
Abstract
Background
People often ignore the usefulness of stroke prevention, the typical onset symptoms, and the efficacy of the new therapies. In order to attempt to correct this situation, we performed a wide educational campaign addressed to students of high schools in Liguria and Piedmont Italian regions.
Method
The campaign consisted in two phases: (1) compilation of a simple questionnaire on stroke, followed by a scientific lecture on the disease, distribution of didactic materials, and final open discussion; (2) re-filling and sending by participants of the same questionnaire for the statistical evaluation of the improvement of stroke awareness.
Results
The global initial percentage of wrong answers (number of subjects 2,264) was 33.4%: (A) stroke general knowledge 23.5%, (B) stroke risk factors 37.6%, (C) stroke early symptoms 34.1%). At the end of the campaign, the total percentage of wrong answers (number of subjects 1883) attained the 11.4%.: (A) stroke general knowledge 3.7%, (B) stroke risk factors 11.7%, (C) stroke early symptoms 12.5%). All these differences were strongly significant.
Discussion and conclusion
We demonstrated that our educational campaign obtained an important improvement of stroke awareness in our sample. Girl students, Lyceum students, and less young students attained significant better knowledge improvement. We hope that the enhanced awareness might induce a more frequent diffusion of prevention strategies, an increased capacity of recognizing onset stroke symptoms with shortening of patients’ presentation in the emergency room of the hospitals when they can undergo reperfusion treatments.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Stroke is the second leading cause of death and dementia and one of the major causes of disability in the world [1, 2]. Despite the worldwide increasing possibility of very useful treatments of the hyperacute phase of the ischemic forms of the disease, by reperfusion strategies [3, 4], the awareness in the general population of symptoms and signs of stroke is still quite low [5,6,7,8]. Moreover, the well-known efficacy of primary stroke prevention through modifications and treatments of risk factor is not yet spread in the general population nor the need to carefully follow treatments of causal stroke mechanisms in reducing the stroke recurrence rate in secondary prevention [9].
Thus, many subjects with new onset stroke often attain the hospital emergency room too late for getting advantage from revascularization therapies and a large amount of people at stroke risk are not acquainted with the situation and do not adopt a healthy life style nor correct avoidable risk factors [10,11,12,13,14]. Moreover, many patients who survived their stroke do not follow prescribed treatments nor change their non-healthy life-style in order to avoid recurrence of the disease [15, 16]. Finally, many stroke patients are not admitted to a stroke-unit, one of the best factors linked with prognosis improvement [17], even if available in the living area.
Several worldwide surveys demonstrated that the knowledge of typical stroke presentation symptoms, of principles of stroke prevention, and of the need of a prompt hospital admission, in case of stroke, are strongly lacking in many countries, including Italy, even in people with high level of education [6,7,8,9,10]. Educational campaigns can improve stroke knowledge in the population, enhance prevention, improve correct symptoms’ recognition, and timely care response [18,19,20,21,22,23].
A group of vascular neurologists organized a survey named “PRESTO” (Italian translation of “FAST” acronym [24]) in Liguria (Italy) to spread easy and clear messages regarding the stroke prevention strategies as well as the correct management of the acute phase of the disease.
Educational material (leaflets, videos, radio broadcasts, and social media messages) was disseminated to educate people to prevent stroke, to be able to recognize the early stroke signs, and to call the emergency medical services as soon as stroke symptoms appear.
We are aware that school-based education pertaining to lifestyle-related diseases can help in preventing diseases like stroke. Moreover, we know that educated family members will act appropriately by calling emergent medical services in the event of a suspected stroke [25,26,27,28].
Based on these considerations, we organized a wide educational campaign on stroke awareness in several high schools involving more than 2500 students and the results of this part of the “PRESTO” project [29] are the object of the present report. The list of the 19 involved high school institutes for 33 didactic sessions, as well as the number of participant students of each school, and the school location is available in Table 1.
The Liguria and the Piedmont School Regional Directions (Direzioni Scolastiche Regionali della Liguria e del Piemonte) approved the project named “Know stroke in order to improve its prevention and treatment” (English translation of: “Conoscere l’ictus per meglio prevenirlo e curarlo”).
