
Abstract
Introduction
Door-to-needle time (DNT) is an established predictor of outcome in acute ischemic stroke (AIS) patients treated with intravenous thrombolysis (IVT). Several strategies have been proposed to streamline in-hospital pathways, among which treatment at CT/MR bed.
Aim
To explore the impact of treatment at CT/MR bed, here defined as imaging area (IA), on functional outcome in stroke patients treated with IVT alone.
Methods
All AIS patients treated with IVT alone at our center in 2020, 2021, and 2022 were included. Patients with any previous disability were excluded. The cohort was divided into two groups, depending on the treatment site. One group received IVT at IA, the other at emergency room or stroke unit (non-IA). Regression analysis assessed the association between treatment site and 3-month outcome.
Results
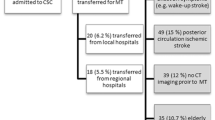
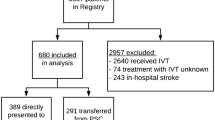
A total of 327 patients who received IVT alone were included in the analysis. One hundred thirty-three (40.7%) were in the IA group and 194 (59.3%) in the non-IA group. The groups showed similar baseline characteristics. In the IA group, DNT was 45 min shorter. Despite similar rates of functional independence (mRS 0-2), the IA group showed higher rates of excellent outcome (mRS 0-1) compared to the non-IA group (60.1% vs 42.8%, p<0.01). Immediate treatment at IA was independently associated to excellent outcome (OR 1.78 [1.03–3.08]).
Conclusions
Thrombolytic treatment at IA lowers DNT and is an independent predictor of excellent outcome after AIS. Our study emphasizes the importance of immediate thrombolytic treatment at IA, soon after radiological eligibility is confirmed. Immediate treatment at IA should be a standard-of-care for AIS.


Similar content being viewed by others

References
Emberson J, Lees KR, Lyden P et al (2014) Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet 384(9958):1929–1935. https://doi.org/10.1016/S0140-6736(14)60584-5
Ahmed N, Wahlgren N, Grond M et al (2010) Implementation and outcome of thrombolysis with alteplase 3-4.5 h after an acute stroke: an updated analysis from SITS-ISTR. Lancet Neurol 9(9):866–874. https://doi.org/10.1016/S1474-4422(10)70165-4
Lin CB, Peterson ED, Smith EE et al (2012) Emergency medical service hospital prenotification is associated with improved evaluation and treatment of acute ischemic stroke. Circ Cardiovasc Qual Outcomes 5(4):514–522. https://doi.org/10.1161/CIRCOUTCOMES.112.965210
Vidale S, Arnaboldi M, Bezzi G et al (2016) Reducing time delays in the management of ischemic stroke patients in Northern Italy. Int J Cardiol 15(215):431–434. https://doi.org/10.1016/j.ijcard.2016.03.232
Candelaresi P, Lattuada P, Uggetti C et al (2017) A high-urgency stroke code reduces in-hospital delays in acute ischemic stroke: a single-centre experience. Neurol Sci 38(9):1671–1676. https://doi.org/10.1007/s10072-017-3046-y
Rost NS, Masrur S, Pervez MA, Viswanathan A, Schwamm LH (2009) Unsuspected coagulopathy rarely prevents IV thrombolysis in acute ischemic stroke. Neurology 73(23):1957–1962. https://doi.org/10.1212/WNL.0b013e3181c5b46d
Xian Y, Smith EE, Zhao X et al (2014) Strategies used by hospitals to improve speed of tissue-type plasminogen activator treatment in acute ischemic stroke. Stroke 45(5):1387–1395. https://doi.org/10.1161/STROKEAHA.113.003898
Siarkowski M, Lin K, Li SS, Al Sultan A, Ganshorn H, Kamal N, Hill M, Lang E (2020) Meta-analysis of interventions to reduce door to needle times in acute ischaemic stroke patients. BMJ Open Qual 9(3):e000915. https://doi.org/10.1136/bmjoq-2020-000915
Berge E, Whiteley W, Audebert H et al (2021) European Stroke Organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur Stroke J 6(1):I-LXII. https://doi.org/10.1177/2396987321989865
Johns H, Campbell B, Turc G, Churilov L (2023) Power analysis for ordinal analyses of the modified Rankin scale and an online and downloadable tool for practical use. Stroke 54(7):1750–1760. https://doi.org/10.1161/STROKEAHA.122.041260
