchymal stem cells and type I collagen can augment the volume of alveolar bone without impairing cementum regeneration. J Periodontol. 2015;86:456–64. https://doi.org/10.1902/jop.2014.140384.
Paknejad M, Eslaminejad MB, Ghaedi B, Rokn A, Khorsand A, Etemad-Moghadam S, et al. Isolation and assessment of mesenchymal stem cells derived from bone marrow: histologic and histomorphometric study in a canine periodontal defect. J Oral Implantol. 2015;41:284–91. https://doi.org/10.3390/ijms19040944.
Zhang C, Yan B, Cui Z, Cui S, Zhang T, Wang X, et al. Bone regeneration in minipigs by intrafibrillarly-mineralized collagen loaded with autologous periodontal ligament stem cells. Sci Rep. 2017. https://doi.org/10.1038/s41598-017-11155-7.
Tassi SA, Sergio NZ, Misawa MYO, Villar CC. Efficacy of stem cells on periodontal regeneration: systematic review of pre-clinical studies. J Periodontal Res. 2017;52:793–812. https://doi.org/10.1111/jre.12455.
Yan X, Yang F, Jansen JA, de Vries RBM, van den Beucken J, Jeroen JJP. Cell-based approaches in periodontal regeneration: a systematic review and meta-analysis of periodontal defect models in animal experimental work. Tissue Eng Part B Rev. 2015;21:411–26. https://doi.org/10.1089/ten.teb.2015.0049.
Wikesjö UM, Sorensen RG, Wozney JM. Augmentation of alveolar bone and dental implant osseointegration: clinical implications of studies with rhBMP-2. J Bone Joint Surg Am. 2001;83:136.
Xie J, Peng C, Zhao Q, Wang X, Yuan H, Yang L, et al. Osteogenic differentiation and bone regeneration of iPSC-MSCs supported by a biomimetic nanofibrous scaffold. Acta Biomater. 2016;29:365–79. https://doi.org/10.1016/j.actbio.2015.10.007.
Tang M, Chen W, Liu J, Weir MD, Cheng L, Xu HHK. Human induced pluripotent stem cell-derived mesenchymal stem cell seeding on calcium phosphate scaffold for bone regeneration. Tissue Eng Part A. 2014;20:1295–305. https://doi.org/10.1089/ten.TEA.2013.0211.
Harris CT, Cooper LF. Comparison of bone graft matrices for human mesenchymal stem cell-directed osteogenesis. J Biomed Mater Res A. 2004;68:747–55.
Lee YM, Seol YJ, Lim YT, Kim S, Han SB, Rhyu IC, et al. Tissue-engineered growth of bone by marrow cell transplantation using porous calcium metaphosphate matrices. J Biomed Mater Res. 2001;54:216–23.
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature. This study was partly funded by a pre-doctoral grant (on a competitive basis) from the Health Research Institute of Santiago de Compostela that was awarded to Alba Pérez Jardón (IDIS2020/PREDOC/03).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by ITC, FCA and MPS. The first draft of the manuscript was written by LCB and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there are no conflicts of interest regarding the publication of this paper. The authors declare that they have contributed significantly to the preparation of the manuscript and that all authors agree with the content of the manuscript.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Clinical relevance: The MSCs could be effective in the regeneration of human periodontal defects.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chauca-Bajaña, L., Velasquez-Ron, B., Tomás-Carmona, I. et al. Regeneration of periodontal bone defects with mesenchymal stem cells in animal models. Systematic review and meta-analysis. Odontology 111, 105–122 (2023). https://doi.org/10.1007/s10266-022-00725-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10266-022-00725-5