Rotary District 2032 (including Liguria and Piedmont southern part) of Rotary International (https://www.rotary.org) and A.L.I.Ce. Liguria ODV (Associazione per la Lotta all’Ictus Cerebrale della Liguria: Association for the fight against Stroke of the Liguria; http://liguria.aliceitalia.org) gave an unconditioned support for the campaign in high schools.
Rotary International is a service organization present in more than 200 nations whose stated purpose is to bring together business and professional leaders in order to provide humanitarian service and to advance goodwill and peace around the world (https://www.rotary.org). Two of the seven Rotarian main objectives are health promotion in the population and improvement of educational in young people.
A.L.I.Ce. Liguria ODV is the local session of A.L.I.Ce. Italia ODV (https://www.aliceitalia.org/), an Italian very large organization of voluntaries against stroke, with more than 80 centers in all Italian regions, several thousand members, and associated with SAFE (Stroke Alliance for Europe: https://www.safestroke.eu/), which support many initiatives for contrast the harmful effect of the disease.
We performed and already published the results, a similar project addressed to Rotarians members and their friends and relatives a few years ago [30].
The high school project on stroke awareness started at the beginning of 2019 but the COVID-19 pandemic caused a 2-year arrest of the survey which restarted only at the end of 2021 and finished in April 2022.
Methods
The organization of the survey foresaw two main steps:
-
(1)
First step: The participant students have been invited to fill in a simple anonymous questionnaire, with multiple possible answers, on stroke general knowledge (Section A), stroke risk factors (Section B), and stroke early symptoms (Section C). The questionnaire is visible in the supplemental material (Addendum n° 1). After the compilation, one of the vascular neurologist promotors of the campaign (CG, FA) presented a simplified, but scientifically correct, lecture on stroke prevention, treatment, and early symptoms, including the correct answers to the questionnaire. An open and friendly discussion on the topic followed the presentation.
-
(2)
Second step: After lecture and discussion, the speaker distributed another copy of the questionnaire, identical to the previous one, and a didactic pamphlet on stroke, asking all listeners to read the pamphlet the following few days for deepening the topic, and, finally, to re-fill in the questionnaire. The students sent the second questionnaire, by electronic mail or by post, anonymously, to the speaker, in order to allow the objective quantification of the expected improvement of stroke knowledge.
In order to respect the privacy rules, we recorded only age, gender, and type of school (Lyceum or Technical Institute) of the students who attended the formative sessions and filled in the two questionnaires.
We compared the proportions of correct and wrong answers of the first and of the second questionnaires (first and second study phases). In mean comparisons, we used T-Test for unpaired data. In proportion comparisons, we used the chi2 test with Yates’ correction.
We also performed a multivariate analysis on independent factors causing higher proportion of correct answers to the questionnaire (multiple logistic regression) using the following binary cutoffs: (a) age (less and equal or more than the median value), (b) gender (male, female), and (c) school type (Lyceum or Technical Institute). We always considered statistically significant the P values less than 5%. We used for all statistics the program StatView.
Results
The number of students attending the first phase of the educational campaign who filled in the first questionnaire was 2264, with mild female predominance (1293 females, 57.1% vs. 971 males, 42.9%). The mean age (± sd) was 17.72 (± 3.29) years. The median age was 17 years. The age ranged between 13 and 22 years. The school type was Lyceum for 914 students (40.4%) and Technical Institute for the remaining 1350 ones (59.6%).
The number of students who filled in the second questionnaire was 1883, with a satisfactory 83.2% global recompilation rate. Females remained prevalent (1064 females, 56.6% vs. 817 males, 43.4%). The mean age (± sd) was 17.77 (± 2.95) years; the median age value was 17 years; the age ranged between 13 and 22 years.
Table 2 reports the main characteristics of these two groups. We did not observe any significant difference in relation to age and gender between the students involved in the survey comparing the first and the second step, but significantly, more Lyceum students completed the second step (recompilation of the questionnaire) than Technical Institute ones.