Wahlgren N, Ahmed N, Dávalos A et al (2007) Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST): an observational study. Lancet 369(9558):275–282. https://doi.org/10.1016/S0140-6736(07)60149-4
Ringelstein EB, Chamorro A, Kaste M et al (2013) European Stroke Organisation recommendations to establish a stroke unit and stroke center. Stroke 44(3):828–840. https://doi.org/10.1161/STROKEAHA.112.670430
Powers WJ, Rabinstein AA, Ackerson T et al (2019) Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke 50(12):e344–e418. https://doi.org/10.1161/STR.0000000000000211
Fonarow GC, Smith EE, Saver JL et al (2011) Timeliness of tissue-type plasminogen activator therapy in acute ischemic stroke: patient characteristics, hospital factors, and outcomes associated with door-to-needle times within 60 minutes. Circulation 123(7):750–758. https://doi.org/10.1161/CIRCULATIONAHA.110.974675
Tong X, Wiltz JL, George MG et al (2018) A decade of improvement in door-to-needle time among acute ischemic stroke patients, 2008 to 2017. Circ Cardiovasc Qual Outcomes 11(12):e004981. https://doi.org/10.1161/CIRCOUTCOMES.118.004981
Candelaresi P, Manzo V, Servillo G et al (2021) The impact of Covid-19 lockdown on stroke admissions and treatments in Campania. J Stroke Cerebrovasc Dis 30(1):105448. https://doi.org/10.1016/j.jstrokecerebrovasdis.2020.105448
Thortveit ET, Bøe MG, Ljøstad U, Mygland A, Tveiten A (2014) Organizational changes aiming to reduce iv tPA door-to-needle time. Acta Neurol Scand 130(4):248–252. https://doi.org/10.1111/ane.12204
Galecio-Castillo M, Vivanco-Suarez J, Zevallos CB et al (2022) Direct to angiosuite strategy versus standard workflow triage for endovascular therapy: systematic review and meta-analysis. J Neurointerv Surg 16:neurintsurg-2022-018895. https://doi.org/10.1136/neurintsurg-2022-018895
Gallien P, Gich J, Sánchez-Dalmau BF, Feneberg W (2014) Multidisciplinary management of multiple sclerosis symptoms. Eur Neurol 72(Suppl 1):20–25. https://doi.org/10.1159/000367620
Dehli T, Uleberg O, Wisborg T (2018) Trauma team activation - common rules, common gain. Acta Anaesthesiol Scand 62(2):144–146. https://doi.org/10.1111/aas.13013
Acknowledgements
The authors would like to acknowledge all the professionals involved in stroke care at our hospital, who actively contributed to the improvement of the stroke chain of recovery.
Author information
Authors and Affiliations
Contributions
Drs. De Mase, Spina, and Candelaresi had full access to all data in the study and take responsibility for the integrity of the data.
Concept and design: De Mase, Spina, Candelaresi.
Drafting of the manuscript: De Mase, Spina, Candelaresi. Collection of data: De Mase, Spina, Candelaresi, Servillo, Barbato, Leone, Giordano, Guarnieri, Muto Massimo, Alfieri, Longo, Di Iorio.
Critical revision of the manuscript for important intellectual content: De Mase, Spina, Candelaresi, Servillo, Barbato, Leone, Giordano, Guarnieri, Muto Massimo, Alfieri, Longo, Di Iorio, Muto Mario, Andreone.
Supervision: Candelaresi, Andreone.
Corresponding author
Ethics declarations
Ethical approval
Ethical approval was not sought for the present retrospective study because every patient was treated according to the current standard of care. This study was completed in accordance with the Helsinki Declaration as revised in 2013.
Informed consent
All patients or relatives have given written or verbal consent to the clinical procedures and to inclusion in the internal register for subsequent retrospective analysis.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
ESM 1
(DOCX 17 kb)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
De Mase, ., Spina, E., Servillo, G. et al. Effects of immediate thrombolytic treatment in imaging area on functional outcome in patients with acute ischemic stroke. Neurol Sci 45, 1557–1563 (2024). https://doi.org/10.1007/s10072-023-07166-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-023-07166-0