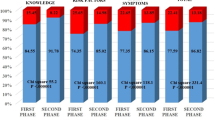
At the first phase of the campaign, the global percentage of wrong answers was 33.4; in particular, being the proportions of errors the following: (A) stroke general knowledge = 23.5, (B) stroke risk factors = 37.6, (C) stroke early symptoms = 34.1.
At the end of the campaign (second phase), the total percentage of wrong answers strongly lowered attaining 11.4; the proportions of errors were as follows: (A) stroke general knowledge = 3.7, (B) stroke risk factors = 11.7; (C) stroke early symptoms = 12.5.
All the differences of these three question subsets between the first and the second phase were strongly significant at the statistical univariate analysis (P < 0.00001) (Fig. 1). We reported the complete description of the results in Table 3.

Univariate statistic comparison (chi2 test with Yates’ correction) of correct versus wrong answers to the three main question subsets of the questionnaire in the two steps of the survey
In the separate analysis of proportions of correct versus wrong answers at each item of the questionnaire, all differences remained statistically significant, with a clear improvement in stroke awareness, with the exception of two items on “difficulty in moving both legs” and “sudden high fever” in stroke early symptoms subset C. In fact, both these two items attained a very high proportion of correct answers already in the first phase of the campaign, before the didactic sessions, so the improvement in the second phase could not reach the statistical significance.
We performed a multivariate analysis on the available factors (age, gender, and school type) in order to evaluate those that independently influenced the correct answer proportion, in the first as well as in the second study phase by multiple logistic regression.
In the first phase, older age (more than the median value) and female gender were statistically associated with a higher proportion of correct answers. Technical Institutes had a lower rate of correct answers in comparison with Lyceums.
In the second phase, these differences remained, even if the significance of older versus younger age was quite lower. Table 4 summarizes these results.
Discussion
We demonstrate that, with a careful, complete, and scientifically correct approach, it is possible to largely improve stroke awareness in a group of motivated high school students.
The sample we analyzed demonstrated also a good pre-existing knowledge on stroke, better than the one demonstrated in the study on a representative sample of general Italian population, published by Baldereschi and co-workers a few years ago [6].
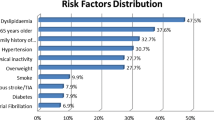
The higher percentage of mistakes was, in stroke general knowledge (Section A of the questionnaire), on the beneficial role of the new acute reperfusion treatments (45.4). In the Section B of the questionnaire (stroke risk factors), the proportion of wrong answers was very high in the items “atrial fibrillation” (58.4%) and “diabetes” (66.1%). Finally, in the last part of the questionnaire, on stroke early symptoms (Section C), many subjects ignored that a “sudden visual disturbance or diplopia” (47.5%) and a “sudden very strong unusual headache” (48.8%) may be prodromal stroke symptoms. On the other hand, many students (48.7%) erroneously believed that a sudden loss of consciousness might be a common initial sign of stroke. Moreover, only 41.9% of our sample knew that a “sudden strength reduction of ipsilateral arm and leg” is one of the most frequent stroke symptoms. All these previous mistaken beliefs significantly regressed after the didactic sessions and the discussion.
The proportion of wrong answers did not significantly lowered in the second phase questionnaire, in comparison with the first one, only in two items, in particular, in the questions on “difficulty in moving both legs” and “sudden high fever” in the section dealing with stroke early symptoms.
We believe that this apparent lack of significant improvement depended by the already very low error rate in the first questionnaire for the item “sudden high fever,” and by the comprehensible possible confusion, in young people, between the not simple concepts of “sudden walking difficulty due to incoordination” and “difficulty of moving both legs” as initial stroke symptoms.
In the first phase of the study, the results were better in students attending Lyceum in comparison with those attending Technical Institute. The difference remained unchanged in the second part of the study. Moreover, the completion rate of the second questionnaire was significantly higher in Lyceum students.
The students attending Lyceum usually go on with university level of education, while Technical Institutes have, in Italy, overall professional purpose and their students more often search for a job just after school, even if the access to university is possible in any case.
In both types of school, the girls attained significantly better results than boys, in the first phase questionnaire, and this difference remained significant after the formative session. The vascular neurologists who performed the scientific lecture observed a higher interest in the topic by girl students and many of them declared, during the discussion, the intention to attain medical professions after the conclusion of high school cycle. This is in line with the reported strong tendency to feminization of the medical professions in several countries [31,32,33,34,35].
In Italy, findings available on the ALMALAUREA website (a public organization of the Italian Ministry of Education which depicts the situation of Italian Universities [36]) confirmed this tendency. In first-level university courses, women constitute, in Italy, a marked majority in health related degrees (74.4%).
In conclusion, we obtained a very important improvement of stroke awareness in our sample, with particular relevance on the role of “thrombolysis/thrombectomy” (Section A) with 39% error rate reduction on “atrial fibrillation” and “diabetes” as risk factors (Section B), with − 33.9% and − 56.5% error rate, respectively, on “sudden strength reduction of ipsilateral arm and leg” and “sudden visual loss or diplopia” as prodromal symptoms (Section C), with − 36.1% and − 36.4% error rate, respectively.
Our group obtained similar results in two recently published reports on campaigns centered on stroke awareness performed in La Spezia, Italy, addressed to general population [37], and in the Rotary Clubs of the North Western Italian Rotary District 2032 [30].
We hope that the enhanced awareness might induce a more frequent diffusion of prevention strategies, an increased capacity of recognizing onset stroke symptoms with shortening of patients’ presentation time in emergency room of our hospitals when they can undergo thrombolysis/thrombectomy, even if other Italian campaigns failed to obtain this result [38].
We observed, after the global campaign “PRESTO” [29], a significant mild average reduction of onset-to-door time (less 33 min) in ischemic stroke patients and a slight increase in the number of patients who arrived to hospitals with milder symptoms and transient ischemic stroke (TIA), in comparison to the same period before the campaign. We hope that our educational campaign in high schools might have contributed to these encouraging results.
Our study has some specific limitations and strengths. The main limitation was that the group of selected subjects was, in comparison to the general population, much younger, with higher female prevalence, and with higher educational level. In effect, the results of our survey could not be generalized to the global Italian population. Another limit was that the percentage of the second phase-recompiled questionnaires was 83.2 of the previous first phase ones. We can speculate that only more motivated students completed the survey, introducing a selection bias that may have caused an overvaluation of the awareness improvement. Finally, we could not perform an analysis of awareness improvement in each participant, being the questionnaires anonymous, but only a global evaluation. Nevertheless, a very high number of subjects were involved with consequent large diffusion of the messages on the efficacy of stroke prevention and on the need to be able to recognize early onset stroke symptoms. Finally, the accurate evaluation of the results was, in our opinion, a commendable aspect, in a field often lacking of a scientific approach.
References
WHO (2022). Accessed 13–06–2022. https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
Virani SS, Alonso A, Benjamin EJ, et al (2020). American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2020 update: a report from the American Heart Association. Circulation 2020;141:e139–596. PMID:31992061. https://doi.org/10.1161/CIR.0000000000000757.
Roaldsen MB, Jusufovic M, Berge E, Lindekleiv H (2021). Endovascular thrombectomy and intra-arterial interventions for acute ischaemic stroke. Cochrane Database Syst Rev. 2021;6:CD007574. https://doi.org/10.1002/14651858.CD007574.pub3.
Powers WJ, Rabinstein AA, Ackerson T, et al (2018). American Heart Association Stroke Council. 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke;49:e46–110. PMID:29367334. https://doi.org/10.1161/STR.0000000000000158.
Baldereschi M, Di Carlo A, Vaccaro C, Polizzi B, Inzitari D (2020) For the promotion implementation of Stroke Care in Italy Project Working Group 2015 Stroke knowledge in Italy. Neurol Sci 36:415-421
Han CH, Kim H, Lee S, Chung JH (2019). Knowledge and poor understanding factors of stroke and heart attack symptoms. Int J Environ Res Public Health;16:3665. https://doi.org/10.3390/ijerph16193665
Stack K, Robertson W, Blackburn C (2020) Does socioeconomic position affect knowledge of the risk factors and warning signs of stroke in the WHO European region? A systematic literature review. BMC Public Health 20:1473–1485. https://doi.org/10.1186/s12889-020-09580-x
Krishnamurthi RV, Barker-Collo S, Barber PA (2020) Community knowledge and awareness of stroke in New Zealand. J Stroke Cerebrovas Dis 29:104589. https://doi.org/10.1016/j.jstrokecerebrovasdis.2019.104589
O’Donnell MJ, Chin SL, Rangarajan S et al (2016) Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet 388(10046):761–775
Patel A, Fang J, Gillespie C, et al (2019). Awareness of stroke signs and symptoms and calling 9–1–1 among US adults: National Health Interview Survey, 2009 and 2014. Prev Chronic Dis;16:180564. PMID:31228234. https://doi.org/10.5888/pcd16.180564
Ruiz RG, Fernández JS, Ruiz RMG et al (2018) Response to symptoms and prehospital delay in stroke patients. Is it time to reconsider stroke awareness campaigns? J Stroke Cerebrovas Dis 27:625–632. https://doi.org/10.1016/j.jstrokecerebrovasdis.2017.09.036
Fladt J, Meier N, Thilemann S et al (2019) Reasons for prehospital delay in acute ischemic stroke. J Am Heart Assoc 8:e013101. https://doi.org/10.1161/JAHA.119.013101
Wang P-Y, Tsao L-I, Chen Y-W, Lo Y-T, Sun H-L (2021) Hesitating and puzzling: the experiences and decision process of acute ischemic stroke patients with prehospital delay after the onset of symptoms. Healthcare 9:1061. https://doi.org/10.3390/healthcare9081061
Amtoft AC, Danielsen AK, Hornnes N, Kruuse C (2021) A qualitative inquiry into patient reported factors that influence time from stroke symptom onset to hospitalization. J Neurosci Nurs 53:5–10. https://doi.org/10.1097/JNN.0000000000000557
Boden-Albala B, Carman H, Moran M, Doyle M, Paik MC (2011) Perception of recurrent stroke risk among black, white and Hispanic ischemic stroke and transient ischemic attack survivors: the SWIFT study. Neuroepidemiology 37(2):83–87
Bai F, Chen J, Pandey D et al (2021) Stroke risk factor status and use of stroke prevention medications Among Hispanic/Latino adults in HCHS/SOL. Stroke 52:1339–1346. https://doi.org/10.1161/STROKEAHA.120.031216
Langhorne P, Ramachandra S (2020) Organised inpatient (stroke unit) care for stroke: network meta-analysis. Cochrane Database Syst Rev (4):CD000197. https://doi.org/10.1002/14651858.CD000197.pub4.
Advani R, Naess H, Kurz M (2016) Mass media intervention in western Norway aimed at improving public recognition of stroke, emergency response, and acute treatment. J Stroke Cerebrovas Dis 25:1467–1472. https://doi.org/10.1016/j.jstrokecerebrovasdis.2016.02.026
Folyovich A, Biczó D, Béres-Molnár KA, Toldi G (2018) Assessment of the efficiency of stroke awareness campaigns in Hungary. J Stroke Cerebrovas Dis 27:1770–1774. https://doi.org/10.1016/j.jstrokecerebrovasdis.2018.02.006
Bray JE, Finn J, Cameron P et al (2018) Temporal trends in emergency medical services and general practitioner use for acute stroke after Australian public education campaigns. Stroke 49:3078–3080. https://doi.org/10.1161/STROKEAHA.118.023263
Gordon C, Bell R, Ranta A (2019) Impact of the national public “FAST” campaigns. NZ Med J 132:48–56
Haesebaert J, Laude C, Termoz A et al (2020) Impact of a theory-informed and user-centered stroke information campaign on the public’s behaviors, attitudes, and knowledge when facing acute stroke: a controlled before-and-after study. BMC Public Health 20:1712–1721. https://doi.org/10.1186/s12889-020-09795-y
Cao M, Guan T, Han X et al (2021) Impact of a health campaign on Chinese public awareness of stroke: evidence from internet search data. BMJ Open 11:e054463. https://doi.org/10.1136/bmjopen-2021-054463
Harbison J, Hossain O, Jenkinson D et al (2003) Diagnostic accuracy of stroke referrals from primary care, emergency room physicians, and ambulance staff using the face arm speech test. Stroke 34:71–76
Miyashita F, Yokota C, Nishimura K et al (2014) The effectiveness of a stroke educational activity performed by a schoolteacher for junior high school students. J Stroke Cerebrovasc Dis 23:1385–1390
Amano T, Yokota C, Sakamoto Y et al (2014) Stroke education program of act FAST for junior high school students and their parents. J Stroke Cerebrovasc Dis 23:1040–1045
Matsuzono K, Yokota C, Takekawa H et al (2015) Effects of stroke education of junior high school students on stroke knowledge of their parents: Tochigi project. Stroke 46:572–574
Ohyama S, Yokota C, Miyashita F et al (2015) Effective education materials to advance stroke awareness without teacher participation in junior high school students. J Stroke Cerebrovasc Dis 24:2533–2538
Gandoglia I, Schirinzi E, Reale N, et al (2022). The PRESTO study: symptom awareness and time from onset to intervention. Neurological Sciences, in press.
Gandolfo C, Alberti F, Del Sette M et al (2020) Results of an educational campaign on stroke awareness in the 2032 Rotary District in Northern-Western Italy. Neurol Sci 41:411–416. https://doi.org/10.1007/s10072-019-04126-5
Alers M, van Leerdam L, Dielissen P, Lagro-Janssen A (2014) Gendered specialities during medical education: a literature review. Perspect Med Educ 3:163–178. https://doi.org/10.1007/s40037-014-0132-1
Bleakley A (2017) Force and presence in the world of medicine. Healthcare 5:58–66. https://doi.org/10.3390/healthcare5030058
Laurence D, Görlich Y, Simmenroth A (2020) How do applicants, students and physicians think about the feminisation of medicine? - a questionnaire-survey. BMC Med Educ 20:48. https://doi.org/10.1186/s12909-020-1959-2
Bardoel EA, Russell G, Advocat J et al (2020) Turnover among Australian general practitioners: a longitudinal gender analysis. Hum Resour Health 18:99. https://doi.org/10.1186/s12960-020-00525-4
Ijaz N, Welsh S, Zhang Q et al (2021) A cross-sectional workforce survey of three traditional and complementary medicine professions in Ontario. Canada PLoS One 16:e0250223. https://doi.org/10.1371/journal.pone.0250223
ALMALAUREA (2022) Accessed: 14–06–2022. https://www.almalaurea.it/sites/almalaurea.it/files/docs/universita/profilo/profilo2021/sintesi_profilo_rapporto_2021_en.pdf
Giorli E, Schirinzi E, Baldi R et al (2019) Planning a campaign to fight stroke: an educational pilot project in La Spezia, Italy. Neurol Sci 40:2133–2140. https://doi.org/10.1007/s10072-019-03963-8
Denti L, Caminiti C, Scoditti U et al (2017) Impact on prehospital delay of a stroke preparedness campaign: a SW-RCT (stepped-wedge cluster randomized controlled trial). Stroke 48:3316–3322
Funding
The project received unconditioned financial support from Rotary International and from A.L.I.Ce. Liguria ODV.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
The Rotary District 2032 Governor, the Rotary District 2032 Health Projects Commission, the Direction Committee of A.L.I.Ce. Liguria ODV, the Liguria and the Piedmont School Regional Directions approved the educational campaign. The authors performed the study in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. The authors omitted any details that might disclose the identity of the subjects under study.
Consent to participate
All recruited persons gave their informed consent prior the inclusion in the study.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gandolfo, C., Alberti, F., Del Sette, M. et al. Stroke prevention and therapy awareness in a large sample of high school students: results of an educational campaign in the Northern-Western Italy. Neurol Sci 43, 6847–6854 (2022). https://doi.org/10.1007/s10072-022-06372-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-022-06372-6